Complete Remission of Recurrent Primary Cutaneous Anaplastic Large Cell Lymphoma Following Bexarotene Therapy: A Case Report
Natsumi Shimada, Natsuko Saito-Sasaki, Hitomi Fujimura, Hikaru Kawahara, Etsuko Okada, Yu Sawada

TL;DR
An elderly man with a rare skin lymphoma achieved full recovery using bexarotene after other treatments failed.
Contribution
This case report demonstrates bexarotene's effectiveness in treating refractory primary cutaneous anaplastic large cell lymphoma.
Findings
Bexarotene treatment led to complete remission in a patient with recurrent pcALCL.
The patient showed resistance to radiotherapy and topical steroids but responded well to bexarotene.
Abstract
Primary cutaneous anaplastic large cell lymphoma (pcALCL) is a CD30-positive cutaneous T-cell lymphoma with a generally favorable prognosis. While radiotherapy is effective, recurrence is not uncommon. Herein, we report the case of an 87-year-old man with recurrent pcALCL who achieved complete remission after bexarotene treatment, despite resistance to radiotherapy and topical steroids. This case highlights bexarotene as a promising therapeutic option for refractory pcALCL. Our experience reinforces the potential of bexarotene as a viable treatment for pcALCL, particularly in recurrent or refractory cases where conventional therapies are contraindicated or ineffective.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
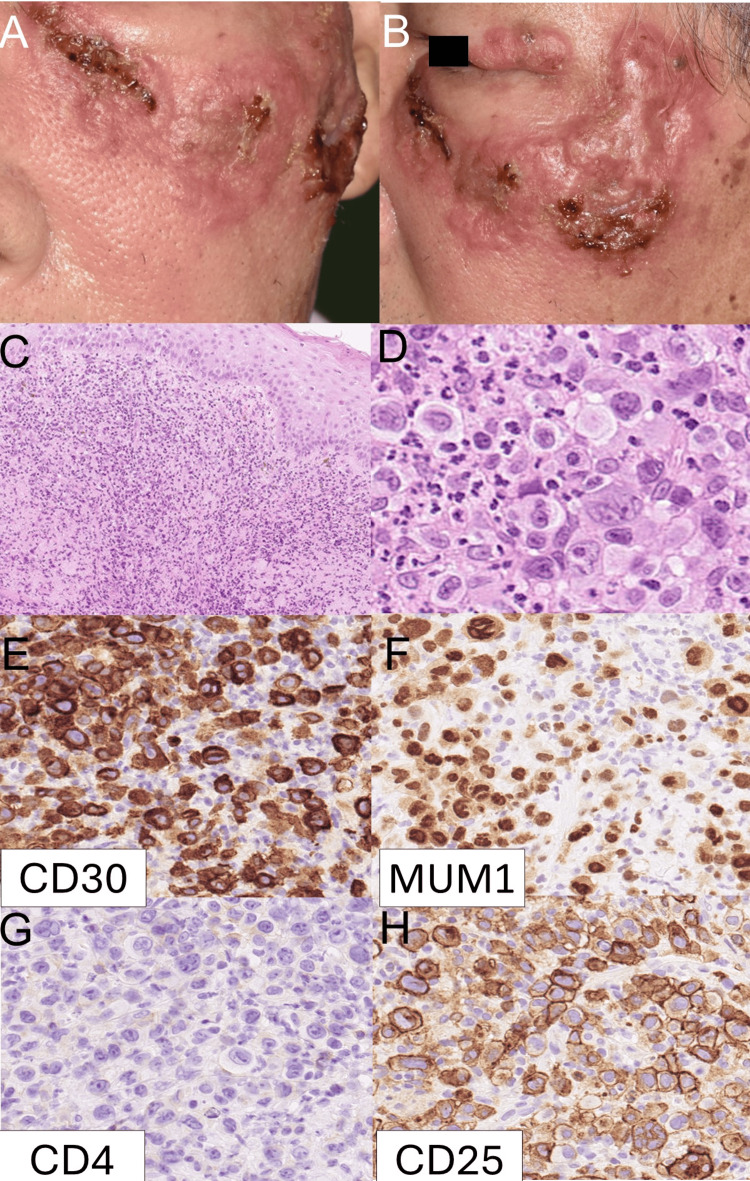 Figure 1
Figure 1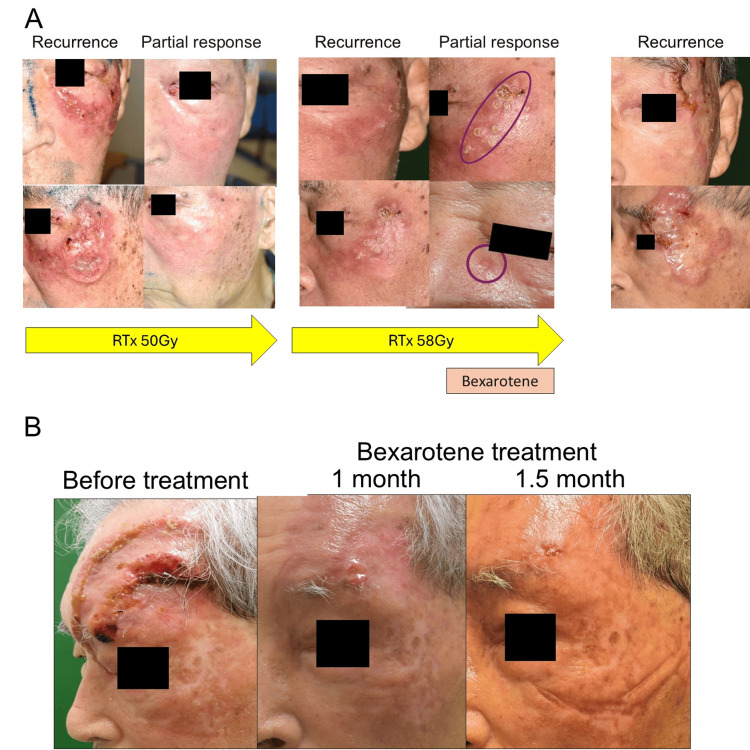 Figure 2
Figure 2| Authors | Age | Gender | Site | Previous treatment | Bexarotene dose | Outcome |
| Sheehy et al. [ | 40 | Female | Face, abdomen, thigh | CHOP chemotherapy | 525 mg | CR |
| Keun et al. [ | 80 | Female | Hand, forearm, leg | Prednisolone, cyclophosphamide, dexamethasone, electrobeam | 300 mg/m2 | CR |
| Ardigò et al. [ | 74 | Male | Face, trunk, extremities | Multiple chemotherapy | 300 mg/m2 | CR |
| Our case | 87 | Male | Face | Radiation | 300 mg/m² → 150 mg/m² | CR |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · CNS Lymphoma Diagnosis and Treatment · Lymphoma Diagnosis and Treatment
Introduction
Primary cutaneous anaplastic large cell lymphoma (pcALCL) is characterized by CD30 expression in more than 75% of tumor cells and is considered part of the spectrum of CD30-positive cutaneous lymphoproliferative disorders [1], in contrast to systemic ALCL, which often presents with nodal or visceral disease. PcALCL generally has a favorable prognosis but may relapse locally. Although pcALCL has a favorable prognosis, with a five-year survival rate exceeding 90%, recurrence can occur in up to 40% of cases following standard therapies such as radiotherapy [2]. Bexarotene, a synthetic retinoid, has shown efficacy in cutaneous T-cell lymphomas [3]. Common adverse effects of bexarotene include hypertriglyceridemia, hypothyroidism, and hepatotoxicity; therefore, regular monitoring of lipid levels, thyroid function, and liver enzymes is recommended during treatment. Reports of its successful use in pcALCL remain limited. We report a refractory case of pcALCL successfully treated with bexarotene.
Case presentation
An 87-year-old man presented with a reddish tumor on his left lower eyelid. Thirteen years earlier, he had been diagnosed with pcALCL on his left cheek and forehead and had achieved complete remission following IFN-γ therapy. At the time of re-presentation, physical examination revealed a solitary erythematous nodule on the left lower eyelid. The lesion was firm, mildly tender, and measured approximately 1.5 cm in diameter. The patient reported no associated pain or systemic symptoms. The lesion rapidly enlarged over the following weeks (Figure 1A, B). A skin biopsy showed large atypical lymphoid cells that were CD30+, CD4+, MUM1+, and CD25+ (Figure 1C-F). The diagnosis was supported by histological features and immunohistochemical markers, including diffuse CD30 positivity in large atypical lymphoid cells and absence of ALK expression, consistent with a diagnosis of pcALCL (T2aN0M0).
Initial clinical, histological, and immunohistochemical findings.(A, B) Clinical photographs at initial presentation showing a reddish tumor on the left lower eyelid. (C, D) Hematoxylin and eosin (HE) staining revealing large atypical lymphoid cells with pleomorphic nuclei. (E–H) Immunohistochemical staining of the tumor cells showing positivity for CD30 (E), CD4 (F), MUM1 (G), and CD25 (H), supporting the diagnosis of pcALCL.
Radiotherapy was initiated with a total dose of 50 Gy; however, the lesion recurred within two weeks after completion (Figure 2A). Despite additional radiotherapy, the tumor relapsed repeatedly, ultimately requiring a cumulative dose of 108 Gy. In light of the treatment resistance, oral bexarotene (525 mg/day) was initiated. The treatment was temporarily interrupted for surgical resection of newly diagnosed colon cancer, during which the tumor showed rapid growth. Given the progression and prior reports of efficacy in cutaneous T-cell lymphomas, oral bexarotene was re-administered. Within weeks, tumor regression was evident, and the lesion continued to shrink steadily. By 1.5 months after treatment initiation, the patient achieved complete clinical remission with no apparent adverse effects related to bexarotene (Figure 2B). The response was assessed by clinical observation and serial photographs, confirming sustained remission for more than six months. Routine laboratory monitoring, including lipid profile and liver function tests, revealed no abnormalities throughout the treatment period.
Clinical course before and after bexarotene treatment.(A) Serial clinical photographs demonstrating the progression and recurrence of the lesion despite corticosteroid therapy and radiotherapy (50 Gy and 58 Gy). (B) Marked tumor regression and complete remission achieved 1.5 months after initiating oral bexarotene.
Discussion
pcALCL is a CD30-positive lymphoproliferative disorder characterized by solitary or localized nodules and tumors, typically showing indolent behavior and a favorable prognosis [4]. Radiotherapy is generally considered one of the first-line treatments for localized disease [5]. In the present case, the patient initially achieved partial remission following radiotherapy but experienced rapid local recurrence shortly thereafter. Despite repeated courses of radiation, the lesion relapsed multiple times, ultimately requiring a cumulative dose of 108 Gy. Given the patient’s advanced age and multiple comorbidities, systemic chemotherapy was deemed high risk.
Bexarotene, a selective retinoid X receptor (RXR) agonist, is approved for cutaneous T-cell lymphomas and modulates gene expression related to differentiation and apoptosis [6]. Although its role in pcALCL is not yet well established, several case reports have indicated potential efficacy in selected cases. In our case, bexarotene was introduced as a systemic treatment. Treatment was temporarily suspended due to the discovery and surgical resection of newly diagnosed colon cancer, during which time the tumor rapidly regrew. Reinitiation of bexarotene led to marked and sustained clinical remission without notable adverse effects.
Several case reports have described the successful use of bexarotene in patients with ALCL, as summarized in Table 1 [7-9]. Complete remission was achieved in all reported cases, including those treated after failure of chemotherapy or corticosteroids. Notably, our case represents the oldest reported patient (87 years) and is unique in that the lesion demonstrated resistance to high-dose radiotherapy. Moreover, this case is distinguished by the clear temporal correlation between reinitiation of bexarotene and prompt, sustained tumor regression.
These findings suggest that bexarotene may exert meaningful antitumor activity in pcALCL, even in previously irradiated or treatment-resistant lesions. The ability to induce durable remission with an oral agent that is generally well tolerated makes bexarotene particularly appealing for elderly or frail patients in whom aggressive systemic chemotherapy is not feasible.
Mechanistically, bexarotene is thought to promote tumor cell differentiation and apoptosis via RXR-mediated transcriptional regulation [10]. Although its effects have been well characterized in mycosis fungoides and Sézary syndrome [11], its application in pcALCL remains underrecognized. This case contributes to the limited but growing body of evidence supporting its use in this subtype.
Conclusions
In summary, our experience reinforces the potential of bexarotene as a viable treatment option for pcALCL, particularly in recurrent or refractory cases where conventional therapies are contraindicated or ineffective. Further accumulation of clinical data is needed to better define its optimal use and long-term outcomes in this context. Although our patient was elderly and refractory to radiotherapy, bexarotene may also be considered for patients with recurrent or multifocal pcALCL, or for those in whom conventional therapies are contraindicated because of comorbidities or cumulative radiation exposure. However, as this report describes a single case, larger prospective studies are warranted to confirm the efficacy and safety of bexarotene in a broader patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO-EORTC classification for cutaneous lymphomas Blood Willemze R Jaffe ES Burg G 3768378510520051569206310.1182/blood-2004-09-3502 · doi ↗ · pubmed ↗
- 2Prognostic factors in patients with primary cutaneous anaplastic large cell lymphoma: a multicentric, retrospective analysis of the Spanish Group of Cutaneous Lymphoma J Eur Acad Dermatol Venereol Fernández-de-Misa R Hernández-Machín B Combalía A 7627683420203159178610.1111/jdv.16006 · doi ↗ · pubmed ↗
- 3The optimal use of bexarotene in cutaneous T-cell lymphoma Br J Dermatol Gniadecki R Assaf C Bagot M 43344015720071755303910.1111/j.1365-2133.2007.07975.x · doi ↗ · pubmed ↗
- 4Updates in pathobiological aspects of anaplastic large cell lymphoma Front Oncol Wu R Lim MS 12415321320233781097410.3389/fonc.2023.1241532 PMC 10556522 · doi ↗ · pubmed ↗
- 5Recommendations for the optimal radiation dose in patients with primary cutaneous anaplastic large cell lymphoma: a report of the Dutch cutaneous lymphoma group Int J Radiat Oncol Biol Phys Melchers RC Willemze R Daniëls LA 127912859920172895877210.1016/j.ijrobp.2017.08.010 · doi ↗ · pubmed ↗
- 6Safety and efficacy of bexarotene for Japanese patients with cutaneous T-cell lymphoma: real-world experience from post-marketing surveillance J Dermatol Hamada T Morita A Suga H 2532624920223465806010.1111/1346-8138.16201 · doi ↗ · pubmed ↗
- 7Sustained response of primary cutaneous CD 30 positive anaplastic large cell lymphoma to bexarotene and photopheresis Leuk Lymphoma Sheehy O Catherwood M Pettengell R Morris TC 138913915020091954414110.1080/10428190903045385 · doi ↗ · pubmed ↗
- 8Response of CD 30+ large cell lymphoma of skin to bexarotene Leuk Lymphoma Keun YK Woodruff R Sangueza O 115311544320021214890110.1080/10428190290021425 · doi ↗ · pubmed ↗