Clinical outcomes of chlormethine gel in mycosis fungoides affecting “sensitive” areas: A retrospective case series
Gianluca Tavoletti, Gianluca Avallone, Pamela Vezzoli, Paolo Sena, Angelo V. Marzano, Emilio Berti, Silvia Alberti‐Violetti

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
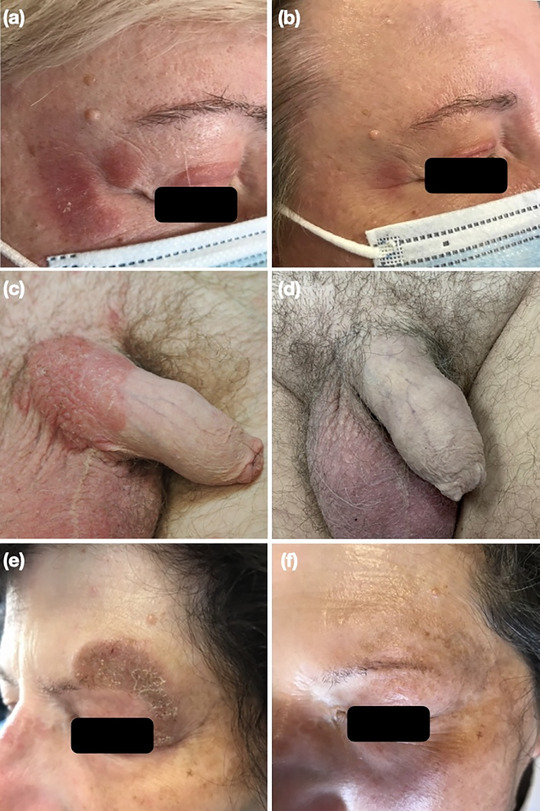 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Fungal Infections and Studies · Nail Diseases and Treatments
Dear Editors,
Chlormethine (CL) gel is the first skin‐directed therapy developed for the treatment of mycosis fungoides (MF).1 It is recommended as a first‐line treatment for adult patients with early‐stage MF (IA–IIA) and, in combination with systemic therapies, for those in advanced stages, according to international guidelines.2, 3, 4 Although clinical trials and real‐world evidence support its efficacy,5, 6 application of CL gel to anatomically “sensitive” areas (e.g., face, anogenital, and intertriginous regions) remains challenging due to the risk of local adverse events (AEs), particularly irritant contact dermatitis (ICD).7 While some anecdotal evidence suggests that CL gel may be used in such sites,8, 9 there is a need for real‐world data to elucidate its effectiveness and to detail management strategies for associated AEs.
We conducted a retrospective case series at two Italian tertiary referral centers from January 2020 to April 2024. The study was approved by the Ethics Committee Milano Area 2 (Protocol No: 0007202). Eligible patients had a histologically confirmed diagnosis of MF with at least one “sensitive” area involved and were treated with CL gel. Assessments were performed at baseline and every 3 months, in accordance with standard clinical care and institutional protocols. The response was evaluated using a modified Composite Assessment of Index Lesion Severity (mCAILS), which excluded hyperpigmentation.7, 8 The objective response rate (ORR), defined as the proportion of patients who achieved either a complete (mCAILS = 0) or partial response (≥ 50% reduction in mCAILS) at the three‐month evaluation,6 was calculated. AEs were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0.10
We included eight patients (5 males and 3 females) at different stages of MF (75% in early stage) (Table 1). The median age of patients was 56.5 years (Q1 = 50; Q3 = 58.5), and the median age at diagnosis was 43.5 years (Q1 = 40; Q3 = 49). Clinical variants were classical MF (n = 5), folliculotropic MF (n = 2), and poikilodermatous MF (n = 1). “Sensitive” areas involved the eyelid (n = 3), groin, cheek, perineum, pubic region, penis, and scrotum. Four patients (50%) used concomitant topical corticosteroids (TCS) to reduce local irritation, and three (38%) were receiving systemic therapy. Two patients (25%) applied CL gel daily, and six patients (75%) applied it on alternate days. The median treatment duration was 3 months (Q1 = 2; Q3 = 3.5). At three months, six patients (75%) achieved the ORR, while two had persistent disease, yet decreased in severity. Among patients undergoing systemic therapy, CL gel was introduced on targeted recalcitrant or new lesions, further supporting overall disease control. At a median follow‐up of 22 months (Q1 = 14; Q3 = 42), six patients achieved and maintained a complete response (mCAILS = 0), while two (25%) displayed minimal residual disease (Figure 1). Adverse events occurred in six patients (75%) and included mild ICD in three patients (38%), moderate ICD in two (25%), and severe ICD in one (13%). All but one patient continued CL gel after a brief interruption or a reduced application frequency. Adjunctive TCS was used to manage inflammation, with clinicians remaining cautious due to the heightened risk of steroid‐induced atrophy in sensitive areas. Transient hyperpigmentation was observed in the treated areas of six patients (75%).
Although clinical trials suggest that sensitive areas are at increased risk of AEs related to CL gel use,7, 8 this retrospective case series demonstrates that CL gel can be both safe and effective for MF lesions in sensitive skin regions. The concomitant use of TCS appears to enhance tolerability, aligning with prior observational evidence.6
Study limitations include the retrospective design, the relatively small sample size, and the exclusive inclusion of Caucasian patients. Future prospective studies should investigate optimal application schedules, evaluate supportive measures to prevent or manage ICD, and further clarify the role of CL gel in combination with systemic agents.
CONFLICT OF INTEREST STATEMENT
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guenova E , Ortiz‐Romero PL , Poligone B , Querfeld C . Mechanism of action of chlormethine gel in mycosis fungoides. J Eur Acad Dermatol Venereol. 2023;37(9):1739‐1748.37262305 10.1111/jdv.19237 · doi ↗ · pubmed ↗
- 2Latzka J , Assaf C , Bagot M , et al. EORTC consensus recommendations for the treatment of mycosis fungoides/Sézary syndrome ‐ Update 2023. Eur J Cancer. 2023;195:113343.37890355 10.1016/j.ejca.2023.113343 · doi ↗ · pubmed ↗
- 3National Comprehensive Cancer Network . NCCN Clinical Practice Guidelines ® (NCCN Guidelines). Primary cutaneous lymphomas. Version 2.2020. Available from: https://www.nccn.org/professionals/physician_gls/pdf/primary_cutaneous.pdf [Last accessed December 20, 2022].
- 4Quaglino P , Prince HM , Cowan R , et al. Treatment of early‐stage mycosis fungoides: results from the PR Ospective Cutaneous Lymphoma International Prognostic Index (PROCLIPI) study [published correction appears in Br J Dermatol. 2021 Sep;185(3):685]. Br J Dermatol. 2021;184(4):722‐730.32479678 10.1111/bjd.19252 PMC 7704558 · doi ↗ · pubmed ↗
- 5Geskin LJ , Bagot M , Hodak E , Kim EJ . Chlormethine Gel for the Treatment of Skin Lesions in All Stages of Mycosis Fungoides Cutaneous T‐Cell Lymphoma: A Narrative Review and International Experience. Dermatol Ther (Heidelb). 2021;11(4):1085‐1106.34021485 10.1007/s 13555-021-00539-3PMC 8322195 · doi ↗ · pubmed ↗
- 6Alberti‐Violetti S , Ardigò M , Massone C , et al. Effectiveness and tolerability of chlormethine gel for the management of mycosis fungoides: a multicenter real‐life evaluation. Front Oncol. 2024;13:1298296.38239642 10.3389/fonc.2023.1298296 PMC 10794371 · doi ↗ · pubmed ↗
- 7Ledaga [summary of product characteristics]. Dublin, Ireland: Helsinn Birex Pharmaceuticals Ltd.; 2017. Available from: https://www.ema.europa.eu/en/documents/product‐information/ledaga‐epar‐product‐information_en.pdf [Last accessed July 7, 2024].
- 8Lessin SR , Duvic M , Guitart J , et al. Topical chemotherapy in cutaneous T‐cell lymphoma: positive results of a randomized, controlled, multicenter trial testing the efficacy and safety of a novel mechlorethamine, 0.02%, gel in mycosis fungoides. JAMA Dermatol. 2013;149(1):25‐32.23069814 10.1001/2013.jamadermatol.541PMC 3662469 · doi ↗ · pubmed ↗