Stomach cancer elective surgery morbidity and mortality at 90-Day (Hold Study): a prospective, international collaborative cohort study
Claudia Neves-Marques, Mohamed Abulazayem, Geoffrey Yuet Mun Wong, Ricardo David Maldonado, Yirupaiahgari Viswanath, Alex Boddy, Claire Donohoe, Juan Pablo Scarano, Alessandro Martinino, Amaar Aamery, Nuriddin Abdulkhakimov, Essam Eldien Abuobaida, Ulaş Aday, Khayry Al-Shami

TL;DR
This study reports global 90-day outcomes after elective gastric cancer surgery and identifies risk factors for complications and mortality.
Contribution
The study provides the most comprehensive international prospective data on gastric cancer surgery outcomes and associated risk factors.
Findings
90-day morbidity rate was 38.2% and mortality rate was 2.9%.
Factors like higher comorbidity index and weight loss were linked to worse outcomes.
Abstract
Data on multinational 90-day mortality and morbidity rates after surgery for gastric cancer is limited in the literature. This study aimed to understand the 90-day mortality and morbidity outcomes among patients undergoing elective gastric cancer surgery, as in the GASTRODATA Registry, and to identify associated risk factors. We conducted an international prospective study on patients aged ≥ 18 years undergoing elective surgery for gastric cancer with curative intent from January 4 to September 30, 2022. Known metastatic disease, concurrent secondary cancers, gastrointestinal stromal tumour (GIST) and Siewert type I/II oesophagogastric junction malignancies were excluded. Univariate and multivariate logistic regression were used to identify variables associated with the 90-day outcome. 380 collaborators from 47 countries submitted data on 1538 patients. Median age was 65 years (IQR:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
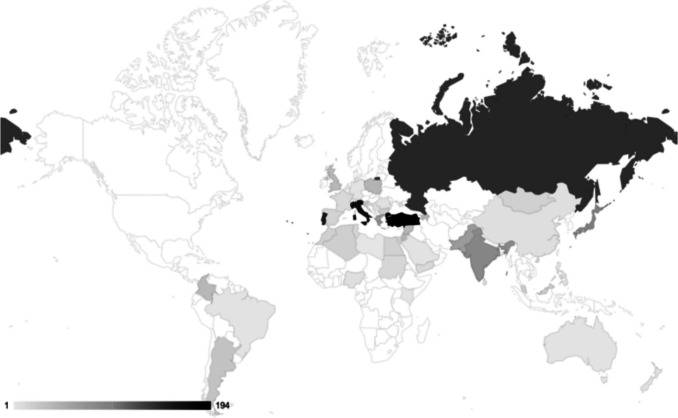 Figure 1
Figure 1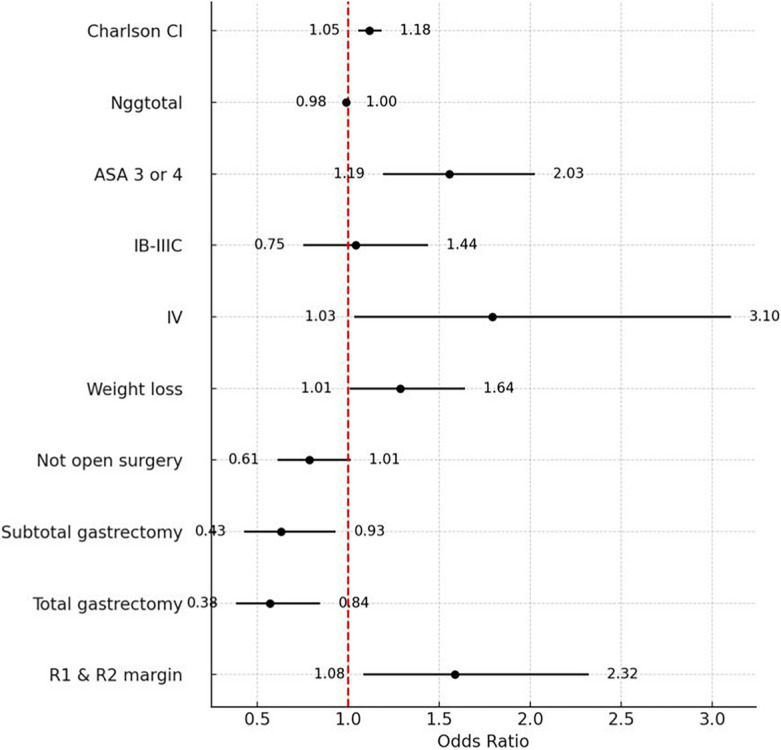 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Enhanced Recovery After Surgery · Helicobacter pylori-related gastroenterology studies
Introduction
Gastric cancer is the fifth most common malignancy and the fifth leading cause of cancer mortality worldwide, as reported by GLOBOCAN (Global Cancer Observatory) [1]. Surgical resection with regional lymphadenectomy remains the gold standard of treatment [2–4]. The primary aim of treatment is complete resection with microscopically negative margins. While subtotal gastrectomy is favoured to reduce postoperative morbidity, total gastrectomy (TG) is often necessary [5, 6] to achieve adequate treatment.
In the management of gastric cancer, the shift towards evidence-based and precision-oriented care has led to the adoption of standardised treatment protocols [4, 7] and improved surgical performance. This includes the integration of multimodal strategies, minimally invasive surgical techniques, and the development of comprehensive complication registries and follow-up databases [2, 8]. The centralisation of surgical procedures and the adoption of multimodal treatment strategies have improved outcomes of gastric cancer surgery [7, 9] by targeting both local and systemic disease, enhancing surgical effectiveness and supporting patient recovery. Delivered within a multidisciplinary framework, these approaches optimise both oncological results and perioperative recovery. Nevertheless, morbidity and mortality rates vary significantly among countries [10, 11]. This can be attributed to several factors, including screening programmes, disease incidence, management protocols, stage of cancer at presentation, surgical techniques, and follow-up [12].
The mortality rates in the East are consistently lower [13, 14], with 30-day mortality rates below 1% [15, 16]. Conversely, western countries report a wider morbidity range [17, 18] from 6.3% to 43% [13, 19, 20] and higher mortality rates, spanning 2 to 12.8% [21–23], mostly reported until 30 days postoperatively.
Complications following surgical intervention in gastric cancer patients adversely influence the oncological prognosis, manifesting in reduced survival rates [24] and earlier recurrence. While several studies have reported on 60- and 90-day postoperative morbidity and mortality in gastric cancer surgery [9, 14, 25–29], many have been limited by a focus on a single surgical technique, a single-country dataset, or relatively small multicentre cohorts [9, 14, 25, 26]. Our study contributes to this body of work by providing the most comprehensive 90-day prospective data to date, encompassing large-scale, international, prospective data across various surgical approaches.
The main aims of this study were to understand the global 90-day morbidity and mortality rates of curative gastric cancer surgery and to understand factors associated with morbidity.
Methods
Study Design
We conducted a global, multicentre, prospective observational cohort study. The study was registered as a clinical audit at James Cook University Hospital, Middlesbrough, UK (Registration Number CATS ID 8504). The primary aim was to assess the 90-day mortality and morbidity rates of patients who underwent elective gastric cancer surgery between 01/04/2022 and 30/09/2022 at participating centres. The secondary aim was to identify the factors influencing these rates.
Data collection
We collected demographic data, pre- operative data (cTNM staging, neoadjuvant therapy), surgical data (gastric resection and lymphadenectomy, surgical approach, reconstruction, jejunostomy, surgery duration and definitive histopathology report), and 90-day outcomes. The Gastrectomy Complications Consensus Group (GCCG) of GASTRODATA [27] was used to identify postoperative complications and morbidity. General postoperative complications included systemic events such as infections, respiratory or renal failure, while surgical postoperative complications referred to events directly related to the operative site, such as anastomotic leaks, postoperative bleeding, or bowel perforation. We used the Clavien-Dindo (CD) classification [30, 31] to record the severity of complications, including mortality. We defined a clinically relevant morbidity as CD ≥ II [32]. This study focused on the number of patients who developed complications rather than the number of complications. The highest CD score was considered when a patient experienced more than one complication. The eighth edition of the TNM (TNM-8) was used for tumour staging [33].
The study was promoted to the members of The Upper Gastrointestinal Surgical Society (TUGSS) through emails and widely disseminated on social media. Researchers collected anonymised patient data and submitted it in a password-protected Microsoft Excel sheet and the password was shared separately to preserve data confidentiality. A 'Data Dictionary' file was shared with all researchers, Appendix 1*.* To mitigate selection bias, collaborators were asked to record all consecutive eligible patients during the study period. After submission, we examined the data for incomplete or missing information and contacted collaborators for clarification as needed.
Participants
All adults (≥ 18 years) diagnosed with primary gastric cancer, including Siewert type III, who were candidates for elective surgery with curative intent. Exclusion criteria were patients with gastrointestinal stromal tumour (GIST), preoperative known metastatic disease, positive peritoneal cytology at staging laparoscopy or definitive surgery, concurrent secondary cancers, those with Siewert type I or II oesophagogastric junction malignancies, and patients requiring emergency surgical interventions or other surgeries in addition to the primary gastric malignancy treatment.
Statistical analysis
Univariate and multivariate logistic regression were used to identify variables associated with minor (Clavien-Dindo 0 and I) and clinically significant (Clavien-Dindo II-V) postoperative outcomes. Multivariable analysis was performed for factors with a p-value of ≤ 0.20 in the univariable analysis. All statistical testing was two‐sided, with significance defined as a p-value < 0.05. Lasso analysis for logistic regression was performed to validate the findings. The dataset was split into a testing sample (75%) and a validation sample (25%) with random allocation. Lasso analysis for logistic regression was performed to validate and further explore the relevance of the variables selected by the multivariate logistic regression model. Data management and statistical analyses were performed using Stata® SE for Windows® version 15.1 (StataCorp, College Station, TX, USA).
Ethical considerations
Collaborators were responsible for obtaining local permission and patient consent and documenting that conversation in the patient record.
Results
Pre-operative demographic, clinical, and imaging data
The study considered data from 1,670 patients across 138 hospitals in 47 countries, submitted by 380 collaborators (Fig. 1). We excluded 132 (7.9%) patients as they did not meet our inclusion criteria, resulting in a final analysis of 1,538 patients. Table 1 shows the demographic characteristics of our cohort.Fig. 1. Heatmap Patients/Country: Number of patients (n = 1538) included in the HOLD Study by country (47 countries)Table 1. Basic demographic data (n = 1538)PATIENT CHARACTERISTICS GASTRIC RESECTIONOverall,N = 1538Subtotal Gastrectomy,N = 761Total Gastrectomy,N = 627Extended Total Gastrectomy,N = 74Proximal Gastrectomy, N = 48Oesophago-Gastrectomy,N = 28Age64,2 ± 13,465,9 ±12,962,6 ± 13,560,9 ± 15,466,2 ± 11,358,5 ± 13,5Gender | Male966 (62,8%)441 (28,7%)418 (27,2%)51 (3,3%)35 (2,3%)21 (1,4%)Preoperative BMI24,7 ± 4,724,4 ± 4,624,9 ± 4,925,7 ± 4,426,5 ± 5,823,9 ± 3,4Preoperative Weight Loss > 10%624 (40,6%)295 (19,2%)267 (17,4%)32 (2,1%)14 (0,9%)16 (1,0%)ASA1210 (13,7%)100 (6,5%)94(6,1%)7 (0,5%)3 (0,2%)6 (0,4%)2742 (48,2%)372(24,2%)298 (19,4%)33 (2,1%)29 (1,9%)10 (0,7%)3551 (35,8%)275 (17,9%)216 (14,0%)33 (2,1%)15 (1,0%)12 (0,8%)435 (2,3%)14 (0,9%)19 (1,2%)1 (0,1%)1 (0,1%)-Charlson Comorbidity index (CCI)4,8 ± 2,34,9 ± 1,64,7 ± 2,15,9 ± 2,44,9 ± 3,05,1 ±2,9ECOG(a)0686 (44,6%)358 (23,3%)266 (17,3%)35 (2,3%)15 (1,0%)12 (0,8%)1548 (35,7%)258 (16,8%)241 (15,7%)20 (1,3%)18 (1,2%)11 (0,7%)2206 (13,4%)100 (6,5%)83 (5,4%)10 (0,7%)10 (0,7%)3 (0,2%)384 (5,5%)41 (2,7%)30 (2,0%)6 (0,4%)5 (0,3%)2 (0,1%)413 (0,8%)4 (0,3%)6 (0,4%)3 (0,2%)--BMI Body Mass Index; ASA American Society of Anaesthesiologists; ECOG Eastern Cooperative Oncology Group Performance Status;(a) In ECOG, information was missing from 1 patient, a Total gastrectomy
The median age of patients was 65 years (interquartile Range -IQR: 19–94), with 50% of patients aged between 56 and 74 years. Overall, 62.8% were male. In our study, each additional year of age was correlated with a 1.3% increase in the odds (p = 0.0013) of experiencing clinically relevant 90-day morbidity (CD II-V) and mortality. The median body mass index (BMI) was 24.5 kg/m^2^, and 40.6% of the patients experienced severe weight loss (> 10% of body weight) in the 6 months preceding surgery.
Caucasians accounted for 58.5% of all patients, followed by Asians (26.0%). Nearly half of the cohort (48.2%) had an American Society of Anaesthesiologists (ASA) score of II, and 44.6% had an Eastern Cooperative Oncology Group (ECOG) Performance Status [34] of 0. Approximately 52.7% of the patients had a Charlson Comorbidity Index (CCI) score of 5 or higher [35, 36].
More than half (61.5%) were diagnosed as cT2-T3 stages with nodal (cN +) involvement (51.7%), and 4.4% were suspected to have cT4 disease. Pre-operatively, 3.4% of patients had incomplete staging [2–4, 33] and 11.2% had unknown histology [2–4]. Despite the high prevalence of advanced gastric cancer at diagnosis, fewer than half of patients received neoadjuvant therapy. Among those staged as cT3–cT4, 57.1% underwent neoadjuvant chemotherapy, accounting for 76.0% of all patients treated in the neoadjuvant setting. In total, 680 patients received neoadjuvant chemotherapy, predominantly those with cT3–cT4 disease (n = 504) and/or node-positive disease (cN + , n = 481). Treatment completion, however, was suboptimal, with 13.7% (n = 93) failing to complete the planned regimen. Notably, completion rates were markedly lower in patients aged > 70 years (28.3%) when compared with younger patients (54.4%). Patients in the "No neoadjuvant chemotherapy but should" subgroup showed higher Charlson Comorbidity Index scores, indicating a greater burden of co-existing conditions and suggesting increased complexity and risk in their surgical care. Table 2 provides details of staging and neoadjuvant therapy.Table 2. Pre-operative Staging and Oncological Data (n = 1538)PATIENT CHARACTERISTICS GASTRIC RESECTIONOverall,N = 1538Subtotal Gastrectomy,N = 761Total Gastrectomy,N = 627Extended Total Gastrectomy,N = 74Proximal Gastrectomy, N = 48Oesophago-Gastrectomy,N = 28cT(a)T0**10 (0,7%)3 (0,2%)5 (0,3%)1 (0,1%)1 (0,1%)-T1206 (13,4%)134 (8,7%)48 (3,1%)2 (0,1%)18 (1,2%)4 (0,3%)T2334 (21,7%)181 (11,8%)141 (9,2%)4 (0,3%)5 (0,3%)3 (0,2%)T3612 (39,8%)270 (17,6%)281 (18,3%)40 (2,6%)10 (0,7%)11 (0,7%)T4271 (17,6%)122 (7,9%)117 (7,6%)21 (1,4%)5 (0,3%)6 (0,4%)Tis4 (0,3%)3 (0,2%)1 (0,1%)---Tx101 (6,6%)48 (3,1%)34 (2,2%)6 (0,4%)9 (0,6%)4 (0,3%)cN(a)N0586 (38,1%)**337 (21,9%)204 (13,3%)16 (1,0%)22 (1,4%)7 (0,5%)N + **795 (51,7%)346 (22,5%)364 (23,7%)53 (3,4%)16 (1,0%)16 (1,0%)Nx157 (10,2%)78 (5,1%)59 (3,8%)5 (0,3%)10 (0,7%)5 (0,3%)cM(a)M01366 (88,8%)698 (45,4%)560 (36,4%)51 (3,3%)36 (2,3%)21 (1,4%)M168 (4,4%)24 (1,6%)25 (1,6%)17 (1,1%)1 (0,1%)1 (0,1%)Mx104 (6,8%)39 (2,5%)42 (2,7%)6 (0,4%)11 (0,7%)6 (0,4%)Neoadjuvant ChemotherapyGiven, completed587 (38,2%)223 (14,5%)293 (19,1%)44 (2,9%)13 (0,8%)14 (0,9%)Given, not completed93 (6,1%)28 (1,8%)44 (2,9%)14 (0,9%)5 (0,3%)2 (0,1%)Not given856 (55,7%)509 (33,1%)289 (18,8%)16 (1,0%)30 (2,0%)12 (0,8%)Missing data2 (0,1%)**1 (0,1%)1 (0,1%)---(a) James D. Brierley (Editor) MKG (Editor), CW (Editor). TNM Classification of Malignant Tumours, 8th Edition. Wiley-Blackwell; 2017
Gastric adenocarcinoma (87.7%) was the most common type, followed by adenosquamous carcinoma (2.9%) and undifferentiated carcinoma (2.1%) [37]. Other neoplasms, such as squamous cell carcinoma and lymphoma, accounted for 1.6% and 4.4% of the cases, respectively.
Surgical approach and postoperative histopathology
Subtotal (49.5%, n = 761) and total (40.8%, n = 627) gastrectomies were the most common types of surgery, as shown in Table 3. These resections presented a 40% lower risk (p < 0.001) of clinically relevant postoperative morbidity and mortality when compared to all other resections. Total gastrectomy had the highest conversion to open rate (13.2%). Only a minority of conversions to open (12.3%) were due to intraoperative adverse events.Table 3. Surgery details regarding patients undergoing elective gastric surgery for malignancy (n = 1538)PATIENT CHARACTERISTICS GASTRIC RESECTIONOverall,N = 1538Subtotal Gastrectomy,N = 761Total Gastrectomy,N = 627Extended Total Gastrectomy,N = 74Proximal Gastrectomy, N = 48Oesophago-Gastrectomy,N = 28Surgical ApproachOpen**874 (56,8%)408 (26,5%)378 (24,6%)42 (2,7%)29 (1,9%)17 (1,1%)Laparoscopic452 (29,4%)266 (17,3%)145 (9,4%)20 (1,3%)14 (0,9%)7 (0,5%)Robotic69 (4,5%)39 (2,5%)21 (1,4%)2 (0,1%)5 (0,3%)2 (0,1%)Laparoscopic/Robotic Converted to Open143 (9,3%)48 (3,1%)83 (5,4%)10 (0,7%)-2 (0,1%)ReconstructionRoux en Y1113 (72,4%)471 (30,6%)564 (36,7%)57 (3,7%)8 (0,5%)13 (0,8%)Bilroth I27 (1,8%)21 (1,4%)2 (0,1%)1 (0,1%)3 (0,2%)-Bilroth II285 (18,5%)248 (16,1%)21 (1,4%)8 (0,5%)2 (0,1%)6 (0,4%)Jejunal Interposition34 (2,2%)6 (0,4%)16 (1,0%)6 (0,4%)4 (0,3%)2 (0,1%)Colonic Interposition9 (0,6%)1 (0,1%)1 (0,1%)1 (0,1%)-6 (0,4%)Gastric Reconstruction30 (2,0%)5 (0,3%)2 (0,1%)1 (0,1%)21 (1,4%)1 (0,1%)Undetailed Reconstruction40 (2,6%)9 (0,6%)21 (1,4%)-10 (0,7%)-Jejunostomy performed169 (11,0%)55 (3,6%)84 (5,5%)14 (0,9%)4 (0,3%)12 (0,8%)Lympha-denectomyD031 (2,0%)18 (1,2%)7 (0,5%)2 (0,1%)4 (0,3%)-D1258 (16,8%)**131 (8,5%)95 (6,2%)14 (0,9%)8 (0,5%)10 (0,7%)D1 + **216 (14,0%)125 (8,1%)68 (4,4%)8 (0,5%)14 (0,9%)1 (0,1%)D2970 (63,1%)**470 (30,6%)420 (27,3%)43 (2,8%)21 (1,4%)16 (1,0%)D2 + **62 (4,0%)16 (1,0%)37 (2,4%)7 (0,5%)1 (0,1%)1 (0,1%)Missing data1 (0,1%)**1 (0,1%)----Lymph nodes harvested in D2(average ± standard deviation)**28,6 **±14,529,5 ±14,928,3 ±14,427,9 ±11,319,2 ±8,125,7 ±10,7
Open surgery (56.8%) was the most common technique, followed by laparoscopic surgery (29.4%) and robotic surgery (4.5%). Laparoscopic surgery was more common in early stages (49.2% in Ia), while open surgery was the preferred technique in advanced stages (80.9% in IIIc). Roux-en-Y reconstruction was the primary approach for gastrointestinal tract reconstruction (72.4%), and a complete macroscopic resection margin was achieved in 89.1% (n = 1371) of patients. The median duration of surgery was 220.0 min (IQR: 161.3–270.0).
D2 lymphadenectomy was reported in 63.1% (n = 970) of patients, with a median of 22.5 lymph nodes (IQR: 14.0–33.5) harvested. Adequate lymph node retrieval (> 15 lymph nodes) for pathological staging was achieved in 79.1% of cases, with 5.2% missing data. Jejunostomy was performed in 11.0% of the cohort (n = 169), most commonly in oesophago-gastric resections.
The final pathology report (pTNM) was completed in 94.7% (n = 1456) of patients, with 74.2% (n = 1141) staged as locally advanced gastric cancer (≥ Ib) (Table 4). Node-negative status (pN0) was observed in 38.6% of the patients. Chemotherapy details were inconsistently reported across centres, limiting treatment-specific analysis. The majority of patients received standard perioperative regimens (e.g., FLOT or ECF). Pathological complete remission (pT0) occurred in 4.3% of patients receiving neoadjuvant chemotherapy (n=29). In definitive pathology, early gastric cancer was identified in 15.8% (n = 238) of cases, an increase from 13.4% identified at clinical staging.Table 4. Data regarding definitive histopathology report after surgery (n = 1538)PATIENT CHARACTERISTICSGASTRIC RESECTIONOverall,N = 1538Subtotal Gastrectomy,N = 761Total Gastrectomy,N = 627Extended Total Gastrectomy,N = 74Proximal Gastrectomy, N = 48Oesophago-Gastrectomy,N = 28Tumour Histology (WHO) (a)Adenocarcinoma1349 (87,7%)681 (44,3%)554 (36,0%)55 (3,6%)43 (2,8%)16 (1,0%)Adenosquamous45 (2,9%)18 (1,2%)15 (1,0%)6 (0,4%)1 (0,1%)5 (0,3%)Undifferentiated33 (2,1%)16 (1,0%)12 (0,8%)2 (0,1%)1 (0,1%)2 (0,1%)Squamous Cell Carcinoma24 (1,6%)10 (0,7%)9 (0,6%)1 (0,1%)1 (0,1%)3 (0,2%)Carcinoma with lymphoid stroma13 (0,8%)3 (0,2%)6 (0,4%)2 (0,1%)1 (0,1%)1 (0,1%)Hepatoid Carcinoma6 (0,4%)1 (0,1%)1 (0,1%)4 (0,3%)--Other68 (4,4%)32 (2,1%)30 (2,0%)4 (0,3%)1 (0,1%)1 (0,1%)pTT037 (2,4%)19 (1,2%)16 (1,0%)1 (0,1%)-1 (0,1%)Tis2 (0,1%)-1 (0,1%)1 (0,1%)--T1**324 (21,1%)201 (13,1%)86 (5,6%)6 (0,4%)25 (1,6%)6 (0,4%)T2269 (17,5%)142 (9,2%)102 (6,6%)11 (0,7%)7 (0,5%)7 (0,5%)T3527 (34,3%)225 (14,6%)251(16,3%)30 (2,0%)11 (0,7%)10 (0,7%)T4375 (24,4%)172 (11,2%)169 (11,0%)25 (1,6%)5 (0,3%)4 (0,3%)Tx4 (0,3%)2 (0,1%)2 (0,1%)---pNN0594 (38,6%)337 (21,9%)207 (13,5%)17 (1,1%)25 (1,6%)8 (0,5%)N1269 (17,5%)139 (9,0%)102 (6,6%)16 (1,0%)11 (0,7%)1 (0,1%)N2288 (18,7%)121 (7,9%)123 (8,0%)24 (1,6%)8 (0,5%)12 (0,8%)N3281 (24,8%)161 (10,5%)192 (12,5%)17 (1,1%)4 (0,3%)7 (0,4%)Nx6 (0,4%)3 (0,2%)3 (0,2%)---Resection MarginR01371 (89,1%)707 (46,0%)553 (36,0%)50 (3,3%)41 (2,7%)20 (1,3%)R1130 (8,5%)47 (31%)57 (3,7%)16 (1,0%)7 (0,5%)3 (0,2%)R237 (2,4%)7 (0,5%)17 (1,1%)8 (0,5%)-5 (0,3%)Lymph nodes > 151217 (79,1%)**35 (2,3%)599 (38,9%)506 (32,9%)57 (3,7%)20 (1,3%)Total Number(pN total)26,7 ± 15,026,5 ±15,627,6 ± 14,826,2 ±13,520,1 ±11,924,7 ±10,9Positive (pN +)4,7 ± 7,13,8 ±6,36,0 ±8,24,7 ±5,22,2 ±3,65,8 ±7,2(a) Kushima R LGRM. WHO Classification of Tumours: Digestive Systemic Tumours. 5th ed. WHO Classification of Tumours Editorial Board, editor. Vol. Gastric Dysplasia. International Agency for Research on Cancer 2019
Less than half of the clinically suspected metastatic disease was confirmed as pM1 (i.e. peritoneal invasion or positive cytology), with 54.8% of pM1 also categorised as either R1 or R2 resection. Most patients (89.1%, n = 1371) achieved a microscopic R0 resection. R2 resections, which are rarely reported in gastric cancer surgery [38], were observed in 2.4% of cases. R1 resection was most frequent in patients undergoing extended total gastrectomy (21.6%) and in those with stage IIIa–IIIc disease (58.3%). Notably, approximately half of patients with R1 resections (54.5%) had received pre-operative chemotherapy.
90-day Morbidity and Mortality
In this cohort, the 90-day morbidity rate was 38.2% (n = 587), and the mortality rate was 2.9% (n = 45). Following Clavien Dindo (CD) classification, 12.0% (n = 184) had CD Grade I, 12.2% (n = 188) had CD Grade II, 10.5% (n = 162) had CD Grade III, and 3.4% (n = 53) had CD Grade IV (Table 5).Table 5. Postoperative data of patients undergoing curative elective gastric surgery for malignancy (n = 1538)90-DAY MORBIDITY and MORTALITYGASTRIC RESECTIONOverall,N = 1538Subtotal Gastrectomy,N = 761Total Gastrectomy,N = 627Extended Total Gastrectomy,N = 74Proximal Gastrectomy, N = 48Oesophago-Gastrectomy,N = 28Clavien Dindo ClassI**184 (12,0%)93 (6,0%)76 (4,9%)3 (0,2%)7 (0,5%)5 (0,3%)II188 (12,2%)90 (5,9%)74 (4,8%)13 (0,8%)10 (0,7%)1 (0,1%)IIIa85 (5,5%)38 (2,5%)33 (2,1%)8 (0,5%)4 (0,3%)2 (0,1%)IIIb77 (5,0%)40 (2,6%)27 (1,8%)7 (0,5%)2 (0,1%)1 (0,1%)IVa42 (2,7%)16 (1,0%)17 (1,1%)5 (0,3%)1 (0,1%)3 (0,2%)IVb11 (0,7%)**3 (0,2%)6 (0,4%)1 (0,1%)1 (0,1%)-V (Mortality)**45 (2,9%)22 (1,4%)16 (1,0%)5 (0,3%)2 (0,1%)-Total Morbidity and Mortality at 90-day632 (41,1%)**302 (19,6%)249 (16,2%)42 (2,7%)27 (1,8%)12 (0,8%)Postoperative Complications Incidence at 90 days (a)Non-Surgical Infections (c)**73 (4,7%)**31(2,0%)28 (1,8%)2 (0,1%)8 (0,5%)4 (0,3%)Anastomotic leak (b)**70 (4,6%)**19 (1,2%)37 (2,4%)9 (0,6%)3 (0,2%)2 (0,1%)Abnormal fluid from drainage / abdominal collections WITHOUT Leak (b)**52 (3,4%)**30 (2,0%)20 (1,3%)1 (0,1%)-1 (0,1%)Postoperative bleeding requiring invasive treatment (b)**40 (2,6%)**16 (1,0%)17 (1,1%)5 (0,3%)1 (0,1%)1 (0,1%)Pleural effusion requiring drainage (c)**36 (2,3%)**11 (0,7%)21 (1,4%)2 (0,1%)2 (0,1%)-Postoperative bowel obstruction (b)**34 (2,2%)**14 (0,9%)15 (1,0%)3 (0,2%)1 (0,1%)1 (0,1%)Duodenal leak (b)**29 (1,9%)**20 (1,3%)4 (0,3%)4 (0,3%)-1 (0,1%)Respiratory failure requiring reintubation (c)**21 (1,4%)**10 (0,7%)8 (0,5%)2 (0,1%)-1 (0,1%)Need for prolonged intubation (> 24 h after surgery) OR Tracheostomy (c)**21 (1,4%)**4 (0,3%)10 (0,7%)5 (0,3%)-2 (0,1%)Pulmonary embolism (c)**20 (1,3%)**6 (0,4%)10 (0,7%)3 (0,2%)1 (0,1%)-Delayed gastric emptying (> 10th postoperative day) (b)**18 (1,2%)**14 (0,9%)3 (0,2%)-1 (0,1%)-Acute renal failure requiring CVVH/dialysis (c)**15 (1,0%)**8 (0,5%)5 (0,3%)2 (0,1%)--Postoperative pancreatic fistula (b)**14 (0,9%)**7 (0,5%)2 (0,1%)4 (0,3%)1 (0,1%)Myocardial infarction (c)**14 (0,9%)**6 (0,4%)5 (0,3%)1 (0,1%)2 (0,1%)-Postoperative bowel perforation or necrosis (b)**9 (0,6%)**3 (0,2%)3 (0,2%)3 (0,2%)--Postoperative pancreatitis (b)**7 (0,5%)**2 (0,1%)5 (0,3%)---Others (d)**296 (19,2%)**146 (9,5%)118 (7,7%)17 (1,1%)12 (0,8)3 (0,2%)Length of stay (days)**11,0 ±8,710,5 ±8,611,0 ±8,715,2 ±11,311,6 ±5,612,6 ±6,5Need for Reoperation124 (8,1%)68 (4,4%)42 (2,7%)10 (0,7%)1 (0,1%)3 (0,2%)Readmission163 (10,6%)**81 (5,3%)59 (3,8%)14 (0,9%)5 (0,3%)4 (0,3%)(a) Following GASTRODATA Registry—Baiocchi GL, Giacopuzzi S, Marrelli D, Reim D, Piessen G, Matos da Costa P, et al. International consensus on a complications list after gastrectomy for cancer. Gastric Cancer. 2019 Jan 22;22(1):172–89(b) Surgical Post Operative complications(c) General Post Operative complications (non Surgical)(d) Other included n = 9 Acute cardiac failure OR cardiac dysrhythmia, n = 8 Cardiopulmonary resuscitation, n = 3 acute liver dysfunction, n = 3 stroke with permanent deficit, n = 2 Pneumothorax requiring treatment, n = 1 surgical site infections, n = 179 non-detailed general complications, n = 57 non-detailed minor surgical complications, n = 34 non-detailed major complications requiring intervention
Complications were further categorised according to the GASTRODATA classification [27], with general complications representing 42.4% and surgical complications representing 35.9% of all adverse events. Both types co-occurred in 21.5% of patients, with missing data in 0.2% of cases. Mortality was up to threefold higher among patients experiencing both general and surgical complications. Non-surgical infections (4.7%; n = 73), anastomotic leak (4.6%; n = 70), abnormal fluid drainage (3.4%; n = 52), and postoperative bleeding requiring invasive treatment (2.6%; n = 40) were the most frequent causes of morbidity. A detailed description of 90-day morbidity and mortality is provided in Table 5.
Univariate analysis for 90-day morbidity and mortality
On univariate analysis, several pre-operative factors were significantly associated with increased 90-day clinically relevant morbidity and mortality (Clavien–Dindo grade II–V), including older age, higher Charlson Comorbidity Index (CCI), ASA score of 3 or 4, ECOG performance status of 3–4, and severe pre-operative weight loss. ECOG 3–4 was associated with clinically relevant morbidity and mortality outcomes, presenting twice the risk of CD II-V outcome. Surgical variables such as longer operative duration, positive resection margins (R1/R2), and pathologically confirmed metastatic disease (pM1) were also associated with worse outcomes. BMI, gender, and surgical approach (open vs minimally invasive) were not associated with 90-day clinically relevant morbidity and mortality.
Multivariate analysis for 90-day morbidity and mortality
On multivariate analysis, 90-day clinically relevant morbidity and mortality was significantly associated with pre-operative higher CCI [(p < 0.001), (OR = 1.12), (95% CI = 1.05–1.18)], ASA score 3 or 4 [(p = 0.001), (OR = 1.55), (95% CI = 1.19–2.02)], severe pre-operative weight loss [(p = 0.042), (OR = 1.29), (95% CI = 1.0–1.6)] and surgical determinants such as pathological staging with confirmed metastatic disease [(p = 0.038), (OR = 1.79), (95% CI = 1.03–3.10)] and positive (R1 or R2) margin [(p = 0.018), (OR = 1.59), (95% CI = 1.08–2.32)]. Age, ECOG performance status, procedure duration, total number of harvested lymph nodes and surgical approach (open vs minimally invasive) were not associated with 90-day clinically relevant morbidity and mortality on multivariate analysis. Details of the analysis are presented in Table 6.Table 6. Univariate and multivariate logistic regression analysis for predicting clinically relevant morbidity and mortality (Clavien Dindo II-V) (n = 1538)PREDICTORs OF 90-DAYCLINICALLY RELEVANT MORBIDITY AND MORTALITYUnivariate analysisMultivariate analysisOdds RatioP value (< 0.05)Odds RatioP value (< 0.05)Age1.013 (1.005–1.022)< 0.0011.004 (0.993–1.016)0.46Gender Female1.00 (reference)0.27 Male1.137 (0.904–1.431)ECOG Performance Status 0–21.00 (reference)< 0.001-0.23 Status 3–42.322 (1.534–3.516)1.347 (0.827–2.192) Body Mass Index (BMI)0.999 (0.976–1.023)0.95- Charlson Comorbidity Index (CCI)1.200 (1.142–1.261)< 0.0011.117 (1.055 – 1.184)< 0.001ASA Score 1 or 21.00 (reference)< 0.001-< 0.001 3 or 42.017 (1.612–2.523)1.554 (1.193 – 2.026)Preoperative > 10% Weight Loss No1.00 (reference)< 0.001-0.04 Yes1.487 (1.190–1.857)1.287 (1.010 – 1.641) Total number of harvested Lymph nodes0.993 (0.985–1.000)0.060.990 (0.982 – 0.998)0.02 Duration of Surgery (minutes)1.003 (1.002–1.004)< 0.0011.004 (1.003 – 1.005)< 0.001Pathology Anatomic Stage (a) 0, Ia and Remission1.00 (reference)- Ib-IIIc1.200 (0.888–1.622)0.241.041 (0.753–1.440)0.81 IV2.791 (1.713–4.548)< 0.0011.791 (1.034 – 3.103)0.04Surgical approach Open1.00 (reference)0.11 Minimally invasive0.834 (0.669–1.039)Margin Status R01.00 (reference)< 0.001-0.02 R1 or R21.823 (1.311–2.534)1.586 (1.083 – 2.323)Values in parentheses are 95 per cent confidence intervals; ECOG Eastern Cooperative Oncology Group(a) James D. Brierley (Editor) MKG (Editor), CW (Editor). TNM Classification of Malignant Tumours, 8th Edition. Wiley-Blackwell; 2017
Most deaths were associated with general complications (77.8%), and almost half of all 90-day follow-up deaths had both surgical and general complications occurring in the postoperative period. Anastomotic leak (non-duodenal) was the leading cause of death, representing 24.4% (n = 11) of all mortality (n = 45), 1.5 times more than duodenal leaks.
The median hospital stay was 8 days (IQR 6–11). The readmission rate was 10.6%, and the 90-day reoperation rate was 8.1% (n = 124). Reoperations were mainly performed for non-duodenal anastomotic leaks (31.5%), postoperative haemorrhage (16.9%), and duodenal leaks (10.5%).
Discussion
This large, multinational, prospective study of 1538 gastric cancer patients found that elective gastric cancer surgery with curative intent has a 90-day morbidity and mortality of 38.2% (n = 587) and 2.9% (n = 45), respectively. We found that higher CCI, ASA score 3 or 4, severe pre-operative weight loss pathologically confirmed metastatic disease (stage IV), and positive (R1 or R2) margins are significantly associated with clinically relevant 90-day morbidity and mortality, as showed in Chart 1. Additionally, a higher number of lymph nodes retrieved emerged as a potential protective factor in the final model; however, the effect was marginal and not clinically meaningful, as the number of harvested lymph nodes was only weakly associated with reduced odds of 90-day clinically relevant morbidity and mortality (OR = 0.99; 95% CI = 0.982–0.998). Likewise, procedure duration, with an odds ratio close to 1, presented no meaningful association with 90-day morbidity and mortality.Chart 1Forest plot representing the odds ratio of multivariate analysis of each specific variable's impact on the outcome (90-day morbidity and mortality, CD II-V). Error bars indicate the confidence intervals (CI). Ngg Total Total number of harvested Lymph Nodes. Ib-IIIc and IV reporting AJCC TNM Staging
The 90-day morbidity rate of 38.2% was consistent with previous studies, ranging from 6.3% to 43% [13, 19, 20]. Cats et al*.* reported lower 30-day morbidity rates at 22–28% [39], and Baiocchi et al. reported a 90-day morbidity rate of 29.8% [40]. However, our study reported lower clinically significant morbidity rates (CD II-IV) (26.2%) compared to these studies, including the PRESTO study [26], with fewer events per patient (1.3 vs. 1.5) [40]. Non-surgical infections (4.7%) and anastomotic leak (n = 70) were the most common causes of morbidity, as observed in other studies [13, 32].
Our study reported a 2.9% mortality rate, which is lower than previously reported figures, including 3.4% in Peltrini et al. [41] and a range of up to 12.5% in Baiocchi et al. [40]. This may reflect advances in perioperative care and surgical techniques, as observed in more recent prospective [23, 28, 42, 43] and randomised studies [21], suggesting an overall trend toward improved contemporary outcomes.
The reoperation rate was 8.1% in our study, similar to previous studies [40]. The higher comorbidity burden in our cohort may have contributed to a higher 90-day morbidity and mortality rate (Table 6). Although our cohort had a high comorbidity burden, as measured by the Charlson Comorbidity Index (CCI), the 90-day mortality rate was lower than that reported in previous studies [28, 29, 44], suggesting that high comorbidity did not necessarily translate into higher mortality in our population. This finding is consistent with reports highlighting the role of pre-operative prehabilitation and careful patient selection [7, 15]. Such strategies are increasingly recognised for their role in optimising care for high-risk patients and potentially mitigating the impact of comorbidities on surgical outcomes.
Advanced disease defined as metastatic involvement identified intraoperatively or on final pathology (p = 0.0001), and positive surgical margin (p = 0.0004) were both significantly associated with clinically relevant 90-day morbidity and mortality, with almost threefold increase in risk. These findings highlight the importance of carefully balancing the extent of surgical intervention against palliative approaches, taking into account optimal pre-operative staging, patient life expectancy, and individual expectations. In this cohort, patients were deemed suitable for surgery based on ASA and ECOG criteria. However, over half of the cohort had a CCI of 5 or higher. Recognised surgical quality indicators [13, 32] such as R0 resection, D2 lymphadenectomy, and retrieval of > 15 lymph nodes were achieved in the present cohort in 89.1%, 63.1% and 79.1% of the patients, respectively.
In the Western world, unlike in the East, the absence of screening protocols results in the rare early detection of gastric cancer [44]. In our study, locally advanced gastric cancers (stage Ib and above) accounted for the majority of patients (74.2%; n = 1141) at postoperative pathological assessment.
The approach to intra-abdominal complications primarily involved conservative management, similar to previous studies [29], with 21.9% (n = 80) of cases undergoing drainage via endoscopic or interventional radiology. A smaller proportion (8.1%) required reoperation during the same hospital admission. These patients had a significantly higher mortality rate (p < 0.001), likely reflecting the severity of the underlying complication and the additional risk associated with re-exploration in clinically unstable individuals.
This study also highlighted differences in treatment and outcomes between duodenal and non-duodenal leaks [40], with the latter necessitating more frequent (55.7%) reoperations and more extended hospital stays (with an average delay of 9 days). Non-duodenal leakage has been reported in previous studies, with a reported incidence ranging from 2 to 11%. It was the leading cause of death in our study, representing 24.4% of all mortality, 1.5 times more than duodenal leaks.
Clavien–Dindo grade ≥ II complications were the primary determinant of prolonged hospital stay (mean > 14 days), particularly in patients undergoing total gastrectomy or experiencing an anastomotic leak (mean stay of 28.1 ± 19.7 days). The overall readmission rate was low (10.6%) and was most related to intra-abdominal collections following subtotal gastrectomy.
Although age was significantly associated with clinically relevant 90-day morbidity and mortality in univariate analysis, as seen in previous studies in the literature [45, 46], it did not remain significant in the multivariate model (p = 0.078). This may reflect confounding or collinearity with other age-related variables such as ASA score and Charlson Comorbidity Index, which remained independently associated with adverse outcomes and may better capture physiological vulnerability in this cohort [47, 48].
Notably, patients aged ≥ 70 years had nearly double the 90-day mortality rate (5.1%) compared to their younger counterparts, reinforcing the clinical relevance of age despite statistical adjustment. Among patients who were ≥ 70 years old and died, 96.8% (n = 18) had a CCI ≥ 5, and most also presented with severe preoperative weight loss.
Ensuring high standards of surgical care involves not only reducing complication rates but also effectively managing complications when they occur, thereby preventing their escalation to critical events or death. The observed combination of significant morbidity and low mortality in our cohort reflects this capacity to 'rescue' patients — a recognised quality indicator in modern surgical practice [7].
Strengths and weaknesses
This study offers a comprehensive and contemporary overview of real-world 90-day morbidity and mortality after curative gastric cancer surgery, using prospective data from a broad and diverse international cohort. Its novelty lies in the combination of scale, geographical diversity, and standardised complication classification, enabling the identification of clinically relevant predictors across different surgical approaches and health systems. Rather than focusing on a single technique or setting, it reflects current global practice and provides meaningful insights into perioperative risk factors applicable across varied contexts. However, data inconsistencies may arise from structural database flaws or institutional apprehension about high complication rates and inadequate follow-up. The classification of lymphadenectomy as D1, D1 + or D2 was based on the operating surgeon’s intraoperative judgement and documentation, without central validation. This subjective assessment may not always correspond to the final number of lymph nodes retrieved, which is also influenced by pathological processing and institutional practices. Variability in patient demographics contributed to wide standard deviations, and the absence of systematic data on patient optimisation before reintervention and on the timing of such interventions limits our ability to assess their impact on outcomes. Given the heterogeneity across participating institutions and the absence of standardised treatment pathways, our findings should be interpreted as a reflection of real-world practice. Future research should aim to examine how institutional characteristics and care models impact surgical outcomes in gastric cancer. Comparative studies between Eastern and Western treatment strategies would be valuable.
Conclusion
Elective gastric cancer surgery was associated with 90-day morbidity of 38.2%, with a total of 26.2% classified as clinically relevant (CD II-IV), and 90-day mortality of 2.9% in this global cohort. Factors associated with this morbidity and mortality (CD II-V) included a higher CCI, a higher ASA score, pre-operative severe weight loss, pathological confirmation of metastatic disease, and a positive margin. These findings reflect real-world variability and underscore the importance of understanding how institutional and regional factors influence surgical outcomes.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (PDF 446 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferlay J, Ervik M, Lam F et al (2024) Global cancer observatory: cancer today, international agency for research on cancer. https://gco.iarc.who.int/today. Accessed 12 Jan 2024
- 2Omarov N, Uymaz D, Azamat I F, et al (2021) The role of minimally invasive surgery in gastric cancer. Cureus 13(11):e 19563. 10.7759/cureus.1956310.7759/cureus.19563 PMC 859086034796082 · doi ↗ · pubmed ↗
- 3Marano, Luigi et al (2023) Current trends in volume and surgical outcomes in gastric cancer. J. Clin. Med 12(7):2708. 10.3390/jcm 1207270810.3390/jcm 12072708 PMC 1009477637048791 · doi ↗ · pubmed ↗
- 4Hang LN, Mc Millian N, Stein ME, et al (2024) NCCN Clinical practice guidelines in oncology: gastric cancer. Version 3.2023. National Comprehensive Cancer Network. Available at: https://www.nccn.org
- 5Dal Cero, Mariagiulia et al (2022) Textbook outcome and survival after gastric cancer resection with curative intent: A population-based analysis. Eur J Surg Oncol 48(4):768–775. 10.1016/j.ejso.2021.10.02510.1016/j.ejso.2021.10.02534753620 · doi ↗ · pubmed ↗