Hybrid laparo-endoscopic techniques for challenging colorectal lesions: a systematic review
Giovanni Distefano, Carlo Alberto Ammirati, Michele Barbiero, Roberto Passera, Alberto Arezzo

TL;DR
Hybrid laparoscopic-endoscopic techniques offer a safe and effective alternative for complex colorectal lesions that cannot be treated with standard endoscopic methods.
Contribution
This study systematically reviews the safety and efficacy of hybrid laparoscopic-endoscopic techniques for challenging colorectal lesions.
Findings
Hybrid techniques had low complication and recurrence rates for complex colorectal lesions.
Unexpected adenocarcinoma was found in 12% of resected lesions, highlighting the need for intraoperative adaptability.
Conversion to open surgery occurred in only 2% of cases, showing the minimally invasive nature of these techniques.
Abstract
Colorectal cancer screening has increased the detection of polyps requiring resection, but standard endoscopic techniques such as endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) are often unsuitable for large, fibrotic, or anatomically challenging lesions. Segmental colectomy remains definitive but carries substantial morbidity, particularly for benign disease. Laparo-endoscopic cooperative surgery (LECS) and related hybrid techniques have emerged as minimally invasive alternatives bridging the gap between endoscopic and surgical resection. A systematic review was performed according to PRISMA guidelines, querying PubMed, Embase, and Cochrane databases (1985–2024). Studies reporting combined laparoscopic-endoscopic resections for colorectal lesions unsuitable for standard endoscopic treatment were included. Outcomes assessed included additional surgery,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
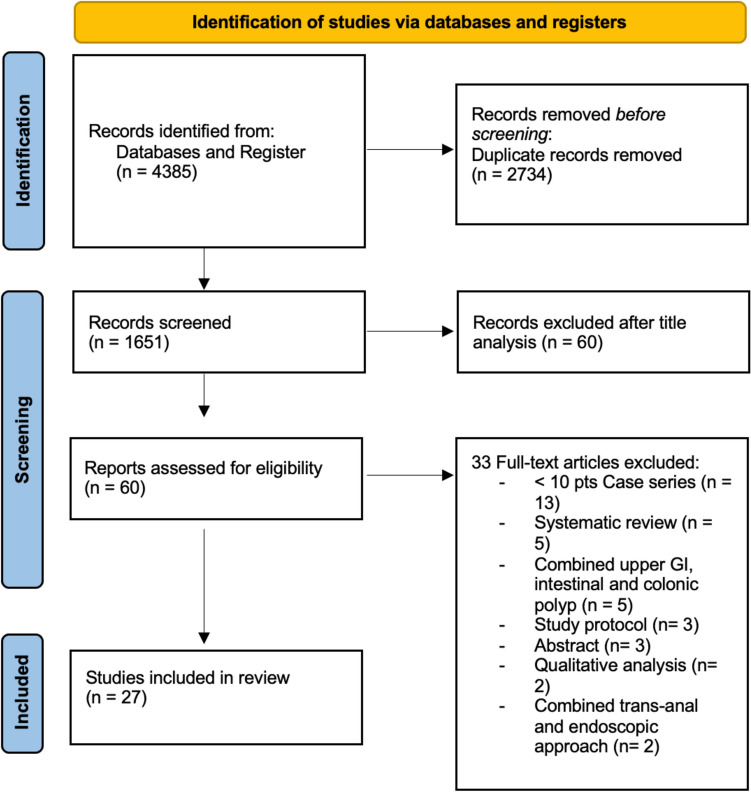 Figure 1
Figure 1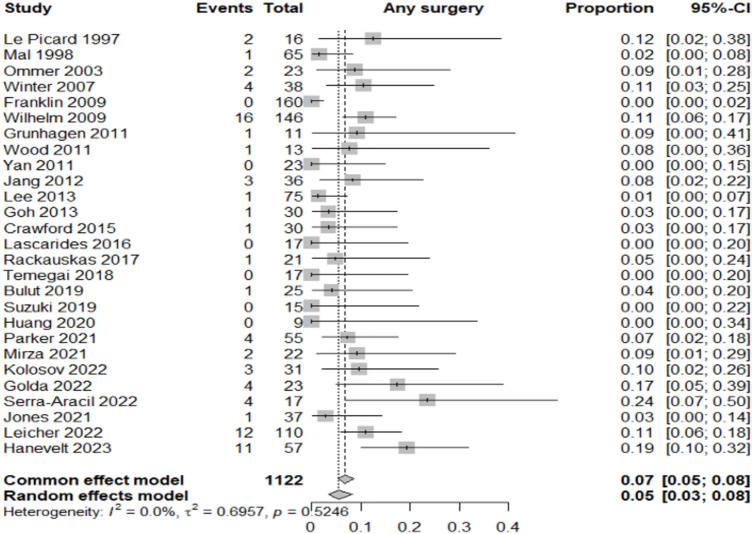 Figure 2
Figure 2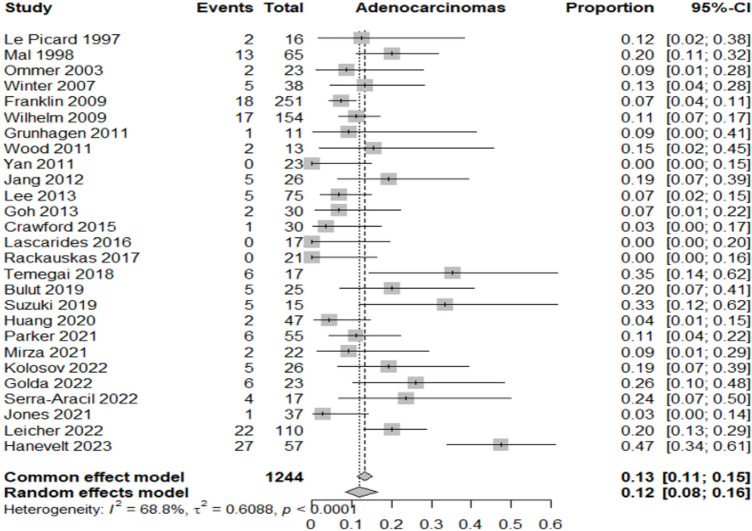 Figure 3
Figure 3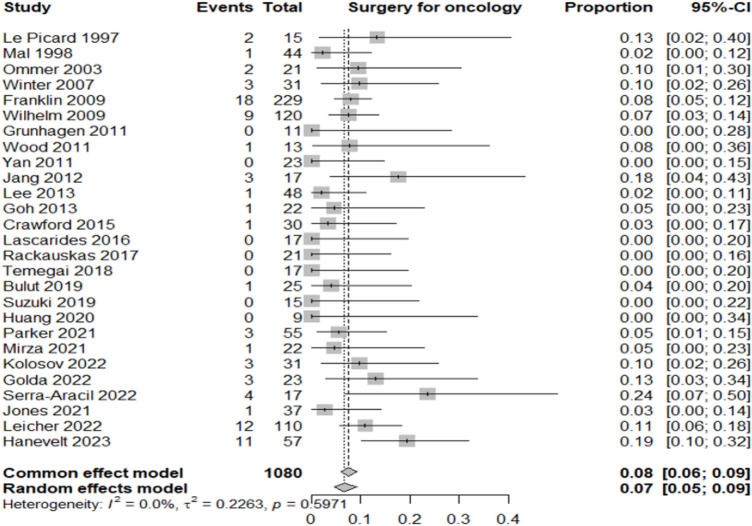 Figure 4
Figure 4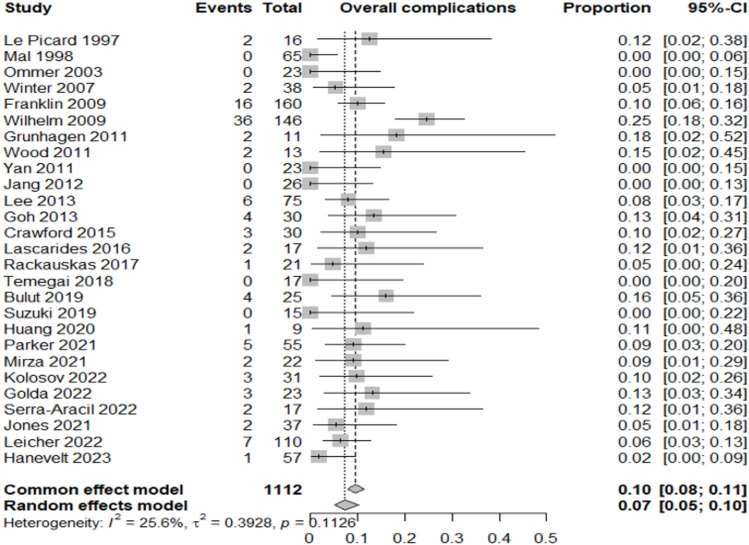 Figure 5
Figure 5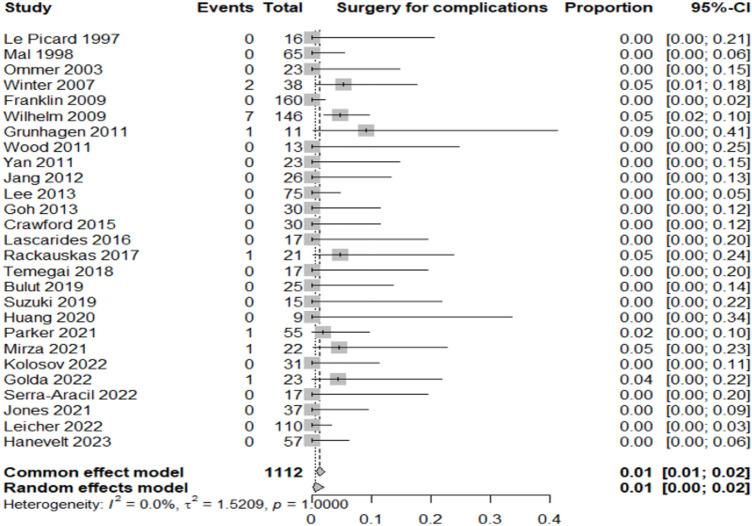 Figure 6
Figure 6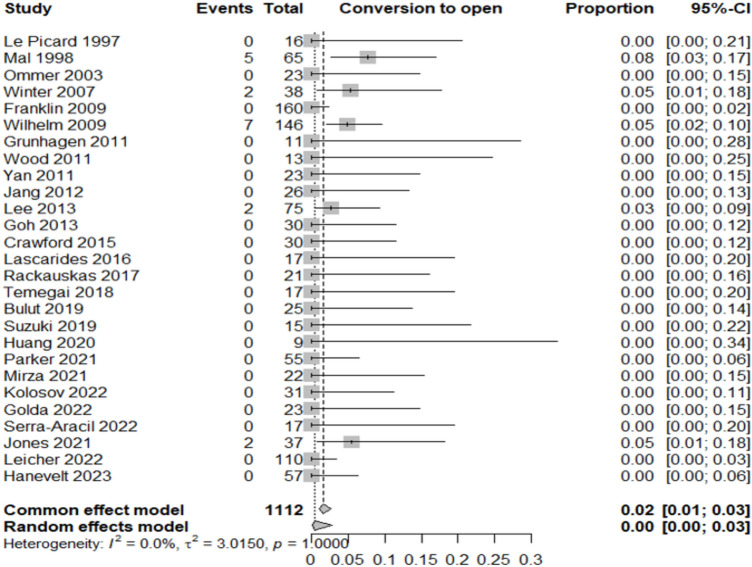 Figure 7
Figure 7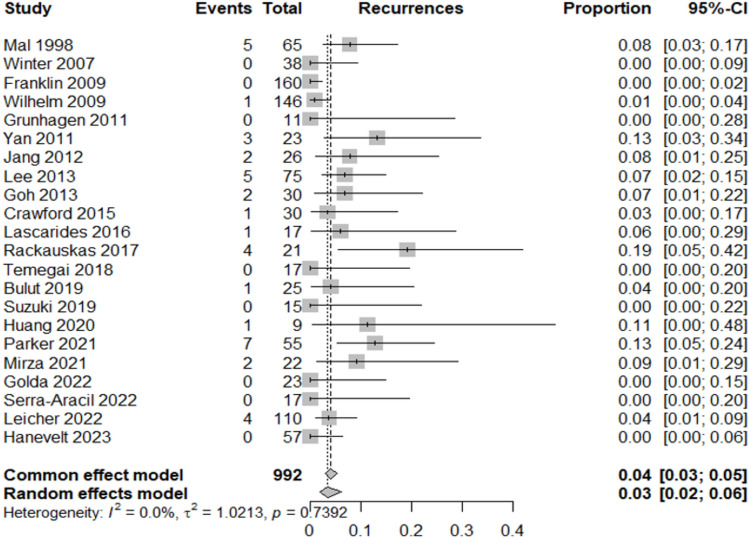 Figure 8
Figure 8 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Colorectal Cancer Screening and Detection
Colorectal cancer (CRC) is the third most diagnosed malignancy and the second leading cause of cancer-related death globally. Worldwide, over 1.920.000 new CRC cases were reported in 2022 with approximately 904.000 deaths attributed to the disease [1]. Despite an overall decline in both incidence and mortality due to increased screening and improved management, regional disparities persist, largely reflecting unequal implementation of screening programs and differences in risk factor profiles [2].
The adenoma–carcinoma sequence remains the fundamental model for CRC development, with the majority of cancers arising from pre-existing adenomatous polyps or sessile serrated lesions [3]. Accordingly, early detection and endoscopic removal of these lesions represents the most effective strategy to reduce CRC incidence and mortality [4]. Large-scale colonoscopy screening programs have significantly increased the detection rate of colorectal polyps, leading to widespread adoption of endoscopic resection techniques such as polypectomy, endoscopic mucosal resection (EMR), and endoscopic submucosal dissection (ESD). These techniques are generally safe and effective; however, they may not be feasible for all lesions.
Large-scale colonoscopy screening programs have significantly increased the detection rate of colorectal polyps, leading to widespread adoption of endoscopic resection techniques such as endoscopic mucosal resection (EMR), and endoscopic submucosal dissection (ESD). These techniques are generally safe and effective; however, they may not be feasible for all lesions.
Large or “complex” polyps—typically defined as lesions > 20 mm, involving multiple folds or more than one-third of the colonic circumference, or located in anatomically challenging sites such as the right colon or near the ileocecal valve—are often associated with fibrosis due to prior resection attempts or are morphologically flat (e.g., lateral spreading tumors, LSTs). Such features substantially increase the technical difficulty and risk of complications during standard endoscopic resection. Additionally, piece-meal resection of large lesions often results in uncertain histopathological assessment and may compromise oncologic adequacy.
Although traditional surgical resection remains a definitive option for such difficult lesions, it is associated with increased morbidity and mortality, particularly in elderly patients or those with significant comorbidities. Segmental colectomy, while radical, is often unwarranted in cases of benign pathology. To bridge this gap, combined laparo-endoscopic approaches have been developed with the aim of minimizing surgical invasiveness while ensuring complete and safe resection of difficult colorectal lesions. Laparo-Endoscopic Cooperative Surgery (LECS) and similar collaborative procedures, including laparoscopically assisted endoscopic resection and endoscopic-assisted laparoscopic wedge or full-thickness resections, have gained attention in recent years. These techniques allow for intraoperative endoscopic localization and assessment of the lesion, laparoscopic control of the bowel wall, and selective full-thickness or transmural resection when needed. They offer the potential to preserve more bowel, avoid major colectomies, and enable immediate surgical management in the case of unexpected malignancy or perforation [5, 6].
Several retrospective and prospective series, as well as systematic reviews, have shown promising results in terms of efficacy, complication rates, and oncologic adequacy [7]. This evolving body of evidence highlights the potential role of laparo-endoscopic approaches in the management of complex colorectal neoplasia. However, considerable heterogeneity remains in terms of technique, indications, and reported outcomes. The present systematic review aims to assess the updated safety and efficacy profile of laparo-endoscopic resections for colorectal lesions that are considered unsuitable for standard endoscopic treatment, with a particular focus on recurrence, complications, oncologic outcomes, and the need for further interventions.
Material and methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [8].
Eligibility criteria
All studies published between January 1985 and December 2024 were eligible for inclusion if they reported on patients undergoing combined laparoscopic-endoscopic local resection of colorectal lesions. Eligible procedures included laparoscopically assisted endoscopic polypectomy, endoscopic-assisted laparoscopic wedge or full-thickness resection, and other minimally invasive techniques aimed at removing colorectal lesions unsuitable for standard endoscopic treatment.
Studies were excluded if they involved extended colorectal resections (e.g., segmental colectomies or hemicolectomies), included fewer than 10 patients, were animal studies, reviews, editorials, position papers, conference abstracts, or book chapters. In cases of suspected patient cohort overlap, only the most recent or complete publication was included.
Search strategy
A comprehensive literature search was conducted in May 2025 using Embase, PubMed, and the Cochrane Central Register of Controlled Trials. The search string was specifically developed for this review and included terms related to laparoscopy, endoscopy, polypectomy, and colorectal lesions. The complete search strategy is provided as an appendix to this manuscript (Appendix 1).
Study selection and data extraction
Two reviewers (GD, MB) independently screened all studies in a three-step process: first by title, then by abstract, and finally through full-text review of potentially eligible articles. Screening and selection were conducted using the Rayyan platform. Any discrepancies were resolved by consensus with a third reviewer (CAA).
Data extraction was independently performed by the same two reviewers using pre-defined data collection forms. Extracted variables included study design, country, sample size, patient demographics, lesion characteristics, surgical technique, recurrence, complications, conversion to open surgery, adenocarcinoma detection, and need for additional surgery (either for complications or oncologic reasons).
Outcomes
The primary outcome of interest was the rate of additional surgery following combined laparoscopic–endoscopic resection. This included both reoperations for postoperative complications and surgeries performed to achieve oncologic radicality.
Secondary outcomes included:
- Incidence of adenocarcinoma in the resected specimens
- Rate of additional oncologic surgery
- Overall complication rate
- Rate of surgery due to complications
- Conversion rate to open surgery
- Recurrence rate after local resection
Each outcome was calculated as the proportion of lesions or patients meeting the criteria relative to the total included in the corresponding category.
Quality assessment and statistical analysis
Risk of bias within individual studies was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool. Specifically, we evaluated the availability of histological reference standards, completeness of data regarding technical success, and reporting on oncologic adequacy.
Following a conservative approach, all outcomes were analysed by a random-effects model, where the proportions of single studies were used to calculate an overall proportion. This model incorporates heterogeneity among studies and takes into account differences in sample size by which proportions were measured in each study; this within-study variation was accounted for using the exact binomial distribution. Individual and pooled estimates of these proportions together with 95% confidence intervals (CIs) were presented in the Forest plots.
Publication bias was assessed by generating a funnel plot and performing the rank correlation test of funnel plot asymmetry. Heterogeneity was assessed by the I^2^ measure of inconsistency, statistically significant if I^2^ > 50%. Potential sources of heterogeneity were explored by two sensitivity analyses: checking the results of cumulative (sequentially including studies by date of publication) and influence analyses (calculating pooled estimates by omitting one study at a time). All analyses were performed using R 4.5.1 package meta (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 27 studies encompassing 1112 patients were included. A flow diagram of this systematic review, with the number of papers retrieved, included and excluded, as well as the reasons for exclusion, is shown in Fig. 1.Fig. 1. Flow-chart of the literature search in this systematic review
A developed summary table (Table 1) includes the core characteristics of all studies included in this review. The characteristics of the studies and detailed QUADAS quality assessment are also summarized in Table 1 and Supplementary Table 1, respectively. QUADAS evaluation showed generally high methodological quality: 100% of studies met core criteria such as appropriate patient spectrum, adequate reference standard, short test-reference interval, and blinded interpretation of results. Some variability was observed in reporting of selection criteria and procedural details (items 2, 8, 9), with 8 studies showing partial or unclear reporting. Table 1. Core characteristics of all included studiesReferenceStudy designCountryInclusion periodMono/multicentricPatients, nMean age (years)Male (%)Le Picard (1997) [9]ProspectiveFrance1994–1996Monocentric1656–8056Mal (1998) [10]RetrospectiveFrance1990–1997Monocentric656258Ommer (2003) [11]RetrospectiveGermany1995–2002Monocentric2370.747.8H. Winter (2007) [12]ProspectiveGermany1998–2007Monocentric386655Wilhelm (2009) [13]ProspectiveGermany1997–2006Monocentric1466447Franklin (2009) [14]ProspectiveUSA1990–2008Monocentric16074.751DJ. Grunhagen (2011) [15]ProspectiveThe Netherlands2006–2009Monocentric1173.263Wood (2011) [16]ProspectiveUK2008–2009Monocentric136633Yan (2011) [17]RetrospectiveUSA2003–2008Monocentric237061Jang (2012) [5]RetrospectiveUSA/Monocentric2660.739Sang W. Lee (2014) [18]RetrospectiveUSA2003–2012Monocentric756943C. Goh (2014) [19]RetrospectiveIreland2010–2013Monocentric3065.460Crawford (2015) [20]RetrospectiveCanada2009–2013Monocentric306466Lascarides (2016) [21]ProspectiveUSA/Monocentric176352Račkauskas (2017) [22]RetrospectiveLithuania2010–2016Monocentric2165.3333Tamegai (2018) [23]RetrospectiveJapan2012–2018Monocentric1766.558Bulut (2019) [24]RetrospectiveNew Zealand2016–2017Monocentric257152S Suzuki (2019) [25]RetrospectiveSingapore2004–2017Monocentric156466ES Huang (2020) [26]RetrospectiveUSA2013–2017Monocentric959.766.6Parker (2021) [27]RetrospectiveUK2008–2018Monocentric556569Kasim L Mirza (2021) [28]RetrospectiveCalifornia2015–2020Monocentric226481.8Kolosov (2022) [29]ProspectiveRussia2019–2020Monocentric3167.893Golda (2022) [30]RetrospectiveSpain2010–2020Monocentric2369.982.6Serra-Aracil (2022) [31]RetrospectiveSpain2018–2020Monocentric176958L W Leicher (2022) [32]ProspectiveThe Netherland2017–2019Multicentric1106656Austin T Jones (2021) [33]RetrospectiveUSA2018–2019Monocentric376759.5Julia Hanevelt (2023) [34]RetrospectiveThe Netherlands2015–2022Monocentric5769.561.4
Reporting of outcomes by specific hybrid technique was inconsistent across studies. For example, *Serra-Aracil *et al. [31] described different variants of combined endoscopic-laparoscopic surgery, including full-thickness resections and laparoscopically assisted resections, but did not provide stratified complication or recurrence rates. Similarly, *Suzuki *et al. [25] and *Tamegai *et al. [23] reported on LECS-CR procedures but presented results in aggregated form without separation by technique. This variability precluded meaningful subgroup analysis and limited the possibility of comparing outcomes across different hybrid approaches. For conceptual clarity, however, the hybrid procedures can be broadly categorized into three groups: (a) laparoscopically assisted EMR, (b) endoscopic-assisted laparoscopic wedge/full-thickness resections, and (c) endoscopic-assisted segmental resections.
Primary outcome—additional surgery
The overall rate of additional surgery, including both oncologic and complication-related interventions, was 5% (95% CI 3–8%; I^2^ = 0%), indicating excellent inter-study consistency. This represents a substantial reduction compared to standard segmental resections and supports the feasibility of the combined approach (Fig. 2).Fig. 2. Forest plot for additional surgery
Secondary outcomes
Table 2 summarizes the proportion of lesions or patients meeting each outcome relative to the total included in the corresponding category.
- Adenocarcinoma detection rate: adenocarcinoma was identified in 12% of resected lesions (95% CI 8–16%; I^2^ = 68.8%), highlighting significant heterogeneity in preoperative diagnostic accuracy across studies (Fig. 3).
- Oncologic surgery requirement: following local resection, 7% of patients (95% CI 5–9%; I^2^ = 0%) required radical oncologic surgery, primarily due to invasive histology (Fig. 4).
- Overall complication rate: complications occurred in 7% of patients (95% CI 5–10%; I^2^ = 25.6%), mainly bleeding, perforation, and localized infections (Fig. 5).
- Surgery for complications: surgical management was necessary in 1% of cases (95% CI 0–2%; I^2^ = 0%) (Fig. 6).
- Conversion to open surgery: conversion was required in 2% of procedures (95% CI 1–3%; I^2^ = 0%), confirming good intraoperative control even in technically challenging situations (Fig. 7).
- Local recurrence: long-term follow-up of 992 patients showed a local recurrence rate of 3% (95% CI 2–6%; I^2^ = 0%), indicating durable local control (Fig. 8). Table 2. Main results of the analyzed outcomesAnalyzed variablesValue (%)95% CII^2^ (%)Recurrence rate32–60Adenocarcinoma detection rate128–1668.8Overall complications rate75–1025.6Surgery for complications10–20Conversion to open surgery21–30Oncologic surgery requirement75–90Fig. 3Forest plot for adenocarcinoma detection rateFig. 4Forest plot for surgery for oncological reasonFig. 5Forest plot for overall complications rateFig. 6Forest plot for surgery for complicationsFig. 7Forest plot for conversion to open surgeryFig. 8Forest plot for local recurrence rate
Follow-up duration was reported in 18 out of 27 studies, with a median of 20 months (range 1–196 months). Although reporting methods varied across studies, a sensitivity analysis restricted to studies with at least 12 months of follow-up yielded recurrence rates comparable to the overall analysis, thereby confirming the robustness of our results.
Discussion
This systematic review confirms that combined laparoscopic-endoscopic techniques, such as LECS and its variants, are safe and effective for the treatment of complex colorectal lesions that are not suitable for standard endoscopic resection. Hybrid laparo-endoscopic approaches encompass a wide spectrum of techniques, ranging from laparoscopically assisted EMR to wedge or full-thickness resections and more limited segmental resections. Although some recent reports, such as Serra-Aracil et al. [31], have highlighted these variants, outcome measures were usually presented in aggregated form without stratification by technique. This lack of granularity precluded reliable meta-analytic comparison between procedural subtypes, and our pooled estimates should therefore be interpreted as representative of hybrid approaches as a whole rather than of individual procedures. With a pooled additional surgery rate of just 5% and consistent results across studies, this approach appears to provide a reliable organ-preserving alternative to traditional segmental colectomy, particularly when complete endoscopic resection is either infeasible or carries high risk. Recent technological advancements and growing expertise in the field of endoscopic resection of large superficial colorectal lesions are progressively reducing the need for surgical intervention. According to recent data from high-volume European centers, endoscopic submucosal dissection (ESD) achieves en bloc resection rates exceeding 85% even for lesions larger than 20 mm, although the true oncologic benefit is realized in only a limited subset of patients.
Endoscopic Submucosal Dissection (ESD) has been widely adopted for en bloc resection of superficial colorectal neoplasms; however, its clinical benefit is often undermined by the relatively high incidence of incomplete (R1) resections. Reported R1 rates in colorectal ESD range from 8 to 15%, largely due to technical challenges, fibrosis, and lesion morphology in the colon and rectum, which differ substantially from gastric ESD where en bloc R0 rates exceed 90% [35–37]. Incomplete resection not only negates the oncologic advantage of ESD by leaving positive margins but also necessitates additional interventions, either repeat endoscopic procedures or radical surgery, thereby increasing morbidity [38]. Moreover, several studies have shown that R1 resections are associated with a significantly higher risk of local recurrence compared to R0 resections [39]. These limitations underscore the need for careful patient selection and technical refinement, as well as the potential role of hybrid laparoscopic-endoscopic approaches to ensure complete full-thickness resection in anatomically or technically challenging lesions [40]. Specifically, the primary oncologic advantage of ESD over endoscopic mucosal resection (EMR) is seen in cases of well-differentiated adenocarcinomas with superficial submucosal invasion and no lymphovascular involvement. However, due to its technical complexity and higher risk of adverse events, ESD should be reserved for lesions with a high suspicion of early submucosal invasion [41]. In most other cases, piecemeal EMR remains a safe and sufficient option for removing large (> 2 cm), sessile or flat colonic lesions. If histology reveals invasive adenocarcinoma beyond the mucosal layer, radical surgery is recommended. Conversely, the presence of dysplasia at the resection margin does not justify surgery but rather calls for close endoscopic follow-up.
The findings also highlight that a significant proportion of lesions presumed benign—approximately 12%—were found to harbor adenocarcinoma on final pathology. The heterogeneity observed in the pooled incidence of adenocarcinoma is mainly attributable to differences in diagnostic accuracy and patient selection across studies. In most series, adenocarcinoma was diagnosed only a posteriori on the final resection specimen, whereas preoperative biopsies rarely guided the indication for hybrid resection and were reserved for patients unfit for extended colectomy. As endoscopic biopsy usually samples only a fraction of the lesion, it may easily understage the true histology, explaining why invasive carcinoma was unexpectedly identified in lesions considered benign at endoscopy. For this reason, a reliable subgroup analysis stratifying lesions as benign versus malignant at baseline could not be performed, as such categories were not consistently available prior to resection. This diagnostic limitation must be acknowledged as a key contributor to the heterogeneity observed in the pooled analysis.
This underscores the limitations of current diagnostic modalities in precisely staging complex colorectal polyps, despite advances in imaging and biopsy techniques. Consequently, a second surgical procedure for oncologic radicality was necessary in 7% of cases. Intraoperative frozen section examination was not reported in any of the included studies. Consequently, adenocarcinoma was generally recognized only on final pathology of the hybrid resection specimen. Patients with such findings were then offered oncologic resection whenever clinically appropriate and acceptable. This highlights both the limits of current intraoperative decision-making and the potential for understaging with endoscopic biopsy, which samples only a small fraction of large or complex lesions. The absence of frozen section use in published series may have contributed to the proportion of patients requiring secondary oncologic surgery observed in this review. This outcome, while not negligible, remains acceptable in a clinical scenario where overtreatment through upfront colectomy can be avoided in the majority of patients. The long-term local recurrence rate of 3% (95% CI 2–6%; I^2^ = 0%) observed in this systematic review underscores the durability of local control achieved with these techniques. This exceptionally low rate, coupled with the absence of heterogeneity across included studies, highlights the oncologic reliability of these approaches when applied in appropriately selected patients. Such outcomes are comparable to, or even better than, those reported for standard surgical resections in early colorectal neoplasia, supporting their role as effective organ-preserving strategies. Moreover, the consistency of results across studies suggests that these techniques can deliver reproducible oncologic safety in different clinical settings, provided that meticulous patient selection and adherence to technical standards are ensured. Only relevant improvements in intraoperative staging of rectal cancer at the time of local excision, such as the use of fluorescence to better characterise tumour histology and invasiveness [42], or sampling of potential sentinel lymph nodes in the mesorectum [43–45], could significantly alter the perspective on organ-sparing techniques. Moreover, these techniques may take advantage of recent research in AI and computed tomography (CT) in assisting the preoperative localization of colorectal cancer resection surgery [46].
The complication rate observed in this review was low, with only 7% of patients experiencing adverse events and a mere 1% requiring surgical management of complications. These results compare favorably with those of standard surgical resection and suggest that laparo-endoscopic approaches maintain a favorable safety profile, even in anatomically challenging cases such as lesions located in the right colon, near the ileocecal valve, or involving previous fibrosis. Moreover, conversion to open surgery was required in only 2% of procedures, indicating that combined approaches are technically feasible and controllable when performed by adequately trained surgical and endoscopic teams. Perhaps most notably, the recurrence rate was just 3%, with excellent consistency across studies, suggesting durable local control and confirming the oncologic reliability of these techniques.
The methodological quality of the included studies was assessed using the QUADAS tool, which revealed an overall high level of internal validity. All studies adequately described the patient spectrum and ensured the independence and reliability of the reference standard. However, certain aspects, such as the clarity of selection criteria and the level of detail provided about index and reference test execution, were less consistently reported. These variations in reporting standards point to a broader need for methodological rigor and transparency in future research.
Despite these strengths, this review has several limitations that must be considered when interpreting the results. The majority of studies were retrospective and monocentric, often conducted in high-volume referral centers, which may limit generalizability to lower-volume or community settings. There was also considerable heterogeneity in the technical execution of the procedures classified under the laparo-endoscopic umbrella, ranging from endoscopic-assisted wedge resections to laparoscopically assisted EMR and full-thickness resections. Follow-up periods varied across studies, and long-term outcomes such as disease-free survival or metachronous lesion development were not systematically reported, making it difficult to draw firm conclusions about oncologic prognosis beyond recurrence. Only a few studies provided extended follow-up beyond 30 months [13, 14, 18, 23, 27], consistently reporting low local recurrence rates. Overall, the pooled recurrence rate across all studies was about 3%, suggesting durable local control and serving as a proxy for oncologic reliability. However, detailed long-term oncologic endpoints such as disease-free survival (DFS) and overall survival (OS) were rarely reported and inconsistently presented across studies. This gap limits the ability to establish oncologic equivalence with standard colectomy and underscores the need for prospective trials with standardized DFS and OS reporting. Furthermore, some studies lacked sufficient detail regarding inclusion criteria and procedural methodology, limiting the ability to stratify results by lesion type or location. Nevertheless, the consistency in core outcomes—such as low recurrence, minimal complications, and a stable rate of additional oncologic surgery—suggests that laparo-endoscopic approaches offer significant advantages when appropriately indicated and performed by experienced multidisciplinary teams.
Hybrid laparoscopic-endoscopic resection techniques emerge as a compelling option for the management of complex colorectal lesions that are not amenable to standard endoscopic removal. These hybrid approaches allow for effective and safe local treatment while minimizing the need for extensive bowel resection. The low rates of complications, recurrence, and conversion to open surgery observed across studies highlight their feasibility and reproducibility in expert settings. The not insignificant proportion of patients found to have invasive carcinoma underscores the need for accurate preoperative evaluation and appropriate intraoperative adaptability. Still, the overall outcomes suggest that the benefits of local, minimally invasive resection can be preserved even when a secondary oncologic surgery becomes necessary. Ultimately, laparo-endoscopic cooperative surgery should be considered an integral part of the therapeutic armamentarium for colorectal lesions, bridging the gap between pure endoscopy and radical surgery. Future prospective, multicenter studies with standardized definitions, longer follow-up, and consistent reporting are needed to refine indications and further establish the long-term oncologic safety of this evolving approach.
This systematic review provides robust evidence supporting the safety and efficacy of combined laparoscopic-endoscopic approaches, such as LECS and its variants, for the management of complex colorectal lesions not suitable for standard endoscopic resection. The findings align with recent trends in minimally invasive surgery, confirming the role of hybrid techniques as a bridge between endoscopic and formal surgical management.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 28 KB)Supplementary file2 (DOCX 22 KB)