Time to screen: rationale and roadmap for HFpEF screening in individuals with obesity
Anouk Achten, Lukas Peeters, Geert Verkoulen, Jerremy Weerts, Christian Knackstedt, Evert-Jan Boerma, Vanessa van Empel, Sandra Sanders-van Wijk

TL;DR
This paper argues for early screening for heart failure in obese individuals due to their higher risk and earlier onset of the condition.
Contribution
The paper proposes a rationale and roadmap for HFpEF screening in obesity, emphasizing earlier detection and tailored diagnostic approaches.
Findings
Obesity-related HFpEF occurs a decade earlier than in non-obese individuals.
Current diagnostic methods face limitations in detecting HFpEF in obese populations.
A stepwise screening pathway is proposed to improve early detection in obese individuals.
Abstract
Obesity is a major risk factor for heart failure with preserved ejection fraction (HFpEF) and is associated with a distinct pathophysiological phenotype. Individuals with obesity develop HFpEF on average a decade earlier than individuals without obesity. Despite this, systematic screening for HFpEF in individuals with obesity is not currently recommended in clinical guidelines. This review discusses the rationale for screening individuals with obesity for HFpEF, highlighting the rising prevalence of obesity-related HFpEF, its earlier onset, and its often under-recognized clinical presentation. We describe the specific pathophysiological mechanisms linking obesity to HFpEF, including inflammation, adipose tissue distribution, and hemodynamic alterations. Furthermore, we review the limitations of current diagnostic approaches in this population, including the interpretation of natriuretic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
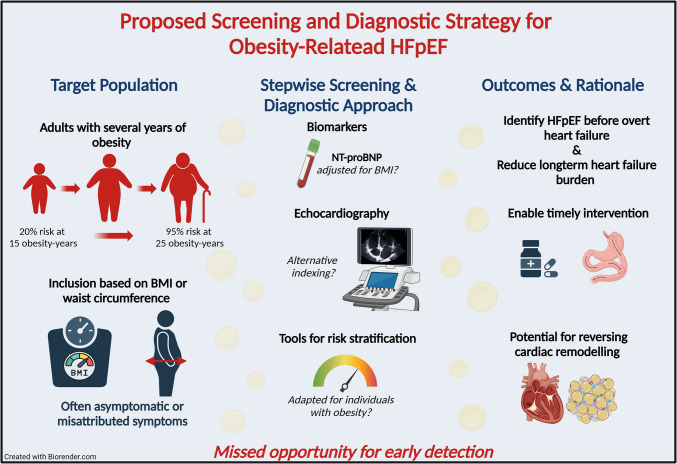 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Cardiovascular Disease and Adiposity · Cardiac Imaging and Diagnostics
Introduction
Obesity has become a global epidemic, impacting more than 650 million adults, and is a significant risk factor for various common and life-threatening conditions, including heart failure (HF) [1–3], particularly HF with preserved ejection fraction (HFpEF). The incidence of HF rises with age and excess weight, and obesity is notably prevalent in HFpEF patients, affecting approximately 48% of cases [4–6]. Moreover, the risk of developing obesity-related cardiac structural changes increases with the number of years a person has obesity—from 20% after 15 years to 95% after 25 years [7]. As a result, HFpEF in patients with obesity often develops at a younger age, typically a decade earlier than other HFpEF subtypes [7]. Consequently, individuals with obesity face a life-threatening disease at a relatively young age.
Early recognition and timely treatment of risk factors are crucial to prevent the development of HFpEF and, thereby, reduce significant disease burden for the patient as well as healthcare expenses. Since obesity is an important and highly treatable risk factor, the relationship between HFpEF and obesity has received more attention over the years. Nevertheless, most studies focus on the obese population already diagnosed with HFpEF. As a result, the prevalence of HFpEF in a general population with obesity is still relatively unknown. Moreover, the question of whether and how systematic screening for HFpEF in asymptomatic or mildly symptomatic individuals with obesity should be implemented remains unresolved. We will discuss in this review the value of screening as well as the bottlenecks and unmet needs in screening for HFpEF in individuals with obesity.
Pathophysiology of obesity-related HFpEF
Research has shown that patients with obesity-related HFpEF exhibit specific pathophysiological characteristics—such as increased right ventricular dysfunction, pericardial restraint, and more pronounced cardiac remodeling—and thus, obesity-related HFpEF is considered a specific phenotype called “obesity-HFpEF” [4, 8]. There is growing interest in elucidating the pathophysiological mechanisms by which obesity contributes to the development of HFpEF. Evidence suggests that, beyond the total amount of fat, the distribution of adipose tissue plays a crucial role in obesity-related disorders [9, 10], likely due to both metabolic and local mechanical effects [11]. Visceral adipose tissue is more commonly linked to metabolic dysfunction than subcutaneous fat, as adipocytes in visceral adipose tissue secrete adipokines that trigger monocyte and macrophage infiltration into visceral adipose tissue, contributing to both local and systemic inflammation [12–14]. Additionally, visceral adipose tissue accumulation is associated with excessive triglyceride deposition in the myocardium, as well as adipose tissue buildup in the epicardial and pericardial regions [15, 16]. HFpEF patients with obesity have an increased amount of epicardial adipose tissue, which also functions as a metabolically active reservoir that affects the myocardium by releasing inflammatory cytokines [9, 17, 18]. These cytokines contribute to low-grade inflammation in the body and negatively affect endothelial function [19], leading to microvascular dysfunction and fibrotic remodeling. While inflammation is known to be present in HFpEF overall, it has also been reported that patients with the obesity HFpEF phenotype exhibit higher levels of systemic inflammation compared to HFpEF patients without obesity [8].
Additional to the metabolic effects, there are local mechanical effects. Epicardial fat exerts a detrimental mechanical effect, particularly during diastole, by occupying space and potentially contributing to elevated intracardiac pressures in HFpEF patients with obesity [4]. As a result, the amount of epicardial adipose tissue accumulation is associated with an adverse prognosis in HF patients [20]. It is, however, still unknown which mediators contribute the most and at which stage of the disease process. Likely, an interplay between the metabolic activity of the adipocytes, their abundance, and their locations all impacts the systemic consequences and the cardiac response. Mediators in the early stages of the disease are particularly interesting for future targeted interventions.
Screening for heart failure in individuals with obesity
Screening for HF in individuals with obesity is not routinely performed, while screening for comorbidities in patients with established HF is recommended in current guidelines. Specifically, the current European Society of Cardiology (ESC) HF guidelines recommend screening for comorbidities such as diabetes, sleep apnea, and iron deficiency in patients diagnosed with HFpEF [21]. Similarly, the ESC cardiovascular risk management guidelines advise screening for diabetes in individuals with obesity and recommend assessing natriuretic peptides to detect HF in patients with diabetes [22]. However, no specific guidance is provided regarding HF screening in individuals suffering from obesity, but without diabetes, leaving a gap in current recommendations. The American Heart Association introduced a cardio-kidney-metabolic framework that emphasizes the importance of screening for HF in individuals with cardiometabolic risk profiles, including those with obesity, diabetes, and chronic kidney disease [23]. Although their approach incorporates kidney function and focuses broadly on multimorbidity, it supports the principle of proactive identification and intervention in at-risk individuals, in alignment with the screening rationale discussed here. Recently, a screening score for HFpEF has been developed, prior to employing natriuretic peptides or echocardiography, which includes obesity as a risk factor. The HFpEF-ABA score incorporates three clinical factors—age, body mass index (BMI), and a history of atrial fibrillation—to efficiently assess the likelihood of underlying HFpEF and identify patients who should be referred for an echocardiogram [24]. This suggests that screening for HF could be integrated into the care of patients with obesity; however, how effective this screening approach is in a population with obesity remains uncertain.
Signs and symptoms for heart failure
Screening for HF is often performed in the presence of signs and symptoms of HF. A preliminary small study indicates that 31% of a population with obesity (BMI ≥ 30 kg/m^2^) and dyspnea symptoms meets the HFpEF criteria according to echocardiogram and invasive right heart catheterization [25]. Nevertheless, it is still unknown how many patients with obesity already exhibit signs of HFpEF without being symptomatic (early stage or “early-HFpEF”). Relying on signs and symptoms for HF might not be the best approach, as symptoms are often attributed to obesity itself, potentially leading to underdiagnosis. Common HF symptoms, such as shortness of breath, reduced exercise capacity, and fluid retention—manifesting as weight gain and ankle swelling—are also frequently observed in individuals with obesity due to excess body weight [26–28]. This overlap makes it challenging to distinguish whether symptoms are driven by HFpEF or are solely a consequence of obesity, complicating the diagnostic process. Furthermore, patients with obesity often have difficulty engaging in physical activity due to musculoskeletal issues, such as joint pain and osteoarthritis, which cause discomfort and reduced mobility. As a result, they may not notice exertional breathlessness, leading to underreported symptoms and potential delays in diagnosis [29].
Screening with natriuretic peptides
Natriuretic peptides, such as B-type natriuretic peptide (BNP) and N-terminal pro B-type natriuretic peptide (NT-proBNP), are crucial biomarkers for diagnosing HF and are incorporated into the ESC guidelines for diagnosing HFpEF [21]. It has been demonstrated that circulating levels of natriuretic peptides are lower in individuals with obesity, regardless of the presence of acute decompensated HF. However, these levels remain above the threshold used to rule out chronic HF [8, 30]. Several studies have shown that a proportion of HFpEF patients present with natriuretic peptide levels below the diagnostic threshold in whom the BMI is often increased [31, 32]. More recently, a multicenter study confirmed that in patients with unexplained dyspnea and invasively confirmed HFpEF, the sensitivity of the ESC-recommended NT-proBNP cutoff of 125 pg/mL decreased from 77 to 67% among those with BMI > 35 kg/m^2^. Of note, 48–63% of these patients were on baseline diuretics, which may also influence natriuretic peptide levels [33]. To conclude, it is well known that natriuretic peptides are influenced by factors such as obesity, kidney function, age, and sex [34] in patients without HF. These findings support that natriuretic peptide thresholds may require adjustment in obese HFpEF, though prospective screening studies in diuretic-naïve populations are needed to establish reliable diagnostic cutoffs without influence of diuretics.
Screening with echocardiography
Measuring natriuretic peptides alone is insufficient to diagnose HFpEF in the absence of acute decompensated HF; therefore, an echocardiogram is the next step in the diagnostic process. Two established scoring systems for HFpEF diagnosis [35, 36] incorporate various echocardiographic parameters, including E/e′ to assess diastolic dysfunction, left atrial volume index, left ventricular mass index, and estimated right ventricular pressure. The HFA-PEFF (Heart Failure Association Pretest Probability of Heart Failure with Preserved Ejection Fraction) and H2FPEF (heavy, hypertension, atrial fibrillation, pulmonary hypertension, elder, and filling pressures) scores assist in diagnosing HFpEF by quantifying its risk through a numerical scoring system. However, both scores classify a significant proportion of suspected HFpEF patients as having an intermediate likelihood, for whom further diagnostic testing is recommended [37, 38]. Thus, the choice of scoring system determines which patients are referred for additional testing or classified as having HFpEF, potentially leading to different clinical decisions. Atrial fibrillation and BMI were the main contributors to the discrepancy between the scores as both are key components of the H2FPEF score, while atrial fibrillation increases the diagnostic threshold for HFpEF in the HFA-PEFF score by increasing the NT-proBNP cutoff [35–37]. Therefore, it is advised that both scores are used next to each other [37]. A diagnosis of HFpEF is confirmed if either score is high, whereas HFpEF is excluded if both scores are low. The actual diagnostic performance of these scores in a specific population with obesity is unknown. In cases of an intermediate score, additional assessment with stress exercise echocardiography or invasive hemodynamic measurements is recommended. However, invasive right heart catheterization may carry a higher risk of complications in patients with severe obesity [39]. Also, performing echocardiography in individuals with obesity presents its challenges. Excess adipose tissue can attenuate ultrasound waves resulting in poor image quality [40]. Nevertheless, when the technician is given adequate time to apply necessary technical adjustments, the majority of key parameters can still be accurately assessed [27]. Additionally, adjusting echocardiographic parameters for body surface area (BSA) might be unreliable in individuals with obesity. Since BSA is largely determined by fat mass, this correction may lead to an overestimation of parameters indexed to BSA—such as left atrial volume—potentially diminishing the observed abnormalities [41]. Previous studies have therefore suggested indexation of left atrial volume to height^2^ and left ventricular mass to height^2.7^ [42, 43].
HFpEF likelihood scoring in individuals with obesity
It is indeed possible to consider using another scoring system in individuals with obesity, though it still needs to be validated. Recently, a new scoring system was developed using machine learning, identifying BMI, estimated glomerular filtration rate, left ventricular mass index, and the left atrial to left ventricular volume ratio as the strongest predictors of HFpEF in obese patients [44]. This new scoring system was shown to outperform the H2FPEF score but was not compared to the HFA-PEFF score. Moreover, the control group in this study consisted of asymptomatic patients, raising uncertainty about how the score will perform in real-life clinical scenarios where HFpEF is suspected based on symptoms or other clinical, laboratory, or imaging findings. Additionally, the median BMI of the control group was 26.99, considerably lower than that of the HFpEF patients included in the study, which may impact the usage of this score to screen patients with obesity for HFpEF.
Proposed screening algorithm
Screening for HFpEF in individuals with obesity holds substantial promise, yet several barriers must be addressed before it can be broadly implemented. An initial step may involve population-level risk stratification using clinical tools such as the HFpEF-ABA score, in combination with natriuretic peptide assessment. However, it is crucial to assess whether BMI is the most appropriate criterion or if waist circumference would be a better measure for selecting patients for screening, as it correlates more strongly with visceral and epicardial adipose tissue [45]. Individuals identified as high-risk can then undergo a targeted diagnostic work-up, including tailored echocardiographic evaluation that accounts for obesity-related limitations in image quality and indexing. Where diagnostic uncertainty persists, adjunctive testing—such as exercise stress echocardiography or invasive hemodynamic assessment—may be warranted. Nevertheless, prospective studies are warranted to investigate the prevalence of HFpEF in a population with obesity. These studies can also evaluate the current scoring systems and potentially lead to the development of a new score.
Treatment
Following the identification of Obesity-HFpEF through screening, initiation of treatment with sodium-glucose cotransporter-2 (SGLT2) inhibitors is appropriate. This is particularly relevant given that obesity often coexists with dysglycaemia and hypertension. SGLT2 inhibitors not only confer clinical benefits in HF symptoms and outcomes but also modestly reduce body weight, glycated hemoglobin, and blood pressure [46]. SGLT2 inhibitors demonstrate consistent efficacy in reducing the primary composite outcome of worsening heart failure or cardiovascular death across the entire BMI spectrum, as shown in the DELIVER trial [46]. Treatment with SGLT2 inhibitors was also associated with an improvement in symptoms, with a greater magnitude of benefit observed in patients with higher BMI. Moreover, SGLT2 inhibitors consistently induce a modest but significantly greater reduction in body weight among individuals with higher BMI compared to those with lower BMI [46].
Obesity represents a significant yet modifiable comorbidity in patients with HFpEF [20]. Notably, individuals with obesity-related HFpEF exhibit a worse prognosis compared to other phenotypes, even after adjustment for comorbid conditions [47]. Early identification of HFpEF in individuals with obesity, coupled with targeted interventions promoting effective weight loss, holds particular promise—not only for preventing progression to overt heart failure, but also for improving clinical outcomes and facilitating reverse cardiac remodeling. Metabolic bariatric surgery (MBS) has proven to be an effective treatment for obesity, providing sustained benefits and higher rates of weight loss than conventional approaches [48, 49]. Research in obese individuals without pre-existing HF has indicated that MBS significantly lowers the risk of developing HF compared to lifestyle interventions alone [50]. Additionally, observational studies suggest that in patients with established HF, MBS is associated with improved quality of life and a reduction in HF-related hospitalizations [51, 52]. However, these studies have not focused specifically on HFpEF. Also, the effects of MBS on parameters such as left ventricular mass, chamber size, and overall cardiac function have been inconsistently reported. It remains uncertain whether the improved outcomes following MBS are primarily driven by weight loss or also by direct improvements in underlying cardiac function or structure [53, 54].
Pharmacological therapy for obesity has increasingly been recognized as a key strategy in recent years. In 2023, a randomized study involving 529 patients with obesity (BMI > 30) and HFpEF demonstrated that treatment with semaglutide, a glucagon-like peptide-1 (GLP-1) agonist, led to an improvement in quality of life after 1 year [55]. However, it is well established that weight loss achieved with MBS significantly exceeds that of GLP-1 agonists, with average reductions of ~ 35% versus ~ 15%, respectively [49, 55]. In combination with glucose-dependent insulinotropic polypeptide (GIP), GLP-1 agonists can achieve weight reductions of up to 25% [56]. Moreover, tirzepatide, combination therapy of GLP-1 and GIP, showed to reduce left ventricular mass and epicardial adipose tissue [57]. Nonetheless, discontinuing GLP-1 agonists is associated with weight regain in approximately 70% of patients [58]. In contrast, MBS combined with lifestyle intervention is capable of maintaining weight loss after 5 years in over 85% of patients [49]. Nonetheless, the indication for MBS is typically limited to patients under 65 years of age, while the average age of a typical HFpEF patient is around 75 years old. However, screening for HFpEF in a population suffering from obesity could allow for earlier diagnosis.
The extent to which early diagnosis and timely intervention, particularly through effective weight reduction, can reverse cardiac remodeling in individuals with obesity-HFpEF remains insufficiently understood. It is also unknown whether a threshold exists beyond which myocardial structural changes become irreversible, despite metabolic improvement. Importantly, recent evidence suggests that GLP-1 receptor agonists—alone or in combination with GIP—as well as MBS may exert cardioprotective effects that extend beyond weight loss. These interventions have been shown to reduce systemic inflammation, improve endothelial function, and attenuate myocardial fibrosis, potentially translating into improved clinical outcomes in HFpEF patients regardless of weight trajectory [56, 59–61].
Conclusion
Systematic screening for HFpEF in individuals with obesity represents a clinically actionable opportunity to shift from late-stage recognition to proactive disease interception. Given the rising prevalence of obesity and its strong association with earlier onset and worse prognosis of HFpEF, timely identification of at-risk individuals is essential, especially with the availability of effective pharmacological and surgical therapies that may target underlying pathophysiologic mechanisms. A stepwise screening and diagnostic approach is proposed, beginning with clinical risk stratification and natriuretic peptide assessment, followed by echocardiographic evaluation tailored to the technical and interpretive challenges posed by obesity. Key research priorities include establishing obesity-specific thresholds for biomarkers, optimizing imaging indexation, and validating tailored diagnostic pathways. Prospective studies are now warranted to define the prevalence of (early) HFpEF in asymptomatic individuals with obesity, evaluate existing and emerging screening tools, and determine whether early diagnosis and intervention can halt or even reverse disease progression. Addressing these knowledge gaps could support guideline changes and ultimately reduce the burden of HFpEF in this growing patient group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bodenstab ML, Varghese RT, Iacobellis G (2024) Cardio-lipotoxicity of epicardial adipose tissue. Biomolecules 14(11)10.3390/biom 14111465 PMC 1159182039595641 · doi ↗ · pubmed ↗
- 2Weerts J, Mourmans SGJ, Barandiarán Aizpurua A, et al (2022) The role of systemic microvascular dysfunction in heart failure with preserved ejection fraction. Biomolecules 12(2)10.3390/biom 12020278 PMC 896161235204779 · doi ↗ · pubmed ↗