Violet Invader: Pediatric Soft Tissue Infection Caused by Chromobacterium violaceum
Zobiakhlui Chhakchhuak, B Lalrinpuia, George Lalthanmawia, TBC Ramengmawii

TL;DR
This paper reports the first case of a rare skin infection caused by Chromobacterium violaceum in a child in Mizoram, India.
Contribution
This is the first documented case of C. violaceum causing infection in northeastern India.
Findings
C. violaceum was isolated from a septic wound in a pediatric patient.
The infection presented as a skin and soft tissue infection that could progress to severe complications.
Abstract
Chromobacterium violaceum is a Gram-negative bacillus known to be a rare cause of human infection. The organism enters the body through skin injury and usually presents as a localized skin infection that can progress to multiple abscesses and multiorgan failure. To our knowledge, this is the first reported case of skin and soft tissue infection caused by C. violaceum in the northeastern state of India, Mizoram. The organism was isolated from a pus sample obtained from a septic wound located on the foot and thigh of a pediatric patient. Though considered rare, this case report indicates that C. violaceum can be a potential cause of infection.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
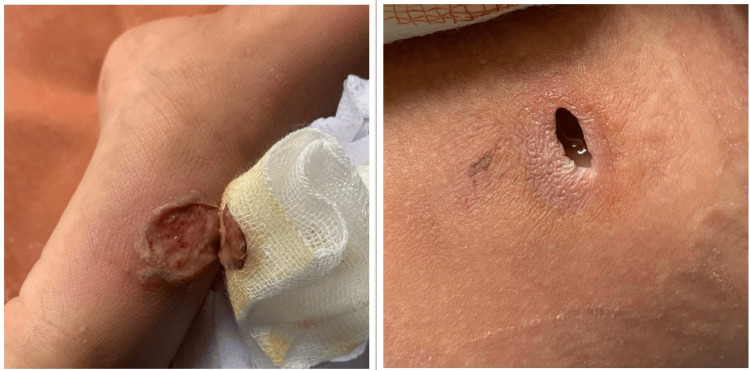 Figure 1
Figure 1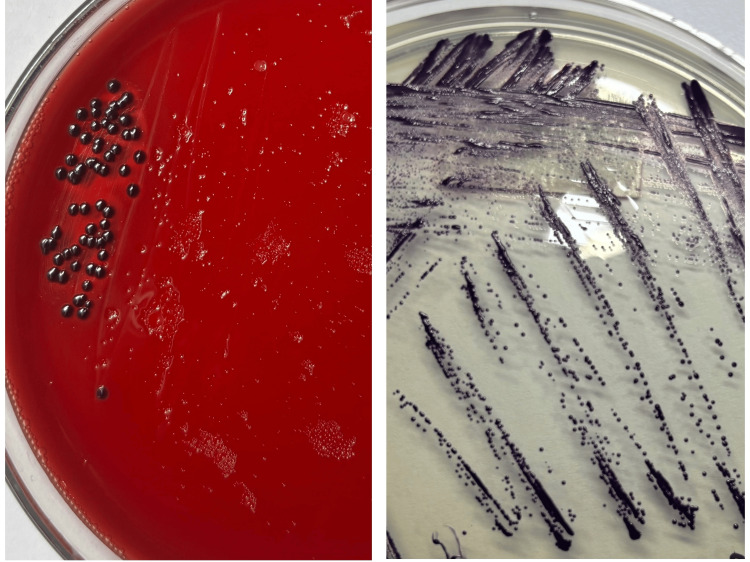 Figure 2
Figure 2| Parameters | Results | Reference value |
| Hemoglobin | 13.6 gm/dL | 12-16.5 gm/dL |
| TLC | 29600/mm³ | 4000-11000/mm³ |
| Differential leukocyte count | ||
| Neutrophils | 95% | 40%-80% |
| Lymphocytes | 2% | 20%-40% |
| Monocytes | 3% | 2%-8% |
| Total platelet count | 3.48 lakh/mm³ | (1.4-4.0) lakh/mm³ |
| Investigations | Results | Reference value |
| CRP | 193.31 mg/L | <5 mg/L |
| Dengue NS1 antigen and anti-dengue IgM antibodies qualitative assay | 0.01 | <1.0 (Index): Negative |
| >1.0 (Index): Positive | ||
| Dengue IgM antibody | 0.5 | <1.0 (Index): Negative |
| >1.0 (Index): Positive | ||
| Scrub typhus ( | Negative | |
| Typhi-screen test for | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMicrobial Metabolism and Applications
Introduction
Chromobacterium violaceum is a Gram-negative bacillus, a facultative anaerobe, and oxidase-positive, belonging to the family Neisseriaceae. It is a common inhabitant of soil and water, causing opportunistic infections in humans by gaining entry through disrupted skin barriers. Infections caused by C. violaceum are rare, with fewer than 200 cases reported. They can range from localized skin and soft tissue infections and organ abscesses to bloodstream infections that may lead to sepsis. This organism can affect both adults and children and is associated with a high mortality rate. Reporting of infections by C. violaceum should be carried out with caution, taking into account geographical location and the local epidemiological profile, with most cases occurring in tropical and subtropical regions [1,2]. Given that most infections occur following skin trauma, we present a case involving a pediatric patient with a skin and soft tissue infection. Due to its high fatality rate and limited number of documented cases, we aim to highlight the virulent nature of an uncommon pathogen, providing insights for both clinicians and microbiologists. Additionally, we aim to emphasize the importance of prompt microbiological culture and sensitivity testing to guide appropriate antibiotic therapy and prevent the development of antibiotic resistance.
Case presentation
A seven-year-old boy came to the Emergency Department with complaints of fever for three days. He had a small wound on his left foot prior to the onset of fever. The child had reportedly sustained the injury while playing outdoors. The wound was managed conservatively at home by the parents with Betadine ointment before presenting to the hospital. On examination, the wound on the left foot had minimal pus discharge. It had initially started as a small pustular lesion that gradually increased in size. There was also a small abscess formation on the left thigh (Figure 1). His blood reports on admission were within the normal reference range except for markedly raised total leukocyte count (TLC) and C-reactive protein (CRP). Other tropical causes of fever, like scrub typhus IgM, dengue NS1 and IgM antibody, and TyphiDot IgM, were all ruled out by negative rapid immunochromatographic test (ICT) (Tables 1, 2). No significant abnormality was observed on the ultrasound of the whole abdomen. The patient was admitted on account of acute febrile illnesses under evaluation, with suspected suppurative lymphadenopathy. He was empirically started on intravenous ceftriaxone 500 mg given every 12 hours. Mupirocin ointment was also applied locally to the wound. The patient was subsequently referred to the Department of Surgery for incision and drainage of the abscess. Pus swab from the foot and aspirated pus from the thigh were sent to the Microbiology Department for culture and sensitivity testing on day 3 (D3) of admission. Plating was performed on blood agar and MacConkey agar, which were incubated at 37°C overnight. Gram staining revealed the presence of a few pus cells, and the culture plates showed heavily pigmented violet-colored, smooth, round, concave colonies on both agar media. The colonies were further subcultured onto nutrient agar for better visualization of the pigment production (Figure 2). Based on the distinct dark violet-colored pigmentation, C. violaceum was suspected to be the isolated organism. As the patient continued to have high-grade fever, the treatment regimen was changed to intravenous piperacillin-tazobactam 1.8 g and clindamycin 270 mg, administered every eight hours. Identification of the organism was further confirmed using the automated VITEK® 2 Compact system (bioMérieux, Inc.) using the Gram-negative identification card. Antimicrobial susceptibility testing revealed the organism to be susceptible to amikacin (MIC 16 µg/mL), ciprofloxacin (MIC ≤0.06 µg/mL), and levofloxacin (MIC ≤0.12 µg/mL). The organism was resistant to piperacillin-tazobactam, ceftazidime, cefoperazone-sulbactam, cefepime, aztreonam, and carbapenems. Based on the antibiotic report, the antibiotic was switched to intravenous ciprofloxacin 500 mg every 12 hours on day 5 (D5). The blood culture sent on admission was sterile after 48 hours and five days of incubation.
Lesion on the left foot (left) and left thigh (right)
Violet-colored colonies of Chromobacterium violaceum on blood agar (left) and nutrient agar (right)
The patient began to show clinical improvement; however, a small lump was noted on the left thigh, just below the site of the previous lesion. Local examination revealed no signs of abscess formation, and the patient remained afebrile with no other systemic symptoms. He was on intravenous ciprofloxacin for 14 days and then discharged with instructions to continue oral ciprofloxacin for another 10 days. He was asked to follow up at the outpatient department (OPD) upon completion of the antibiotic course. At the follow-up post-discharge, the patient was clinically well and asymptomatic. The previously noted lump persisted but had regressed in size. He was advised to continue oral ciprofloxacin and was placed under close monitoring for any recurrence or complications. The patient attended regular follow-ups for nearly two months. The lesions had fully healed with the formation of granulation tissue, and the lump had completely resolved. The patient was advised to monitor for any signs or symptoms of recurrence.
Discussion
C. violaceum was initially described as a tropical pathogen with relatively few documented cases of human infection. It is characterized by its distinctive, dark violet pigmentation on culture media. Among the limited number of reported human infections worldwide, a total of 18 pediatric cases were reported between 2015 and 2024. In children, the presumed source of infection was typically soil or water, with the organism entering the body through traumatic breaches in skin or mucosal barriers. This is often followed by regional lymphadenopathy, as observed in our case [2]. In our patient, the suspected portal of entry was a lesion on the foot, which was subsequently followed by the development of an abscess on the ipsilateral thigh.
The first reported case of C. violaceum in India was seen in an 11-month-old neonate, followed by a second case in a two-year-old pediatric patient. Both succumbed to the infection, underscoring the organism’s potential for high fatality [3]. The isolate described in this study represents the first known reported case of C. violaceum in the northeastern state of India. Given its rarity, C. violaceum was initially considered an unlikely causative agent in our patient. However, its isolation from both the foot and thigh confirmed it as the causative pathogen.
Review of literature showed a wide range of reported mortality rates for C. violaceum infections, varying from approximately 18% to as high as 53% [2,4]. The diverse mortality rate may be attributed to several factors, including the presence of co-morbidities, age of the individual, severity of disease (localized versus disseminated), and timeliness and appropriateness of antimicrobial therapy. Once infection is established, C. violaceum can disseminate locally, resulting in multiple abscesses and progressing to sepsis. As evident in our case report, the inflammatory markers of CRP were markedly raised to 30-fold from their normal reference value, along with TLC. These results confirmed the diagnosis of bacterial infection, underscoring the virulence and severity of C. violaceum infection. Due to its reported high fatality, the timely initiation of effective antimicrobial treatment is critical to preventing disease progression. In the present case, the specimen for culture was not sent on the day of admission, resulting in a delay in identifying the causative organism and exposing the patient to unnecessary empirical antibiotics. Resistance to the initial empirical regimens, third-generation cephalosporin (ceftriaxone) and Piperacillin-tazobactam was observed in our isolated organism. This finding underscores the importance of strict culture-guided therapy to prevent the misuse and overuse of antibiotics. It highlights a broader concern where antibiotic resistance remains a significant global health threat, contributing to increased morbidity, prolonged hospital stays, and healthcare costs. This experience also emphasizes the need for closer coordination between clinicians and microbiologists, with greater vigilance in identifying infection sources. C. violaceum is particularly known to be resistant to several classes of antibiotics [5]. As there are no established antibiotic susceptibility breakpoints for C. violaceum in the current CLSI and EUCAST guidelines, antibiotic susceptibility testing was interpreted following the CLSI M100 35th edition for *Pseudomonas aeruginosa, *which is considered to provide clinically relevant interpretive criteria for *C. violaceum *[6]. When it comes to treatment, various literature have reported successful outcomes with ciprofloxacin, either as monotherapy or in combination with piperacillin-tazobactam or trimethoprim-sulfamethoxazole, guided by antibiotic susceptibility profile [4,5].
Based on the limited resources and high risk of relapse, a prolonged treatment duration of up to three months is generally recommended for C. violaceum. A prolonged antibiotic course typically involves an initial phase of parenteral therapy followed by oral maintenance therapy for a total duration of two to three months [7,8]. In contrast, treatment of shorter duration has also been documented, but it was more frequently associated with relapse. The recurrence of relapse is hypothesized to be due to persistence of microabscesses or septic foci that may not be fully eradicated by therapy. Nonetheless, few reports have noted successful infection control even with shorter treatment duration [9]. Our case lies concurrent with the latter, where a shorter duration of one-month therapy was met with successful resolution of the infection.
Conclusions
C. violaceum is associated with high fatality and morbidity rates due to its potential for rapid progression and dissemination. However, with increasing awareness of its pathogenicity and advancements in early detection methods, these rates are expected to decline substantially. Emphasizing the importance of timely culture and antibiotic susceptibility testing is critical for effective source control and the initiation of appropriate antimicrobial therapy. Furthermore, preventing relapse through continued antibiotic treatment and close patient follow-up remains a key component in the successful management of* C. violaceum* infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fatal infection by Chromobacterium violaceum Lancet Sneath PHA Whelan JPF Singh RB Edwards D 276277262195310.1016/s 0140-6736(53)91132-513085740 · doi ↗ · pubmed ↗
- 2Chromobacterium violaceum infections in children: two case reports and literature review Eur J Clin Microbiol Infect Dis Jiang Z Ren Y Ye S 247724834320243941791710.1007/s 10096-024-04949-x PMC 11608380 · doi ↗ · pubmed ↗
- 3Regulation of virulence in Chromobacterium violaceum and strategies to combat it Front Microbiol Venkatramanan M Nalini E 13035951520243832842310.3389/fmicb.2024.1303595 PMC 10847564 · doi ↗ · pubmed ↗
- 4Chromobacterium violaceum infection: a clinical review of an important but neglected infection J Chin Med Assoc Yang CH Li YH 4354417420112203613410.1016/j.jcma.2011.08.013 · doi ↗ · pubmed ↗
- 5Chromobacterium violaceum: a Review of an Unexpected Scourge Int J Gen Med Alisjahbana B Debora J Susandi E Darmawan G 325932701420213426754410.2147/IJGM.S 272193 PMC 8276824 · doi ↗ · pubmed ↗
- 6CLSI M 100: Performance Standards for Antimicrobial Susceptibility Testing CLSI supplement M 100Clinical and Laboratory Standards Institute Lewis IIJS Mathers AJ Bobenchik AM Pennsylvania, USA Clinical and Laboratory Standards Institute 2025 https://clsi.org/shop/standards/m 100/10.1128/jcm.01623-23PMC 1242184940772786 · doi ↗ · pubmed ↗
- 7Invasive Chromobacterium violaceum infection in children: case report and review Pediatr Infect Dis J Sirinavin S Techasaensiri C Benjaponpitak S Pornkul R Vorachit M 5595612420051593357110.1097/01.inf.0000164761.81491.3f · doi ↗ · pubmed ↗
- 8Chromobacterium violaceum sepsis: rethinking conventional therapy to improve outcome Am J Case Rep Richard KR Lovvorn JJ Oliver SE Ross SA Benner KW Kong MY 7407441620152647775010.12659/AJCR.894509 PMC 4614536 · doi ↗ · pubmed ↗