Efficacy of denosumab versus alendronate for aromatase inhibitor-associated osteoporosis in postmenopausal breast cancer patients: a retrospective analysis
Yi Zhang, Wenhe Cui, Lei Hou

TL;DR
Denosumab was more effective than alendronate in improving bone density and reducing fractures in postmenopausal breast cancer patients on aromatase inhibitors.
Contribution
This study provides a direct comparison of denosumab and alendronate for aromatase inhibitor-associated osteoporosis in breast cancer patients.
Findings
Denosumab showed greater improvement in bone mineral density compared to alendronate.
Denosumab was associated with a significantly lower incidence of vertebral compression fractures.
Both treatments improved bone metabolism markers, but denosumab had better clinical outcomes.
Abstract
Bisphosphonates and denosumab can increase bone mineral density (BMD) and are used to treat osteoporosis caused by aromatase inhibitors (AIs). However, few studies have been conducted on the effects of both on vertebral compression fractures (VCFs). This article aims to compare the effects of alendronate sodium and denosumab injection on the frequency of VCFs in postmenopausal women whose osteoporosis was brought on by AIs treatment for breast cancer. A retrospective cohort study was conducted from January 2020 to December 2024, enrolling 121eligible breast cancer patients with aromatase inhibitor-associated osteoporosis from the orthopedic outpatient department of Foshan Hospital of Traditional Chinese Medicine. Patients were divided into two treatment groups: the alendronate group received oral alendronate sodium tablets (70 mg once weekly), while the denosumab group received…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
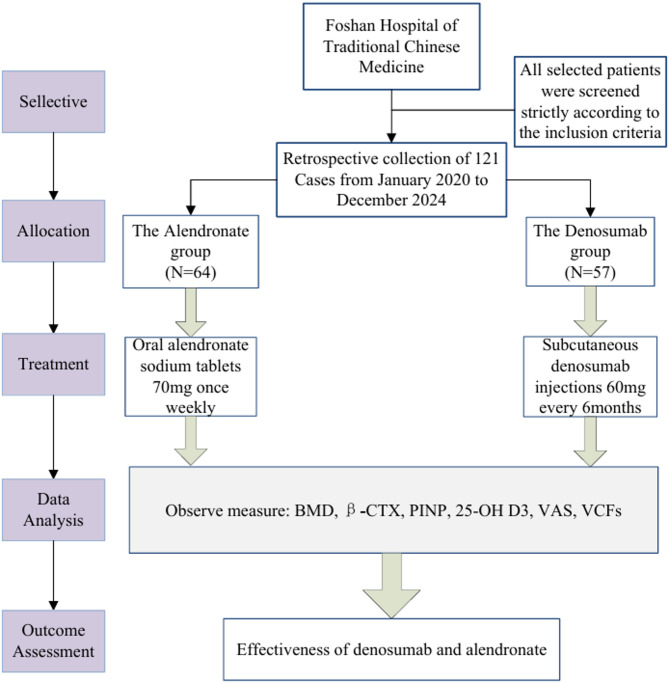 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone health and treatments · Bone Metabolism and Diseases · Bone health and osteoporosis research
Background
Breast cancer represents the most frequently diagnosed malignancy in women globally, with high morbidity and mortality rates in people over 50 years of age [1]. Approximately 75% of cases are hormone receptor-positive (HR+), characterized by expression of estrogen receptor (ER) and/or progesterone receptor (PR) [2]. Importantly, elevated hormone receptor expression has been significantly associated with an increased risk of distant metastasis [3]. Endocrine therapy constitutes the cornerstone treatment for hormone receptor-positive (HR+) breast cancer. Current clinical guidelines recommend selective estrogen receptor modulators (SERMs; e.g., tamoxifen) as first-line therapy for premenopausal patients, while third-generation AIs (e.g., exemestane, letrozole, anastrozole) represent the standard of care for postmenopausal women [4]. Although these regimens significantly reduce recurrence rates and cancer-specific mortality in HR + early breast cancer (EBC), prolonged administration is associated with clinically significant adverse effects [5, 6]. The skeletal effects of endocrine therapy are mediated through estrogen’s pivotal role in bone homeostasis. In premenopausal women, physiological estrogen levels maintain bone integrity through balanced regulation of osteoblast-mediated bone formation and osteoclast-mediated resorption. The postmenopausal state, characterized by ovarian failure and consequent estrogen deficiency, disrupts this equilibrium through multiple mechanisms: (1) impaired osteocyte function, (2) upregulated osteoclast activity, and (3) diminished bone mineralization capacity. These pathological changes collectively lead to accelerated bone loss, microarchitectural deterioration, and compromised biomechanical strength, culminating in osteoporosis and increased susceptibility to fragility fractures [7]. Other clinically significant risk factors, including metabolic comorbidities such as type 2 diabetes mellitus and obesity (BMI ≥ 30 kg/m²), must be carefully evaluated in conjunction with primary treatment considerations [8, 9].
Current clinical guidelines recommend both oral and intravenous bisphosphonates as effective therapeutic interventions for managing aromatase inhibitor-associated bone loss, with demonstrated clinical efficacy in preserving BMD. The pharmacological action of bisphosphonates is mediated through their high affinity for hydroxyapatite crystals in the bone mineral matrix. Following incorporation into the bone structure, these compounds are selectively taken up by osteoclasts during bone resorption, where they induce cellular apoptosis through inhibition of the mevalonate pathway, thereby effectively suppressing excessive bone turnover [10]. Bisphosphonates have emerged as first-line pharmacologic therapy for osteoporosis owing to their potent antiresorptive properties and demonstrated efficacy in increasing BMD [11].
Denosumab is a fully human monoclonal antibody (IgG2 subtype) that functions as a potent anti-resorptive agent through its high-affinity binding to receptor activator of nuclear factor kappa-B ligand (RANKL). The therapeutic mechanism involves: (1) neutralization of circulating RANKL, (2) blockade of RANKL-RANK interaction, and (3) subsequent modulation of the OPG-RANKL-RANK signaling pathway. This targeted action results in three principal clinical effects: (i) suppression of osteoclast differentiation and activation, (ii) enhancement of BMD through reduced bone resorption, and (iii) alleviation of bone pain. Clinically, denosumab is approved for two major indications: treatment of postmenopausal osteoporosis and prevention of skeletal-related events in patients with metastatic breast cancer to bone [12].
From a pharmacokinetic perspective, denosumab exhibits unique metabolic characteristics. As a monoclonal antibody, it undergoes catabolism via proteolytic degradation without hepatic metabolism. Importantly, renal impairment does not significantly alter its pharmacokinetic profile, as demonstrated in clinical pharmacokinetic studies. This distinctive property makes denosumab particularly suitable for patients with compromised renal function [13]. Clinical studies have consistently demonstrated the superior efficacy of denosumab in augmenting BMD compared to other antiresorptive agents, with significant improvements observed at key skeletal sites including the lumbar spine (LS), total hip (TH), and femoral neck (FN) [14]. Based on its demonstrated clinical efficacy, denosumab received regulatory approval for osteoporosis treatment in multiple jurisdictions [15].
Despite the widespread clinical use of both denosumab and bisphosphonates (e.g., alendronate) for osteoporosis management, there remains a paucity of rigorous comparative studies evaluating their relative efficacy in two key domains: (1) BMD improvement, and (2) fracture prevention. To address this critical knowledge gap, we designed this comparative effectiveness study to systematically evaluate these two antiresorptive therapies in breast cancer patients with aromatase inhibitor-induced osteoporosis. Our primary objectives are to compare their effects on: (i) BMD changes at lumbar spine, femoral neck, and total body, (ii) serum bone turnover markers (including β-CTX and P1NP) and 25-OH D3, (iii) incidence of VCFs over a 12-month treatment period.
Patients and methods
Study subjects
We conducted a retrospective cohort analysis of 121 breast cancer patients who developed aromatase inhibitor-induced osteoporosis and were treated at the Orthopedics Outpatient Clinic of Foshan Hospital of Traditional Chinese Medicine from January 2020 to December 2024. All participants received baseline therapy with oral calcitriol (0.25 µg/day) and calcium carbonate/vitamin D3 (600 mg/400 IU daily). Based on their osteoporosis treatment regimen, patients were stratified into two groups: The alendronate group (n = 64) received weekly oral alendronate (70 mg), and the denosumab group (n = 57) received subcutaneous denosumab (60 mg every 6 months). Diagnostic Criteria 1. Histologically confirmed diagnosis of invasive epithelial breast carcinoma. Postmenopausal status, as rigorously defined by the NCCN Clinical Practice Guidelines in Oncology: Breast Cancer (2018 version) [16]0.2. Hormone receptor (HR) status was determined according to the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) Guideline Recommendations for Immunohistochemical Testing of Estrogen and Progesterone Receptors in Breast Cancer (2010 version). HR positivity was defined as ≥ 1% nuclear staining for either estrogen receptor (ER) or progesterone receptor (PR) in invasive tumor cells, as assessed by validated immunohistochemical methods [17]. 3. BMD was evaluated according to World Health Organization (WHO) diagnostic criteria for osteoporosis in postmenopausal women. Measurements were obtained at two anatomical sites: (1) lumbar spine (L1-L4) via anteroposterior dual-energy X-ray absorptiometry (DXA), (2) total hip (including femoral neck), and (3) total body. Results were interpreted using T-scores, with the following WHO classification thresholds: normal (T-score ≥ −1.0), osteopenia (−2.5 < T-score < −1.0), and osteoporosis (T-score ≤ −2.5) [18]. The study design flow is illustrated in Fig. 1. Inclusion Criteria: Eligible patients met al.l of the following criteria: (1) Histologically confirmed invasive breast cancer with hormone receptor positivity. (2) Pathological stage I-IIIA disease according to the AJCC 8th edition staging system. (3) Age ≤ 75 years with preserved hepatic and renal function. (4) Completion of primary treatment, including definitive breast surgery, adjuvant chemotherapy (if indicated), and radiotherapy (if indicated). (5) Current treatment with adjuvant endocrine therapy. (6) Postmenopausal status, defined as either natural menopause or induced menopause. (7) Minimum antiresorptive therapy exposure ≥ 12 months of weekly oral alendronate (70 mg), or ≥ 2 doses of subcutaneous denosumab (60 mg every 6 months). (8) Complete availability of baseline and follow-up clinicopathological data, Serial BMD measurements, and signed informed consent documents. Exclusion Criteria: Patients were excluded if they met any of the following conditions: (1) Presence of metastatic breast cancer. (2) Chronic glucocorticoid use (>3 months cumulative use within the past year). (3) Significant hepatic dysfunction or renal impairment. (4) Concurrent metabolic bone diseases (including but not limited to: Primary hyperparathyroidism, Paget’s disease of bone, and Osteogenesis imperfecta. (5) Severe comorbidities include psychiatric conditions that may compromise pain assessment reliability.Fig. 1. Flow of study design
Methods
Both treatment groups maintained their prescribed endocrine therapy regimens throughout the study period, with all participants receiving standardized baseline supplementation (calcitriol 0.25 µg/day plus calcium carbonate 600 mg/day). The alendronate group (n = 64) was administered oral alendronate sodium (Fosamax^®^; Hangzhou MSD Pharmaceutical Co., Ltd.; NMPA approval no. J20140144) 70 mg once weekly. The denosumab group (n = 57) received subcutaneous denosumab (Prolia^®^; 60 mg) every 6 months. The comparative treatment period was 12 months, and we evaluated pre- and post-treatment indicators: BMD, β-CTX, P1NP, 25-(OH) D3, radiographically confirmed VCF incidence, and VAS pain scores.
Efficacy evaluation criteria
Therapeutic Efficacy Assessment Criteria for Osteoporosis: Markedly Effective Response: Complete resolution or near-complete resolution (≥ 80% reduction) of baseline pain symptoms, significant improvement in BMD by dual-energy X-ray absorptiometry (DXA). Effective response: Clinically meaningful pain reduction, Maintenance of baseline BMD (± 1% change) or modest improvement, No sleep disturbance attributable to persistent pain. Ineffective response: failure to achieve ≥ 50% pain reduction, no significant BMD improvement, and no measurable improvement in quality of life parameters [10].
Statistical methods
All statistical analyses were performed using SPSS version 27.0, with a two-tailed significance threshold set at α = 0.05. Normally distributed count data were expressed as frequencies and analyzed using the chi-square test. Measurement data were assessed for normality (Shapiro-Wilk test) and homogeneity of variance (F-test). Normally distributed measurement data were presented as mean ± standard deviation (x̄ ± s). Intergroup comparisons of normally distributed measurement data were performed using the independent t-test (Student’s t-test for equal variances; Welch’s t-test for unequal variances). Intragroup comparisons before and after treatment were conducted using the paired t-test. Non-normally distributed continuous variables were expressed as medians and interquartile ranges [M (P25, P75)]. Intergroup comparisons were performed using the Mann–Whitney U test, and intragroup comparisons were conducted using the Wilcoxon signed-rank test.
P < 0.05 was considered statistically significant.
Results
Baseline characteristics
Baseline demographic and clinical characteristics, including age, body mass index (BMI), menopausal duration, and duration of AIs therapy, were well-balanced between the two treatment groups (all P > 0.05), demonstrating comparable baseline profiles (Table 1).Table 1. Comparison of general data between the two groups (x ± s)GropeYearBMI/(g/cm2)Menopause period(year)Taking Ais time(month)Alendronate(n = 64)59.58 ± 6.0122.49± 2.719.02 ± 4.3722.81 ± 10.04Denosumab(n = 57)61.16 ± 5.0722.62 ± 3.448.88 ± 3.8324.07 ± 9.86t1.5520.2320.1840.694P0.1230.8170.8530.489
Comparison of BMD before and after treatment
Lumbar spine BMD T-Score comparison
Initial assessment revealed no statistically significant intergroup difference in lumbar spine BMD T-score (P = 0.076), confirming appropriate baseline matching between cohorts. Following the intervention period, an independent samples t-test demonstrated significantly greater improvement in lumbar spine BMD T-score in the denosumab group compared to the alendronate group (P = 0.003). Paired t-tests indicated significant within-group improvements from baseline in both treatment arms(P<0.001) (Table 2).Table 2. Changes in bone mineral density T-values, bone metabolic indexes and 25(OH)D3 before and after treatment in the two groupsGrouplumbar Spine BMD T-score(x ± s, g/cm2)femoral neck BMD T-score(x ± s, g/cm2)total body BMD T-score (x ± s, g/cm2)β-CTX [M (P25, P75) ng/mL]PINP [M (P25, P75) ng/mL]25-OH D3[M (P25, P75) ng/mL]Alendronate(n = 64)before treatment−2.96 ± 0.77−2.68 ± 0.68−2.77 ± 0.8460.92(0.32, 0.78)62.50(36.44, ,56.08)59.22(16.09, 26.347)after treatment−2.72 ± 0.78−2.55 ± 0.72−2.63 ± 0.8064.31(0.30, 0.68)66.13(47.43, 66.27)59.27(19.77, 38.83)t/Z/U7.2324.8885.785−3.301−5.026−6.52P-value<0.001<0.001<0.001<0.001<0.001<0.001Denosumab(n = 57)before treatment−3.47 ± 0.99−3.15 ± 0.95−3.20± 1.0861.09(0.38, 0.76)59.24(33.77, 56.79)63.00(16.67, 27.41)after treatment−3.19± 0.94−3.01± 0.92−3.05 ± 1.0457.28(0.27, 0.64)55.25(42.45, 62.41)62.95(20.83, 33.98)t/Z/U7.5754.0587.981−4.308−4.517−5.097P-value<0.001<0.001<0.001<0.001<0.001<0.001t1/Z1/U12.9021.1091.456181917231710P1-value0.0760.0770.1160.9790.5540.554t2/Z2/U23.0273.0882.468161214961713P2-value0.0030.030.0260.2710.0890.564t1/Z1/U1, P1-value means Comparison of the two groups before treatment; t2/Z2/U2, P2-value means Comparison of the two groups after treatment
Femoral neck BMD T-Score comparison
Initial measurements showed comparable femoral neck BMD T-score between groups (P = 0.077), confirming balanced baseline characteristics. After 12 months of treatment, the denosumab group demonstrated significantly greater improvement in femoral neck BMD T-score compared to the alendronate group (P = 0.005). The BMD T-score of the femoral neck changed significantly in both groups after treatment(P<0.001) (Table 2).
Total body BMD T-Score comparison
Initial total body BMD T-score measurements showed no significant intergroup differences (P = 0.116), confirming comparable baseline characteristics between treatment arms. Following the intervention period, independent samples t-test analysis revealed statistically superior total body BMD T-score improvements in the denosumab group versus the alendronate group (P = 0.026). Paired t-tests demonstrated significant improvements from baseline in both groups (P<0.001) (Table 2).
Comparison of 25-OH D3 levels before and after treatment
No significant difference was observed in baseline serum 25-OH D3 levels between the denosumab groups (P = 0.554), confirming comparable baseline vitamin D status. The Mann-Whitney U test showed no statistically significant difference in post-treatment 25-OH D3 levels between groups (P = 0.564). Wilcoxon signed-rank tests revealed significant increases from baseline in both treatment arms(P<0.001) (Table 2).
Comparison of PINP levels before and after treatment
Initial serum PINP levels were comparable between groups (P = 0.554), indicating balanced baseline bone formation status. The Mann-Whitney U test revealed no significant difference in post-treatment PINP levels between groups (P = 0.089). Wilcoxon signed-rank tests demonstrated significant reductions from baseline in both treatment arms (P<0.001) (Table 2).
Comparison of β-CTX levels before and after treatment
No significant difference was observed in baseline serum β-CTX levels between the treatment groups (P = 0.979), indicating comparable baseline bone resorption activity. The Mann-Whitney U test demonstrated no statistically significant difference in post-treatment β-CTX levels between groups (P = 0.271). Wilcoxon signed-rank tests revealed significant reductions in β-CTX levels from baseline in both groups (P<0.001) (Table 2).
Comparison of VAS scores before and after treatment
Initial VAS pain scores demonstrated no significant difference between groups (P = 0.665), confirming comparable baseline pain levels. Independent samples t-test revealed no statistically significant difference in post-treatment VAS scores between groups (P = 0.892). Paired t-tests demonstrated significant pain reduction in both treatment arms (P<0.001) (Table 3).Table 3. Comparison of VAS scores between the two groups before and after treatment(x ± s)GroupBefore treatmentAfter 6 months of treatmentAfter 12 months of treatmenttPAlendronate(n = 64) 6.22± 0.15 5.36± 0.143.56 ± 0.1219.914<0.001Denosumab(n = 57)6.33± 0.215.33± 0.163.59 ± 0.1318.682<0.001t0.4340.1150.136P0.6650.9060.892
Comparison of vertebral fracture incidence before and after treatment
In the alendronate group, post-treatment thoracic compression fractures occurred in 3 cases and lumbar compression fractures in 6 cases (total fracture rate: 12.5%). The denosumab group reported 1 thoracic and 3 lumbar compression fractures (total fracture rate: 7.017%). Fisher’s exact test demonstrated a significantly lower fracture incidence in the denosumab group (P < 0.05) (Table 4).Table 4. The incidence of vertebral fractures before and after treatment in the two groups (cases %)GroupCasethoracic fracturelumbar fracturetotal rateAlendronate643(4.69)6(9.38)9(14.06)Denosumab571(1.75)3(5.26)4(7.02)X^2^12.00P0.002
Efficacy evaluation before and after treatment
The denosumab group exhibited a higher treatment efficacy rate (91.22%) compared to the alendronate group (82.81%). Fisher’s exact test confirmed the superiority of the denosumab group (P < 0.05) (Table 5).Table 5. Clinical efficacy evaluation of the two groups of patients after treatment (cases/%)GroupCaseSignificant effectEffectiveIneffectiveeffective rate(%)Alendronate6436171153(82.81)Denosumab573715552(91.22)X^2^4.571P0.03
Discussion
Endocrine therapy, utilizing estrogen receptor antagonists and AIs, has become a cornerstone of postoperative breast cancer management by reducing estrogen levels and modifying the tumor microenvironment to inhibit neoplastic growth [19]. Clinical evidence from multiple randomized controlled trials has established that completing a standard 5-year course of adjuvant endocrine therapy in hormone receptor-positive early breast cancer (HR [+] EBC) patients is associated with significant Survival Benefit and durable Protection [20]. Furthermore, multiple clinical trials have confirmed that extending endocrine therapy to up to 10 years further decreases the recurrence and mortality rates of HR [+] EBC. The third-generation AIs have been established as the first-line endocrine therapy for postmenopausal women with hormone receptor-positive (HR+) breast cancer [21].
Despite their oncologic efficacy, endocrine therapies adversely impact bone health through estrogen suppression, leading to accelerated bone loss and significantly elevated fracture risk in breast cancer patients [5, 22]. AIs therapy in HR[+] breast cancer patients is associated with 17–22% 5-year fracture risk, mediated through hypoestrogenism-induced bone turnover imbalance (40–60% CTX elevation) and preferential trabecular bone loss (5–8% annual lumbar spine BMD decline) [23]. A meta-analysis revealed a positive correlation between prolonged AI treatment duration and increased fracture incidence [24]. Goss et al. (MA.17R trial) reported that high-risk patients on extended AI therapy (10 years) face progressive annual fracture risk increases (2–4%) [25]. HR-pQCT analysis by Kuba et al. demonstrated significant 12-month AI-induced deterioration in postmenopausal breast cancer patients, including trabecular BMD loss, cortical thinning, and reduced bone strength [26]. Moreover, all AIs carry significantly higher risks of osteoporosis and fractures versus tamoxifen, with consistent effects across anastrozole, letrozole, and exemestane [5, 27].
Current guidelines recommend combining lifestyle modifications (calcium/vitamin D, exercise) with anti-resorptives (bisphosphonates/denosumab) for bone protection in AIs treated patients [28]. Bisphosphonates and denosumab are essential for maintaining bone health in this population. A recent study reported that early postmenopausal women with ER[+] breast cancer receiving AI therapy combined with anti-resorptive treatment exhibited significant increases in femoral and lumbar spine BMD (6.28% and 7.79%, respectively) after 24 months [29]. Anti-resorptive therapy markedly improves BMD in postmenopausal women with early breast cancer treated with AIs, thereby mitigating bone loss.
Bisphosphonates play a crucial role in regulating bone metabolism. They are effective in increasing BMD, reducing the risk of fractures, and they generally have favorable safety profiles [30]. By reducing levels of neuropeptides such as substance P (SP) and calcitonin gene-related peptide (CGRP), as well as inflammatory cytokines like tumor necrosis factor-alpha (TNF-α), bisphosphonates effectively alleviate pain in patients with osteoporosis and improve their overall quality of life. However, clinical caution is necessary, as bisphosphonates are contraindicated for patients with renal impairment (specifically, those with a creatinine clearance of less than 35 mL/min). Additionally, renal function should be closely monitored in elderly patients [31].
Recent years have seen a rise in the clinical application of denosumab. A literature review found that, compared to oral bisphosphonates, denosumab enhances patient preference and adherence, while providing a cost-effective therapeutic strategy, especially for elderly patients and those at high risk for osteoporosis [32]. Meta-analyses show that denosumab leads to greater gains in BMD compared to bisphosphonates after 12 months [33]. Denosumab shows promise in preventing BRCA1-mutated breast cancer by inhibiting bone metastasis and providing additional anticancer effects, significantly improving patient prognosis [34].
Denosumab has been recognized as an effective and safe treatment for preventing major osteoporotic fractures, especially vertebral and femoral fractures [35, 36]. In the prospective ABCSG-18 trial, denosumab (administered at a dose of 60 mg biannually) was found to reduce the risk of clinical fractures in postmenopausal breast cancer patients who were receiving AIs, compared to those in the vehicle group. Importantly, this treatment did not result in any additional adverse effects. Furthermore, denosumab doubled the time to the first fracture and significantly increased BMD at the lumbar spine, total hip, and femoral neck [37]. A network meta-analysis showed that after 12 months of treatment, denosumab decreased the risk of vertebral fractures by up to 85% compared to the vehicle. Multiple studies confirm that denosumab is the most effective therapy for preventing vertebral fractures [38–40].
Bone remodeling status can be evaluated using metabolic markers. PINP and β-CTX serve as specific markers for bone formation and resorption, respectively [41]. PINP is a biomarker that shows high sensitivity and specificity. It is less affected by hormonal changes and provides insight into osteoblast-mediated collagen synthesis, making it valuable for diagnosing metabolic bone diseases and renal insufficiency. On the other hand, β-CTX is the most commonly used marker for collagen degradation. It is an isomer of α-CTX and is closely related to the intensity of bone resorption. β-CTX responds quickly and sensitively to anti-resorptive therapies and can help predict the severity of abnormal bone turnover. 25-OH D is the main circulating form of vitamin D and accurately reflects the body’s vitamin D status. The liver hydroxylates vitamin D to produce 25-OH D, which is then activated to 1,25-OH D in the kidneys.
This study compared the effectiveness of alendronate and denosumab in treating aromatase inhibitor-induced osteoporosis in postmenopausal breast cancer patients. After one year of treatment, both groups showed increases in BMD at the lumbar spine, femoral neck, and total body, confirming that both medications are effective. Biochemical analyses indicated elevated levels of 25-OH D3 and P1NP, along with reduced β-CTX levels in both groups. Among the 64 patients receiving alendronate, three experienced thoracic VCFs, and five had lumbar VCFs. In the denosumab group, consisting of 57 patients, there was one thoracic VCF and three lumbar VCFs, suggesting a lower incidence of fractures with denosumab. Both treatments improved bone metabolic parameters by suppressing bone turnover and enhancing BMD.
To summarize, the relationship between breast cancer and bone health requires strategies to reduce skeletal complications during treatment. As researchers work to understand the mechanisms behind both acquired and inherent resistance to endocrine therapies and CDK4/6 inhibitors, it is essential to develop new endocrine agents that offer higher efficacy with fewer side effects [42]. Future research could improve tools for assessing fracture risk and lead to the development of more effective therapies.
This study has several limitations: (1) The timing of anti-osteoporotic drug initiation post-AI therapy may influence outcomes; (2) As a single-center retrospective study, the collection of patient data was non-randomized and potentially incomplete; (3) The small sample size may introduce selection bias, limiting the generalizability of findings; (4) The short follow-up period (one year) is insufficient to evaluate long-term efficacy and safety; (5) Rare adverse events (e.g., osteonecrosis of the jaw) were not fully monitored. Future research should increase sample sizes, extend follow-up durations, and evaluate long-term adverse effects to thoroughly assess the clinical effectiveness of denosumab and alendronate.
Conclusion
Both alendronate and denosumab are effective in treating AI-induced osteoporosis in breast cancer patients by improving BMD and modulating bone metabolism. Denosumab offers a reduced risk of VCFs.
Authors’ contributions
YZ contributed to the design of this article, conducted the statistical analyses, and drafted the manuscript. WHC assisted with the statistical analyses. LH provided critical revisions for the manuscript. All authors reviewed and approved the final manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Davies C, Pan H, Godwin J et al. Long-term effects of continuing adjuvant Tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial [published correction appears in lancet. 2013;381(9869):804.10.1016/S 0140-6736(12)61963-1PMC 359606023219286 · doi ↗ · pubmed ↗