Systematic review of indirect costs to families of children with developmental epileptic encephalopathies
Sunny Abdelmageed, Rebecca Y. Du, Maura Carroll, Anup Patel, Sandi Lam

TL;DR
This study reviews the indirect costs and burdens faced by families of children with developmental epileptic encephalopathies, highlighting significant impacts on caregivers' lives and well-being.
Contribution
The paper provides a systematic review of indirect costs and psychosocial impacts in families of children with developmental epileptic encephalopathies.
Findings
Caregiver burden disproportionately affects mothers, leading to career changes and reduced work productivity.
Caregiving is linked to decreased quality of life, depression, anxiety, and social isolation.
Siblings also experience opportunity costs and psychosocial challenges due to caregiving demands.
Abstract
Severe childhood epileptic encephalopathies have high burden on families and large indirect healthcare costs. Several studies have examined indirect costs primarily in Tuberous Sclerosis and Dravet syndrome, finding impacts in all major aspects of life. Indirect costs of these diseases are reported to be higher than other severe pediatric illnesses. To better understand the epilepsy care journey and possible barriers to optimal medical and surgical care, we sought to understand indirect costs of care and burden of illness for families. A systematic search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines using three databases (MEDLINE, Embase, and Scopus). Records were screened independently by two reviewers included based on pre-defined inclusion criteria. Studies were discussed narratively to identify common…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
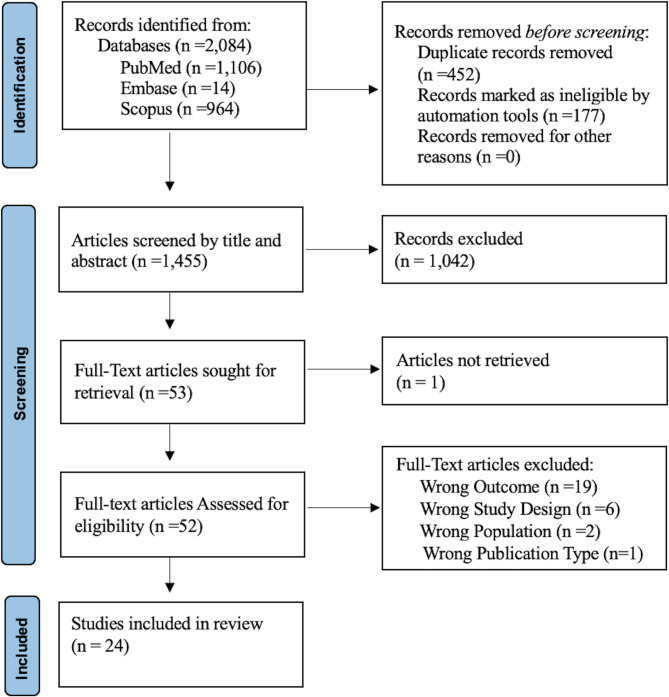 Figure 1
Figure 1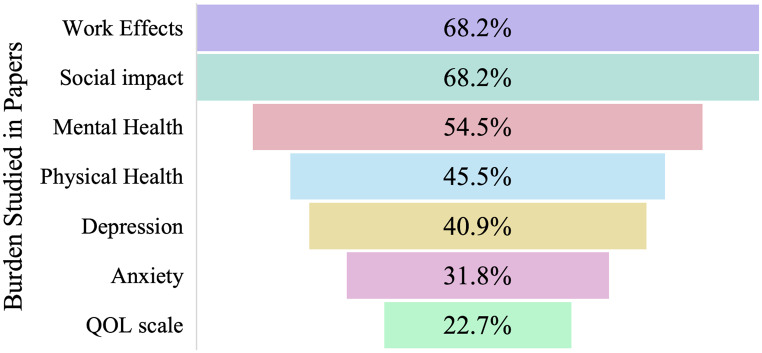 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberous Sclerosis Complex Research · Epilepsy research and treatment · Glycogen Storage Diseases and Myoclonus
Background
Families incur various indirect costs related to the burden of caring for a sick loved one in addition to direct medical expenses [1–3]. Indirect costs to caregivers are often reported by decreased work productivity, work loss, and worker replacement. Psychological, social, and physical impacts have also been described in caregivers [1, 4, 5]. For pediatric epilepsy, indirect costs to caretakers are enormous [6–9]. Pediatric epilepsy is the most common chronic neurological disorder in children, and the indirect costs are estimated to contribute up to 85% of total annual costs for the care of children with epilepsy [8]. With total costs estimated at up to $11,432 in high-income countries in 2022 [10]. Over half of caregivers of children with epilepsy have psychopathological symptoms, including high levels of stress leading to post-traumatic stress disorder, depression, anxiety, and sleep disturbances [5, 11–13].
The term developmental and epileptic encephalopathies (DEE) was developed in 2017 to describe conditions in which both developmental impairment and epileptic activity contribute negatively to the cognition and behavior of the patient [14]. Lennox-Gastaut Syndrome (LGS), Dravet Syndrome (DS) and Tuberous Sclerosis Complex (TSC) are severe forms of childhood onset DEE. Seizures often begin in the first few years of life, and almost all of these children will have developmental and intellectual delay, leading to decreased health-related quality of life (QOL) and major caregiver burden [15–17].
Understanding and quantifying indirect costs are essential for decision-making, healthcare resource allocation, and in defining the support required by families to improve health outcomes [2, 18]. Several studies have examined the indirect healthcare costs associated with DEE, primarily focusing on populations with DS and TSC [19–21] identifying costs in all aspects of life [22–24]. These studies use a variety of methods to explore various indirect costs and often focus on one or two domains such as physical health or psychosocial effects. While these findings are helpful, the burden of these conditions is multifaceted, and comparing caregiver burdens across different DEEs could provide additional insights.
We conducted a systematic review of the current literature on indirect costs of DEE, specifically, LGS, DS, and TSC, to delineate the secondary consequences of caregiver responsibilities and unquantified burdens.
Methods
A systematic review was performed according to the Preferred Reviews and Meta-Analyses (PRISMA) 2020 guidelines to explore the indirect costs of childhood epilepsy syndromes [25]. PubMed MEDLINE (National Library of Medicine), Embase (Elsevier), and Scopus (Elsevier) were searched on May 10, 2023 using keywords associated with three childhood epilepsy syndromes (Lennox-Gastaut Syndrome, Dravet Syndrome, Tuberous Sclerosis), pediatric populations, and indirect healthcare costs. A supplemental table shows this in more detail (see Supplemental File 1 for a full list of search terms). Articles were restricted to English language. No article type restrictions were applied. All studies meeting inclusion criteria were included from inception of the databases to May 10, 2023.This protocol was not prospectively registered because screening and data extraction were initially completed for a grant submission.
After the initial search, duplicates were excluded, and the remaining articles were screened for relevance by title and abstract based on the following prespecified inclusion criteria: 1) published in or translated into the English language, 2) available full text, 3) population of patients with LGS, DS, TSC or another severe childhood-onset epilepsy syndromes, and 4) providing outcomes of indirect healthcare costs. Articles progressing to full-text review were screened for final inclusion based using the full prespecified inclusion criteria seen in supplemental Table 2. Indirect health care costs included indirect economic cost (e.g., productivity loss), psychosocial impacts, physical impact, and impact on siblings. Multi-pass deduplication was performed using EndNote (Clarivate Analytics, Philadelphia, PA) and eligible articles were screened using Rayyan (https://rayyan.qcri.org/). This systematic review was conducted independently by two reviewers and disagreements were resolved based upon discussion.
Data were extracted independently by authors and cross-checked for accuracy. Included articles were reviewed for bibliographic data, design, participants, and outcomes. For each study, the population, country of origin, study design, and indirect costs were recorded. In addition, qualitative themes identified through qualitative studies were recorded.
Critical appraisal of included studies included risk of bias assessment using the Risk of Bias in Non-randomized Studies-of Interventions (ROBINS-I) tool conducted by adapting study design grades from Shadish et al. [26, 27]. Two reviewers (SA and RD) independently assessed each study. A third reviewer resolved disagreements through consensus.
Results
From the three databases, 2,084 records were identified. Following de-duplication 452 duplicates were removed and 177 were marked as ineligible by automation tools, due to non-English language or animal studies, these were cross-checked for accuracy by author SA. A total of 1,455 abstracts were screened and 52 were included for full text review. After screening using pre-determined inclusion/exclusion criteria, 24 full text articles were included in this review (see Fig. 1 for PRISMA full text selection flowchart). The overall quality of evidence was grade D (All studies were either cross-sectional studies or semi-structured interview) as per grading recommendations described in Shadish et al. The overall risk of bias was high.Fig. 1PRISMA flowsheet of included full-text articles
Study characteristics are shown in Tables 1 and 2. Indirect costs for DS caregivers were reviewed in 54.2 of manuscripts (n = 16), 33.3% for TSC (n = 8), 16.7% for LGS (n = 4), and 12.5% included other unspecified childhood onset epilepsies in addition to LGS, Dravet, or TSC (n = 3). Numbers do not add up to 24 as some papers combined diagnoses in the study population. Qualitative methods were used in 29.2% (n = 7) of studies, 66.68 (n = 16) used quantitative methods, and 4.1% (n = 1) used both. Qualitative methods consisted of semi-structured interviews or focus groups. All quantitative studies were cross-sectional designs. Results were sorted into themes based on primary outcomes. The psychosocial theme comprised 79.2% of manuscripts (n = 19), 62.5% in “economic” (n = 15), 41.7% in “physical” (n = 10), and 12.5% 3 in “siblings” (n = 3). Themes were further broken down into work effects (68.2%), social impact (68.2%), mental health effects (54.5%), physical effects (45.5%), and quantitative QOL impacts (22.7%, Fig. 2). Within mental health, 40.9% of papers described depression and 31.8% described anxiety. Studies that did include demographic and socioeconomic data showed subjects were primarily female (56–93%), highly educated (college degree or higher 66–79%), and White/Caucasian (84–91%). Fathers were more likely to be employed than mothers 82–91% compared with 46–70%.Table 1. Summary of included articlesAuthor, YearPopulationCountryMethodsThemesBailey, 2020 [28]LGS, Dravet, TSC, otherUnited StatesQuantitativeCross-sectional multicenter surveySiblingCampbell, 2018 [29]DravetUnited StatesQuantitativeCross-sectional survey single-center surveyEconomicPsychosocialDomaradzki, 2023 [30]DravetPolandQuantitative, qualitativeCross-sectional multicenter surveyEconomic PsychosocialGallop, 2010 [19]LGSUnited KingdomQualitativeSemi-structured interviewsEconomic psychosocial physicalGibson, 2014 [31]LGSUnited StatesQualitativeCross-sectional open and close-ended surveyPsychosocialGraffigna, 2013 [32]TSCItalyQualitativeSemi-structured interviewsPsychosocialphysicalGrau, 2021 [20]TSCGermanyQuantitativeCross-sectional multicenter surveyEconomicHesdorffer, 2020 [33]OtherUnited StatesQuantitativeCross-sectional design using REN dataPsychosocialphysicalJansen, 2020 [34]TSC31 countriesQuantitativeCross-sectional multicenter surveyPsychosocialJensen, 2017 [35]LGS, OtherUnited StatesQualitativeFocus groupsPsychosocialphysicalKopp, 2008 [24]TSCUnited StatesQuantitativeCross-sectional single-center surveyPsychosocialLagae, 2019 [36]DravetUK, France, Germany, Spain, ItalyQuantitativeCross-sectional multicenter surveyEconomicSiblingMaltseva, 2023 [37]DravetGermanyQuantitativeCross-sectional survey, prospective diaryEconomic psychosocial physicalNabbout, 2018 [38]DravetFranceQualitativeSemi-structured interviewsEconomic psychosocial physicalNabbout, 2019 [39]DravetUnited States, United Kingdom, ItalyQualitativeSemi-structured interviewsEconomic psychosocial physicalNabbout, 2020 [40]DravetFranceQuantitativeCross-sectional multicenter surveyEconomic psychosocial physicalGil-Nagel, 2023 [41]DravetSpainQuantitativeCross-sectional multicenter surveyEconomic, psychosocial physicalNolan, 2006 [42]DravetCanadaQualitativeSemi-structured interviewsPsychosocial siblingRentz, 2015 [43]TSCUnited StatesQuantitativeCross-sectional surveyPsychosocial physicalSkalicky, 2018 [44]TSCUnited StatesQuantitativeCross-sectional surveyEconomicStrzelczyk, 2019a [45]DravetGermanyQuantitativeCross-sectional, multi-center survey, prospective work productivity diaryEconomic, psychosocialStzrelczyk, 2019b [46]DravetGermanyQuantitativeCross-sectional, multicenter survey,Economic psychosocialWhittington, 2017 [47]DravetUnited StatesQuantitativeCross-sectional surveyEconomicWillems, 2021 [21]TSCGermanyQuantitativeCross-sectional multicenter surveyEconomic PsychosocialLGS, Lennox-Gastaut Syndrome; TSC, tuberous sclerosis complexTable 2Study characteristicsAim of studyMean Age or RangeDemographics of CaregiversNumber of CaregiversOutcomesInstruments UsedBailey, 2020 [28]Impact on siblings of DEEPatients: 16Siblings: 21Caregivers: NRNR128Siblings: 120QOLPsychosocial impactBurdenSibling Voices SurveyCampbell, 2018 [29]Impact on caregivers of DSPatients: 11.7Caregivers:NRNR30Caregiver burdenQOLEconomic burdenOCBSEQ-5D-5 LGeneral Health AssessmentWPAINHISDomaradzki, 2023 [30]Emotional experience of DS caregiversCaregivers: 39.790.7% female22.7% employed full-time75Emotional experience and burden of caregivingQOLStandardized questionnaireGallop, 2010 [19]QOL for caregivers and LGS childrenPatients: 12Caregivers: 3990% female40QOLPsychosocial impactHealth statusSF-36HADSGibson, 2014 [31]Impact of LGSPatients: 3.5–36Caregivers: NRNR96Psychosocial impactFinancial impactImpact on familySurveyGraffigna, 2013 [32]Parent experience with TSCPatients: 12Caregivers: 4764.6% female100% Italian48Caregiver experienceQualitative interviewGrau, 2021 [20]Direct and indirect costs of TSCPatients: 9.8Mothers: 40,8Fathers: 43.4Mothers: 70% employedFathers: 91% employed184Disease severityHealthcare utilizationDirect and indirect costsQuestionnaireHesdorffer, 2020 [33]Caregiver sleep in DEECaregivers: 4091.9% female91% NHW60.2% employed (full- or part-time)742Disease severityFatigueSleep disturbanceQOLREN surveyPROMISJansen, 2020 [34]Burden of illness and QOL in TSCPatients: 19.8Caregivers: NR61.5% female143Burden of illnessHealthcare utilizationQOLEQ-5DQOLCEJensen, 2017 [35]Life impact for DEE caregiversPatients: 8.4Caregivers: 4284% female84% NHW26% employed full-time19Physical healthMental healthSocial functionFinancial resourcesPROMISKopp, 2008 [24]Behavior Problems in TSCPatients: 7.7Caregivers:NR75.6% female66.7% employed45Patients: 99Psychological impactParental stressParenting Stress IndexSCL-90-RLagae, 2019 [36]Caregiver impact and healthcare utilization in DSCaregivers: NRNR584QOLSupportOut-of-pocket expensesTreatmentOnline SurveyEQ-5D-5 LMaltseva, 2023 [37]Sleep and caregiver burden in DS caregiversPatients: 13.5Caregivers: 44.7Primary caregivers: 92.6% femaleMothers: 46.3% employedFathers: 85.2% employed108Psychosocial impactPhysical healthCaregiver burdenProfessional impactHADSPSQIBSFCQuestionnaireProspective diaryNabbout, 2018 [38]Caregiver related outcomes in DSCaregivers: 40.757.1% female11Psychosocial impactPhysicalCaregiver burdenQOLQualitative interviewNabbout, 2019 [39]Impact of DS in familiesCaregivers: 43.365% female20Caregiver burdenPhysical healthPsychosocial impactFamily impactQualitative interviewsNabbout, 2020 [40]Impact of DS on caregiversPatients: 7.6Caregivers: NR79.3% college education or greater87Caregiver burdenPsychosocial impactProfessional impactSurveyGil-Nagel, 2023 [41]Impact of DS on QOL and FamilyPatients: 10.8Caregivers: NRNR80QOLProfessional impactCarer-QOLSINDRAHUINolan, 2006 [42]Coping in DSPatients: 10.2Caregivers: NRNR24Coping abilityHealthcare utilizationICNDRentz, 2015 [43]Caregiver burden in TSCPatients: 6.9Caregivers: 3978.9% female86% NHW65.5% college education or greater63% employed full-time275Psychosocial impactQOLPhysical healthHealthcare utilizationSurveySF-12HDISkalicky, 2018 [44]Cost of illness in TSCCaregivers: 3979% female86% NHW66% college education or greater64% employed275Healthcare utilizationEconomic burdenSurveyWPAIStrzelczyk, 2019a [45]Cost and Burden of DSPatients: 10.1Mothers: 42.1Fathers: 45.2Mothers: 56% employedFathers: 82% employed93Psychosocial impactQOLEconomic burdenHealthcare utilizationEQ-5D-3 LBDI-IIStzrelczyk, 2019b [46]Cost and burden of DSPatients: 8.162% employed93Psychosocial impactQOLEconomic burdenHealthcare utilizationEQ-5D-3 LBDI-IIWhittington, 2017 [47]Direct and indirect costs of DSCaregivers: NR72.73% employed34Direct and indirect costsEconomic burdenNHISWPAIWillems, 2021 [21]QOL in TSC and caregiversPatients: 9.8Caregivers: 4184.8% female184Psychosocial impactQOLProfessional impactEQ-5DBDI-IIMedian value reportedAbbreviations: DEE, developmental epileptic encephalopathy; QOL, quality of life; DS, Dravet Syndrome; OCBS, Oberst Caregiving Burden Scale; EQ-5D-5 L, 5-level EuroQol-5 Dimensions; WPAI, Work Productivity and Activity Impairment Questionnaire; NHIS, National Health Interview Survey; LGS, Lennox-Gastaut Syndrome; SF-36, 36-Item Short Form Health Survey Questionnaire; HADS, Hospital Anxiety and Depression Scale; TSC, Tuberous Sclerosis Complex; NHW, non-Hispanic White; REN, Rare Epilepsy Network; PROMIS, Patient-Reported Outcomes Measurement Information System; QOLCE, Quality of Life of Childhood Epilepsy Questionnaire; SCL-90-R, Symptom Checklist-90-Revised; PSQI, Pittsburg Sleep Quality Index; BSFC, Burden Scale for Family Caregivers; SINDRA, survey used to assess patient health-related quality of life; HUI, Health Utility Index; ICND, Impact of Childhood Neurological Disability Scale; SF-12, 12-Item Short Form Health Survey Questionnaire; HDI, Hamilton Depression Inventory; BDI-II, Beck’s Depression Inventory Second EditionFig. 2Burden studied in papers. Funnel plot demonstrating percent of manuscripts that reported each category of burden. QOL, quality of life
Indirect economic costs
The indirect economic costs as measured by impact on work are summarized in Table 3. Fifteen studies evaluated the economic impact and productivity loss due to the burden of caregiving [19–21, 29, 30, 32, 36–41, 44–47]. Primary outcomes were absenteeism and presenteeism. Mothers were significantly more impacted by productivity loss than fathers. Caregiving was primarily provided by unpaid caretakers.Table 3. Indirect costs of caregiving on work, quality of life, mental health, and opportunity costStudyReported Indirect CostsCampbell, 2018 [29]• 78% unable to work, 45% quit/lost job, 18% altered work situation• 70% slight anxiety, 33% moderate anxiety, 57% physical discomfort/pain, decreased QOL,• 27 fewer leisure hoursDomaradzki, 2023 [30]• 77.3% unable to work• 80% mental exhaustion, 81.3% physical fatigue, 74.7% negatively impacted QOL, 46.7% impacted sleep,• 66.6% leisure time given up, 46.7% negative impact on relationships, 73.4% lack of time for personal development, 41.4% feel isolatedGallop, 2010 [19]• 57.6% moderate-severe anxiety, 51.5% depression, 24.2% moderate-severe, decreased mental health component score compared to US GP• Decreased social functioning compared to GPGibson, 2014 [31]• 55% negatively impact activities, 13% brought partner further, 40% no time for other childrenGraffigna, 2013 [32]• 15% request emotional counseling• 50% unmet caregiver needs, 25% request more psychosocial supportGrau, 2021 [20]• 13% (mothers), 1.1% (fathers) quit/lost job, 60.3% altered work situationJansen, 2020 [34]• 58.8% unable to work, 21.2% quit/lost job, 34% altered work situation, 53.2% transitioned to part-time• 58.8% anxiety, 45.6% moderate-extreme, 70.7% depression, 53% pain/discomfort• Negative impact on relationships, 40.8% family, 50.7% social, 23.9% work colleaguesJensen, 2017 [35]• Increased anxiety, depression, sleep disturbance, PROMIS scores compared to GP, decreased physical conditioning compared to GP.• Decreased social functioning compared with GPKopp, 2008 [24]• 12.9% significant anxiety, 56.3% significant depression, 46.5% significant impacted QOLLagae, 2019 [36]• 81% of unemployed gave up job for caregiving, 65% took time off in last 4 weeks• 77% < 1 hr of leisure time/day, 46% of siblings gave up leisure time, 70% negative impact on family relationship, 80% impact on social relationshipsMaltseva, 2023 [37]• 33.3% (mother), 0.9% (father) Quit/lost job, 70.4% (mothers), 5.6% (fathers) altered work situation, 26.2% (mothers), 2.8% (fathers) reduced working hours• 35.3% significant anxiety, 23.1% significant depression, increased anxiety/depression HADS score compared to GP, 76.9% sleep disturbanceNabbout, 2018 [38]• 67% unable to work• 100% sleep disturbance• 100% no free time, 67% impact on leisure, negative impact on relationships 67% spouse, 78% family, 100% socialNabbout, 2019 [39]• 90% negative impact on work trajectory• 60% negative impact on emotional wellbeing, 70% physical impact, 75% impacted sleep• 80% impacted leisure time, 60% impact on social life, 90% negative impact on family relationshipsNabbout, 2020 [40]• 33% of mothers unable to work, 58% (mothers), 40% (fathers) altered work situation, 52% (mothers), 7.1% (fathers) interrupted work > 6 m• 19.5% mothers, 15.3% fathers rated health poor/very poor• > 50% negative impact on relationshipsGil-Nagel, 2023 [41]• 48.1% quit/lost job, 65.8% took time off• Mental health problems, 46.3% (some), 22.5% (a lot), 61.3% physical health problems• 35% negative impact on relationshipsNolan, 2006 [42]• Negative impact on relationships, 45.8% spouse, 37.5% family, 62.5% friends, 70% difficulty finding caregiverRentz, 2015 [43]• Decreased social functioning compared with GP• 42% mild to severe depression, decreased physical and mental component scores compared to GPSkalicky, 2018 [44]• 11% missed work, 38% impaired work timeSrtzelczyk, 2019a [45]• 31% (mother), 1% (father) Quit/lost job, 29% (mothers), 6% (fathers) reduced working hours• 38.2% anxiety, 46% depression, decreased QOL scores on EQ-VAS compared to GPStrzelczyk, 2019b [46]• 28% quit/lost job, 29% reduced working hours• Increased BDI scores, decreased QOL scores on EQ-VAS compared to DRE and SR groupsWhittington, 2017 [47]• 27.27% quit, 18.18% lost job, 18.18% altered working situation• 100% lost leisure time 2047 hrs/yrWillems, 2021 [21]• 13% (mother), 1.1% (father) Quit/lost job, 5.4% (mothers, fathers) altered work situation, 84.8% (mothers), 10.3% (fathers) reduced working hours• 45.7% depression, decreased EQ-VASSignificant indicates a score on the utilized scale that equates to a clinically significant level of pathology and/or statistically higher value than the general population
Nine papers reported 2.8–84.8% of caregivers took meaningful amount of time off work or reduced their working hours due to caregiving responsibilities [21, 34, 36, 37, 40, 41, 44–46]. This was reflected more among mothers than fathers, with estimated percentages ranging between 26.2–84.2% vs 2.8–29% respectively. Grau et al. and Strzelcyk et al. quantified the indirect productivity costs using the human capital method in two German cohorts and found them to be to be as high as €1109 for mothers and €163 for fathers (see Table 4) [20, 45]. This discrepancy is attributed to the significantly greater reduction in work hours among mothers compared to fathers. Grau et al. looking at a TSC cohort, report a higher economic burden than Strzelczyk et al. who assessed a Dravet syndrome cohort. This may suggest that TSC causes a greater indirect economic burden; however, more studies are needed [20, 45]. For the entire Dravet syndrome cohort, total productivity costs over 3 months were €4,398.6 for mothers and €358.2 for fathers, which were greater compared with the drug-resistant epilepsy (DRE) cohort (€1,469 for mothers and €72 for fathers) [46].Table 4. Quantified indirect economic costReduced hours (€/3 m)Missed work (€/3 m)Productivity (€/3 m)Grau, 2021 [20]Mothers€1109€732€1466Fathers€86€163€122Srtzelczyk, 2019a [45]Mothers€238€496Fathers€155€127Whittington, 2017 [47]3000(€/3 m): Euros over a 3-month period, (yr): year
Whittington et al. found employed caretakers reported missing an average of 47.6 eight-hour workdays (nearly 20% of total work hours) annually due to caregiving responsibilities, resulting in annual loss of ~2500/3 m) per patient with DS [47]. This is significantly higher than the economic cost reported by both Grau et al. and Strzelczyk et al.; however, this study examines a U.S. cohort compared to a German cohort, and this difference likely reflects variations in caregiver salaries between these two countries. Lagae et al. estimated annual out of pocket fees for childcare paid by caregivers to be $3371 (135–40,449) [36]. While Srtzelczyk et al. estimated informal care provided by family members to be valued at €1130 over 3 months [46].
Up to two-thirds of caregivers changed jobs or lost their employment due to caregiving responsibilities. Eight papers report 5.4–90% of caregivers had to alter their work situation due to caregiving [20, 21, 29, 34, 37, 39, 40, 47]. Whittington et al. found an average salary reduction of $16,053 [47]. Eleven papers reported 0.9%-48.1% of caregivers either quit or lost their job, and Lagae et.al found that 81% of already unemployed caregivers (34% of the study demographic) reported leaving their prior employment due to caregiving responsibilities [20, 21, 29, 34, 36, 37, 40, 41, 45–47]. Mean productivity costs over a three-month period were estimated at €1466, for mothers who quit working (€122 for fathers) [20]. Five papers demonstrated 33–38% of caregivers reported an inability to work due to caregiving responsibilities [29, 30, 34, 38, 40]. Selected statements made by caregivers are summarized in Table 5.Table 5. Caregiver statementsStudyIndirect economic costNabbout, 2018 [38]“My wife can’t work today, the attention on X is too important, and to leave her with somebody else is impossible today. I just have my license as a nurse and afterwards we discovered X’s illness and I saw my dream go away”Gallop, 2010 [19]“I was teaching in a secondary school. I only did six weeks because you just can’t cope with … so I gave up the teaching, and we’re in the, sort of, if you like, problem, not you know, we’re not absolutely desperate for money, but we’re very worried”Quality of life, depression, anxiety, and stressGraffigna, 2013 [32]“It is the disease of anguish: you always live in a state of anxiety about the future”Impact on physical healthJensen, 2017 [35]“I actually think one of the biggest differences in caring for a child with epilepsy versus maybe other chronic illnesses is your uncertainty at night, and the profound lack of sleep … The idea that you never punch out … is hard … I think you’re already dealing with something so emotionally heavy and physically exhausting during the waking hours that the sleep component is just a crazy facet of caregiving for someone with epilepsy”Opportunity cost of caregiving responsibilitiesNabbout, 2018 [38]“Emotionally we have a hard time getting involved in anything. How can you work when you know that the center of your life is your child’s condition. We are kind of detached from the day-to-day life of others”Jensen, 2017 [35]“We don’t even make plans to do things with him because with him being home, keeping the house a little darker, a little quieter, keeps us from spending any time in the hospital, such is the life we choose … I’ve accepted it. It’s what it is. Whatever gets you through the day, that’s what we do”Gallop, 2010 [19]“It’s very difficult to plan anything or do anything because you really didn’t know, you know, if people invited you out you didn’t whether you were going or not going right up until the last minute, because, you know, you could be in hospital before you knew where you were with him. You just didn’t know. You couldn’t plan anything”Indirect costs are a reinforcing cycleJensen, 2017 [35]“We gave up everything. We gave up our house … Just all that. I mean, we gave up all kinds of stuff. I mean, all the things we had worked up to. All the things we had purchased. All the things that we ever owned: A camper, a boat. We had to give them up too also because for him to qualify for Social Security and to get the things that he needed, you have to be poor to get those things”Nabbout, 2018 [38]“She has trouble speaking, she doesn’t talk like you and me, she has trouble articulating and she is constantly finding her words. She has a restricting vocabulary …she doesn’t speak correctly, and we have to figure out what she is trying to say”Positive impact of caregiving responsibilitiesJensen, 2017 [35]“I have full confidence in myself in what I’m doing with him. I have no doubts of what I’m doing. I mean, just because of what we’ve seen him through and just—you know, we now know after so many hospital visits that, you know, when you go in, you have to be his advocate. You have to ask questions. You have to demand things. You have to tell people; this is how I want it done. You know, because it’s so unique as far as in a hospital stay or just a group stay, or whatever. They don’t know, most people don’t know how to keep a kid with Dravet, how to keep them safe and all that kind of stuff. So it’s boosted my confidence with both [my son] and his sister as far as parenting”
Several studies also commonly found presenteeism among caretakers. Whittington et al. found employed caretakers reported ~77 workdays of annual presenteeism, resulting in approximately $12,000 per patient annually [47]. Caregivers reported 38% of work time was impaired due to TSC caregiving [44]. Jansen et al. found that 36.2% of caregivers reported that TSC caregiving negatively impacted their career progression [34].
Additional indirect economic costs arise from caregivers rearranging their families’ living situations to accommodate patient needs. Nabbout et al. found nearly 20% of families moved to a new house to be closer to their hospital or because they required a home better adapted to their child’s needs [38, 40].
Quality of life, depression, anxiety, and stress
The reported impacts on quality of life, depression, anxiety, stress and physical health in caregivers are summarized in Table 3. Caregivers have higher levels of anxiety and depression compared to the general population. Seven papers reported anxiety in as high as 70% of caregivers [19, 24, 29, 34, 35, 37, 45]. Nine papers reported depression in caregivers with ~23.3% reporting moderate-severe depression and as high as 70.7% with some depression [19, 21, 24, 34, 35, 37, 43, 45, 46]. Strzelcyk et al. found Beck depression inventory scores were significantly higher among DS caregivers, when compared to caregivers of children with DRE and seizure remission groups [46]. Three papers reported a general negative impact on emotional well-being or mental exhaustion and 15% of caregivers requested additional emotional counseling [30, 39, 41]. Caregivers take more psychotropic medications than the general public, Rentz et al., found 19.3% of caregivers were taking psychotropic or antidepressant medications, which is nearly twice the national average (11%) [43].
Kopp et al. found 46.5% of parents earned clinically significant scores (T score ⩾ 65) on the Parenting Stress Index [24]. Subscale analysis indicated that elevated total stress scores resulted from various factors, including seizures within the past 6 months, dysfunctional parent-child interactions, difficult child characteristics, a history of psychiatric diagnosis, low intellectual function, and elevated behavioral issues [24]. Selected statements made by caregivers are summarized in Table 4.
Higher rates of depression, anxiety, and stress negatively impact caretaker QOL [43, 45]. Seven studies quantitatively measured QOL among caregivers [21, 24, 29, 30, 43, 45, 46]. All but one found caregivers experienced decreased QOL. Stryzelcyk et al. found similar QOL to that of the average German population; however, they did find higher depression rates among DS caregivers [45]. QOL of DS caregivers was reduced even compared with caregivers of children with drug-resistant epilepsy and seizure-remission groups [46]. Willems et al. found significantly lower QOL among female caregivers compared with males; however, this finding is limited due to a lack of male survey participants [21]. Decreased QOL further impairs parents’ ability to fulfill caregiver responsibility. This impact of caregiving responsibilities on QOL creates a cycle that reinforces the negative impact of caretaker burden, thereby limiting their ability to cope and recover from the economic, psychosocial, and physical consequences. Using EQ-5D general health visual analogue scale (VAS), Campbell et al. found caregivers of patients with VAS < 65 reported a nearly twofold higher impact on mean work productivity (39.1 vs 76.9), and a 1.5-fold greater impact on leisure activities (55.1 vs 82.6) [29]. Rentz et al. found TSC caregivers who spent greater total hours researching the disease, finding doctors, and scheduling appointments had lower physical and mental health related QOL scores (p < 0.0025 and p < 0.05, respectively) and higher depressive symptoms scores ( < 0.0001) [43]. Domaradszki et al. found overall, 50.7% and 46.6% reported an inability to cope with depression and stress, respectively [30].
Impact on physical health
Eight papers reported negative physical impacts of caregiving, with three papers showing significantly lower mean physical component summary scores than the general US population [19, 29, 30, 34, 35, 39, 41, 43]. Mothers of children with DS had a worse perception of their own general health compared with fathers (19.5% vs. 15.3%, respectively, rated their own general health as poor or very poor) [40].
Sleep and fatigue were the most studied physical costs of caregiver responsibilities. Six studies evaluated sleep as a consequence of caregiver responsibilities [30, 33, 34, 37–39]. The impact on sleep may be due to increased stress and coping mechanisms for concerns related to sudden unexpected death in epilepsy (SUDEP) or nocturnal seizures. The use of auditory monitoring tools may also play a role.
Jensen et al. found sleep deprivation to be the most discussed burden by all caregivers, primarily driven by fear of their child experiencing a life-threatening seizure or SUDEP during sleep [35]. In a study examining caregiver sleep and stratifying outcomes into sleep disturbances, caregiver fatigue, and sleep-related impairment, Hesdorffer et al. found that the only factor associated with caregiver disturbance, fatigue, and sleep-related impairment was sharing a bed or room [33]. Use of an audio monitor (29%), a seizure alert device (13%), and keeping the door open (15%), were also associated with sleep disturbance and fatigue, but not with sleep-related impairment. This may suggest caregivers find ways to compensate during their waking hours for the impact of sleep disturbance and fatigue. On the other hand, pediatric nocturnal seizures were associated with caregiver sleep disturbance, but not with caregiver fatigue or sleep-related impairment. Overall, results suggest that caregiver’s sleep patterns were most affected by the unpredictable nature and worry of nocturnal seizures and SUDEP [33].
Opportunity cost of caregiving responsibilities
Table 2 summarizes the opportunity cost of caregiving. Many studies regarding opportunity cost of caregiving responsibilities used semi-structured interviews and open surveys. Selected statements made my caregivers are summarized in Table 4. Caregivers have decreased leisure time, and their social lives and relationships are impacted by caregiving responsibilities. As caregivers utilize their free time for caregiving responsibilities, this may lead to feelings of isolation and a reduction in their ability to cope with the burden of caregiving. Opportunity cost is driven in part by the unpredictable nature of DEE. Seven papers report leisure time given up; Whittington et al. specifically report a total of ~2047 hours annually [29–31, 36, 39, 47] Twelve papers reported caregiving had a negative impact on relationships with three papers finding lower social functioning scores compared to the general population [19, 30, 31, 34–36, 38–40, 42, 43]. Family relationships were the most frequently impacted.
Nabbout et al. found 18.4% of patient families had not taken a vacation in last 12 months, with 85% attributing this to their child having DS and the unpredictability of seizures. Families that were able to go on vacation indicated that their vacation desinations were heavily influenced by proximity to a PICU [40]. Using the Oberst Caregiving Burden Scale (OCBS), Campbell et al. found caregivers primarily spent their time providing transportation, followed by personal care of patients, additional household tasks, communication, symptom observation, coordinating resources, and then medical or nursing treatment [29].
Opportunity cost extends to siblings as well. Gibson et al. reports that 40% of caregivers have no time for their other children [31]. Lagae et al. found 46% of siblings missed leisure opportunities in the past four weeks so that their parents could take care of their sibling with DS. School attendance was not affected [36]. Among 24 families of DS to complete semi-structured interviews, Nolan et al. found both positive and negative effects. The most common positive effect was a caring nature and interest in helping others. The most common negative effect was decreased attention and resentment of the affected sibling [42].
In a cross-sectional survey of siblings of patients with LGS, DS, and other developmental and epileptic encephalopathies (DEE), Bailey et al. found that 18% of siblings aged 13–17 years and 29% of adult siblings felt that they had “lost their childhood.” Older siblings more frequently felt responsible for patients with DEE (63% of adult vs 41% of adolescent siblings) [28]. Bailey et al. found parents reported siblings of DEE patients had lower grades (20%) and demanded more attention (68%). 29% of parents reported altercations with siblings of DEE patients due to caregiving responsibilities [28].
Indirect costs are a reinforcing cycle
Resources are available for patients. However, caregivers sometimes describe making sacrifices in order to qualify for social services. Additionally, caregivers report gaps: Graffigna et al. reports 50% of caregivers have unmet needs, and Nolan et al. reports 70% had difficulty finding an alternate caregiver [32, 42]. Fear of seizures and communication barriers, such as issues with expressive communication or receptive communication, with patients make it particularly difficult for parents to defer caregiving responsibilities to paid services [38, 42].
Positive impact of caregiving responsibilities
Caregiving also has positive impacts, primarily through a sense of fulfillment and personal growth, with up to 90% of caregivers reporting some sense of fulfillment [30, 41]. 74% of parents responded that the experience of having a child with epilepsy brought them and their partner closer together. Themes of self-empowerment, resilience, and personal growth emerged when caregivers explained how having a child with epilepsy affected their families [31].
Discussion
Caregiver responsibilities of developmental epileptic encephalopathies occupy a considerable amount of time. Responsibilities cannot be easily supplemented or transferred to paid services due to the complex nature of the disease and patients’ communication limitations. Caregiving responsibilities place a substantial economic burden on families, primarily measured through productivity loss and changes in employment status [4, 8, 48]. This indirect cost disproportionately impacts female caregivers [20, 46]. Families report rearranging their lives—relocating, forgoing vacations, and sacrificing leisure time [29, 30, 38, 40, 47]. Feelings of loss of control, stress from the unknown, and worry about the future of their child are described [24, 32, 35, 38, 39]. Decreased quality of life and increased levels of anxiety, depression, and stress are seen among caregivers compared to peers in the population [19, 35, 37, 43]. Caregiving takes a toll on physical well-being leading to pain, fatigue, and sleep-related impairments [29, 30, 35, 37–41]. This leads to a decline in the physical health of caregivers compared to the general public [19, 35, 43]. Decreased leisure time leads parents to sacrifice their hobbies, personal ambitions, and interests, and has a negative impact on their social lives and relationships. Consequently, feelings of isolation are reported, which in turn limits their ability to effectively cope with the overall burden of caregiving [29, 30, 35, 38, 42, 43, 47].
Caregiving has positive aspects such as a sense of fulfillment, stronger family relationships, resilience, and personal growth [30, 41]. The overall measured impact of caregiving responsibilities tends to be reported with economic, psychosocial, and physical ramifications on caretakers well-being. Our findings suggest that this impact extends beyond parents and may also involve siblings, although the literature on siblings is generally lacking [28, 36, 42]. Patient characteristics such as communication impairment, behavioral issues, sleep issues, and frequent seizures correlate with higher caregiver burden and indirect costs [21, 33]. For this reason, it is more difficulty for parents to defer caregiving responsibilities to paid services, even if resources are not limited.
In the United States, there are programs to relieve indirect costs incurred by caregivers of children with developmental epileptic encephalopathies. These include Supplemental Security Income (SSI), the only source of federal income support targeted to families caring for children with disabilities. To qualify for SSI, total pre-tax monthly income is limited to 2,827 for a couple and countable assets are limited to 3000 if the child lives with two parents. SSI benefits average $650/month for a child with disability [49]. The Family and Medical Leave Act (FMLA) allows eligible employees to take unpaid leave to care for a family member with serious health condition, including children, without immediate threat of dismissal from the position. The maximum allowable protected length of time is 12 weeks per year [50]. There are no prescriptions for how employers account for loss of these employees’ work time [51]. Some disease specific patient advocacy organizations provide communities to help with families cope with caregiver burden. Many of these are typically from philanthropic support for one-time gifts. For example, the caregiver foundation of a non-profit based in Hawaii provides caregiver workshops, helps coordinate services and provides financial planning [52]. With this study we provide a summary of the existing literature and a framework for future investigation. For example, it may not be straightforward to qualify for social services, and caregivers may find that the services provided are inadequate in terms of both quantity and quality [35, 49]. Overrall, 50% of caregivers reported unmet needs, while 70% had difficulty finding an alternate caregiver [32, 42]. The indirect costs combined with barriers to access of resources create a reinforcing cycle, compounding the difficulties experienced by caregivers.
Strzelczyk et al. provide a comprehensive systematic review of the burden of DS, offering a detailed quantitative analysis that includes epidemiology, mortality, health-related QOL, and a strong focus on direct economic costs. The study also highlights the profound impact on caregivers, particularly in terms of quality-of-life disruptions and productivity losses. In contrast, this systematic review takes a broader approach by examining multiple DEE, including DS, TSC and LGS. This review highlights both shared indirect costs across syndromes and those unique to each condition. Rather than focusing on epidemiology and direct healthcare costs, it primarily explores indirect costs and their psychosocial effects on families. Through the discussion of themes such as caregiver career sacrifices, emotional strain, social isolation, and even some positive aspects of caregiving, such as personal growth, this review provides a broader perspective on the overall caregiver experience.
Overall, there is a paucity of research regarding the indirect cost to caregivers of patients LGS, TSC, and DS. To our knowledge, there has been no study published regarding the indirect costs of caregiving responsibilities for LGS patients beyond interview-based qualitative studies. The studies included in this review carry a high risk of bias, primarily due to limitations in study design and small sample sizes. While these factors may somewhat limit the generalizability of the findings, they do not diminish the importance of the insights gained. The high risk of bias also suggests that the current evidence base may not fully capture the complexity or variability of indirect costs in patients with DEE. This further highlights a significant gap in the literature and underscores the need for more rigorous, large-scale studies to better understand and quantify the indirect costs for patients with DEE. In order to bridge this gap, semi-structured interviews can be paired with quantitative surveys such as the Work Productivity and Activity Impairment Questionnaire and the Impact on Family Scale. This would provide the ability to catalog the indirect costs and burden of care specifically amongst LGS caregivers and estimate associated the monetary costs.
Limitations include a high risk of bias due to the study design and lack of comparison group for many of the studies. No studies were found investigating the impact or efficacy of policies or initiatives intended to alleviate indirect costs and caregiver burden. Few studies included demographic data detailing socioeconomic status and race or ethnicity. Socioeconomic factors may constitute a key component of adherence in pediatric epilepsy [5]. Studies that did include demographic and socioeconomic data showed subjects were primarily female, highly educated, and Non-Hispanic White. Understanding caregiver burden among patients from a diverse and inclusive perspective is essential. Furthermore, this systematic review is also limited to studies published prior to May 2023 and to the three databases searched which is not exhaustive.
Conclusions
The indirect cost and caregiver burden to families of patients with developmental epileptic encephalopathies are significant, and contributors are multifactorial. Economic, psychosocial, and physical aspects on caregivers impacts not only parents but also the entire family unit, including siblings. Further studies are necessary to understand and quantify the total indirect cost and caregiver burden for families of patients with DEE. It is essential to develop this knowledge for families to make informed health care decisions to facilitate sustainable long-term outcomes. Subsequently, directions for the future include health care delivery design and implementation of interventions and policies to address and alleviate these indirect costs and caregiver burden.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baca CB, Vickrey BG, Hays RD, Vassar SD, Berg AT. Differences in child versus parent reports of the child’s health-related quality of life in children with epilepsy and healthy siblings. (1524-4733 (Electronic)).10.1111/j.1524-4733.2010.00732.x PMC 306529520561342 · doi ↗ · pubmed ↗
- 2Yu Z, Shao Q, Hou K, Wang Y, Sun X. The experiences of caregivers of children with epilepsy: a meta-synthesis of qualitative research studies. (1664-0640 (Print)).10.3389/fpsyt.2022.987892 PMC 951354336177220 · doi ↗ · pubmed ↗
- 3Yousaf MN, Naqvi HA, Kane S, Chaudhary FS, Hawksworth J, Nayar VV, et al. Cerebrospinal fluid liver pseudocyst: a bizarre long-term complication of ventriculoperitoneal shunt: a case report. World J Hepatol. 2023;15(5):715–24.10.4254/wjh.v 15.i 5.715PMC 1025128237305372 · doi ↗ · pubmed ↗
- 4Page MJ, Mc Kenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA, 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372.10.1136/bmj.n 71PMC 800592433782057 · doi ↗ · pubmed ↗
- 5Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355(i 4919).10.1136/bmj.i 4919 PMC 506205427733354 · doi ↗ · pubmed ↗
- 6Hesdorffer DC, Kroner BL, Shen J, Farrell K, Roberds S, Fureman B. Factors associated with caregiver sleep quality related to children with rare epilepsy syndromes. J Educ Chang Pediatrics: X. 2020;2.10.1016/j.ympdx.2020.100021 PMC 1023654937332626 · doi ↗ · pubmed ↗
- 7Foundation TC. The caregiver foundation-services. Available from: https://thecaregiverfoundation.org/the-caregiver-foundation-services.