Evaluation of the Accuracy of Intraocular Lens Power Calculation Formulas for Cataract Surgery in Patients with Keratoconus
Firouze Hatami, Sina Khosravi Mirzaei, Mohammad Ali Javadi, Sepehr Feizi, Sare Safi, Seyed Bagher Hosseini

TL;DR
This study compares the accuracy of different formulas used to calculate intraocular lens power for cataract surgery in patients with keratoconus.
Contribution
The study evaluates and compares the performance of various IOL power calculation formulas specifically in patients with keratoconus.
Findings
The SRK/T formula had the lowest mean absolute error (MAE) and highest accuracy in predicting refractive outcomes.
The Holladay 1 and Hoffer Q formulas resulted in a hyperopic refractive shift, while SRK II tended toward myopia.
Among modern formulas, Barrett True-K showed the highest accuracy in eyes with keratoconus.
Abstract
To compare the refractive accuracy of different intraocular lens (IOL) power calculation formulas in eyes with keratoconus (KCN) undergoing cataract surgery. This retrospective case series included the medical records of patients with KCN who underwent optical biometry and cataract surgery with IOL implantation. The predicted spherical equivalent (SE) values were calculated using the Holladay 1, Hoffer Q, SRK/T, and SRK II formulas. Additionally, a subgroup analysis was performed for eyes with available data on anterior chamber depth to compare the accuracy of Haigis, Barrett Universal II, Barrett True-K, EVO 2.0, Kane, and Kane KCN formulas. The mean prediction error (PE), mean absolute error (MAE), median absolute error, and the percentage of eyes within a PE of ± 0.25 diopters (D), ± 0.50 D, ± 0.75 D, and ± 1.00 D were calculated. Forty-seven eyes of 30 patients were included.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
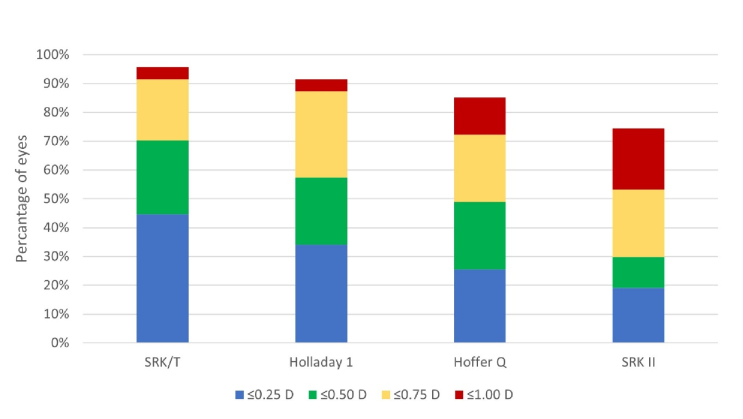 Figure 1
Figure 1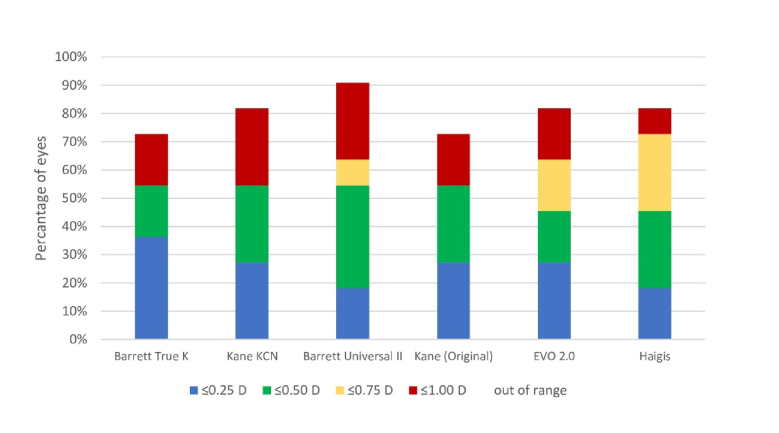 Figure 2
Figure 2|
|
|
| |
| Age (year) | 60.89 | 9.49 | 44 to 77 |
| Axial length (mm) | 23.89 | 1.61 | 21.35 to 26.96 |
| Keratometry (flat) (D) | 45.22 | 2.32 | 40.61 to 49.20 |
| Keratometry (steep) (D) | 48.28 | 2.41 | 43.28 to 52.33 |
| Mean keratometry (D) | 46.75 | 2.22 | 42.26 to 50.44 |
| IOL power (D) | 17.23 | 4.28 | 4.00 to 23.00 |
| Preoperative spherical equivalent (D) | –2.61 | 3.44 | –11.25 to 2.25 |
| Preoperative BCVA (logMAR) | 0.51 | 0.35 | 0.15 to 2.00 |
| D, diopters; IOL, intraocular lens; SD, standard deviation; BCVA, best corrected visual acuity; logMAR, logarithm of the minimum angle of resolution | |||
|
|
|
|
|
|
|
|
| Alcon AcrySof SN60WF | 119.0 | 5.64 | 1.84 | –0.769 | 0.234 | 0.217 |
| Alcon AcrySof SA60AT | 118.8 | 5.44 | 1.67 | –0.111 | 0.249 | 0.179 |
| Alcon AcrySof Toric SN6AT | 119.2 | 5.81 | 1.98 | –0.323 | 0.213 | 0.208 |
| Alcon AcrySof MA60AC | 119.2 | 5.67 | 1.90 | 0.229 | 0.011 | 0.205 |
| Bausch & Lomb enVista toric MX60T | 119.2 | 5.68 | 1.91 | 1.46 | 0.400 | 0.100 |
| Bausch & Lomb enVista MX60P | 119.2 | 5.68 | 1.91 | 1.46 | 0.400 | 0.100 |
|
|
|
|
|
|
| SRK/T | 0.39 | –0.14 | 0.47 | 0.29 |
| Holladay 1 | 0.48 | 0.24 | 0.59 | 0.43 |
| Hoffer Q | 0.59 | 0.41 | 0.63 | 0.54 |
| SRK II | 0.87 | –0.77 | 0.82 | 0.72 |
| MAE, mean absolute error; MPE, mean prediction error; MedAE, median absolute prediction error; PE SD, standard deviation of the prediction error (all values are expressed in diopters). | ||||
|
|
|
|
|
|
| Barrett True-K | 0.54 | –0.27 | 0.65 | 0.31 |
| Kane KCN | 0.56 | –0.04 | 0.70 | 0.45 |
| Barrett Universal II | 0.63 | 0.12 | 0.82 | 0.37 |
| Kane (Original) | 0.65 | 0.04 | 0.87 | 0.45 |
| EVO 2.0 | 0.67 | 0.15 | 0.88 | 0.52 |
| Haigis | 0.68 | 0.20 | 0.87 | 0.61 |
| MAE, mean absolute error; MPE, mean prediction error; MedAE, median absolute prediction error; PE SD, standard deviation of the prediction error; KCN, keratoconus (all values are expressed in diopters). | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Visual Impairment Studies · Corneal surgery and disorders · Intraocular Surgery and Lenses
INTRODUCTION
Keratoconus (KCN) is a progressive non-inflammatory corneal ectasia leading to central or paracentral corneal thinning and reduction in visual acuity.^[1,2]^ Individuals with KCN often experience an earlier onset of cataracts compared to those with normal eyes.^[3]^ The surgical management of cataracts in patients with KCN is more challenging due to the corneal changes, making the accurate prediction of refractive outcomes notably more difficult than in normal eyes.^[4,5]^
The refractive outcomes following intraocular lens (IOL) implantation in non-KCN eyes typically demonstrate a high level of satisfaction, with 72% to 80% of eyes achieving refractive error within 0.5 diopters (D),^[6]^ while the results for eyes with KCN are often less favorable.^[7]^ The IOL power calculation formulas are designed for normal eyes, and using them for eyes with KCN could cause errors in postoperative refraction. This difference in outcomes could have several reasons. First, IOL power calculation formulas assume the ratio of the anterior to posterior corneal power based on established eye models, which are not designed for eyes with KCN.^[8]^ Second, effective lens position (ELP) estimation is calculated using the corneal power; therefore, false corneal power calculation leads to inaccurate ELP.^[9]^ Third, traditional keratometry measurements rely on the assumption of a constant corneal curvature along both the flat and steep meridians; however, this assumption may be inaccurate in keratoconic eyes, where irregularities in corneal curvature and variability in a particular meridian make the principal power meridian measurements non-orthogonal.^[10,11]^
Various approaches have been suggested to improve outcomes in eyes with KCN. These include targeting additional myopia^[12]^ and measuring the anterior and posterior corneal curvature using Scheimpflug tomography and then converting these values to an equivalent keratometry reading that can be used in selected formulas.^[13]^ Identifying the most accurate formula may further contribute to optimizing outcomes. Previous studies have identified different formulas, such as SRK/T,^[14,15]^ Kane KCN,^[11]^ Barrett Universal II,^[16]^ and Barrett True K,^[17]^ as being more accurate than others. Older formulas, such as SRK II, have also been reported to yield better results in mild KCN.^[18]^ Considering that different formulas employ different factors to estimate desired target refraction, it is important to assess the accuracy of their prediction.
In this study, we aimed to compare different IOL power calculation formulas to find the most accurate formula in predicting refractive outcomes in patients with KCN.
METHODS
This retrospective consecutive case series adheres to the tenets of the Declaration of Helsinki and was approved by the Research Committee of Ophthalmic Research Center affiliated with Shahid Beheshti University of Medical Sciences, Tehran, Iran (approval number: IR.SBMU.ORC.REC.1403.001). All cataract surgeries were performed by a single surgeon (MAJ) from March 2015 to July 2023 at a single center.
All patients were diagnosed with KCN and cataract through clinical examination and corneal topography. Patients with previous ocular surgery, history of ocular inflammation, glaucoma, diabetic retinopathy, macular disorders, and intraoperative or postoperative complications were excluded. Before surgery, a comprehensive examination was performed, including assessment of best-corrected visual acuity (BCVA), intraocular pressure, standard keratometry, subjective manifest refraction, and fundoscopy. Biometric values, including keratometry values and axial length measurements, were obtained using IOLMaster 500 optical biometer (software version 7.5; Carl Zeiss Meditec AG, Jena, Germany). In addition, the severity of KCN was defined in three stages. Eyes with a mean central keratometry of 48 D, between 48 and 53 D, and 53 D were classified as stage 1, stage 2, and stage 3, respectively.^[15,19]^ Eyes with unmeasurable refraction, corneal radii 55, corneal scar, corneal perforation, or corneal thickness 200 µm were considered as stage 4 KCN and were excluded from this study.^[19]^
All patients underwent sutureless cataract surgery and IOL implantation within the capsular bag through a 2.8-mm corneal tunnel incision. Postoperative care included chloramphenicol 0.5% eye drops administered every 6 hours for 1 week, and betamethasone 0.1% eye drops initiated every 3 hours and gradually tapered over 4–6 weeks. All patients were followed up for a minimum of 1 month. At the postoperative follow-ups, patients were first examined by an ophthalmologist. Then, a certified optometrist measured subjective refraction (spherical equivalent [SE], astigmatism, and axis orientation) and BCVA of all patients using a Snellen chart.
IOL Power Calculation
The Holladay 1,^[20]^ Hoffer Q,^[21]^ SRK/T,^[22]^ and SRK II^[23,24]^ formulas were obtained by inputting the required values into Excel software (Microsoft Corp, Redmond, WA, USA). Furthermore, for eyes with available anterior chamber depth (ACD) data, the accuracy of six newer formulas, including Haigis,^[25]^ Barrett Universal II,^[26]^ Barrett True-K,^[27]^ EVO 2.0,^[28]^ Kane,^[29]^ and Kane KCN,^[29]^ was evaluated using Excel or online calculators. While different types of IOLs were implemented, optimized lens constants provided by the User Group for Laser Interference Biometry (ULIB) were used.^[15,30]^
The prediction error (PE) for each formula was considered as the actual postoperative SE refraction minus the predicted SE refraction. A negative PE signifies a greater postoperative myopia compared to the anticipated refraction, while a positive PE indicates a more hyperopic outcome. The mean PE, its standard deviation (SD), the mean absolute error (MAE), and the median absolute error (MedAE) were calculated. In addition, the percentage of eyes with a PE within 0.25 D, 0.50 D, 0.75 D, and 1.00 D was evaluated.
Statistical Analysis
All statistical analyses were performed using SPSS software (IBM Corp. Version 27.0, Armonk, NY, USA). The normality of data distribution was assessed with the Shapiro-Wilk test. Due to the non-normal distribution of data, the Friedman test was used to determine the statistical significance between the MAE of each formula. Then, the Wilcoxon signed-rank test was performed to compare formulas with each other. To calculate the percentage of eyes within 0.50 D and 1.00 D ranges, the Cochran's Q test with Bonferroni correction was used. For all analyses, a P-value 0.05 was considered statistically significant.
RESULTS
A total of 47 eyes from 30 patients (16 males) with a mean age of 60.89 9.49 years were included in this study. Table 1 shows the demographics, baseline clinical characteristics, and ocular biometry data. Six IOL types were used for patients: Alcon AcrySof SN60WF (23 eyes), Alcon AcrySof SA60AT (12 eyes), Alcon AcrySof Toric SN6AT (2–9) (4 eyes), Alcon AcrySof MA60AC (1 eye), Bausch & Lomb enVista toric MX60T (4 eyes), and Bausch & Lomb enVista MX60P (3 eyes). The constants used for each IOL model are displayed in Table 2. The mean postoperative SE was –0.50 0.40 D. After cataract surgery, the mean BCVA improved in all eyes and reached 0.21 0.10 logMAR (logarithm of the minimum angle of resolution). Thirty-two eyes were classified as stage 1 KCN, and fifteen eyes as stage 2. None of the included eyes belonged to stage 3.
Table 3 shows the refractive PE for each formula. The SRK/T and SRK II formulas resulted in a negative mean PE, indicating a tendency toward a myopic error. On the other hand, Holladay 1 and Hoffer Q had a positive mean PE, showing a hyperopic tendency for prediction. The Friedman test showed that there was a significant difference among all four formulas (P 0.001). SRK/T had the lowest MAE, and the difference was statistically significant compared to the values obtained by Hoffer Q and SRK II (P 0.05), but there was no significant difference between the SRK/T and the Holladay 1 (*P *= 0.16). Similarly, Holladay 1 had a significantly lower MAE compared to the Hoffer Q and the SRK II formulas. A significant correlation was also found between Hoffer Q and SRK II (P = 0.014). SRK II predicted the postoperative SE with the highest MAE, which was significantly less accurate than those obtained by all other formulas.
Figure 1 shows the percentage of eyes within PE of 0.25 D, 0.50 D, 0.75 D, and 1.00 D for Holladay 1, Hoffer Q, SRK/T, and SRK II formulas. The PE within 0.50 D was calculated in 33 eyes (70.2%) with SRK/T, 27 eyes (57.44%) with Holladay 1, 23 eyes (48.93%) with Hoffer Q, and 14 eyes (29.78%) with SRK II. Comparing the percentage of eyes within 0.50 D, we found significant differences between the SRK/T and SRK II formulas (P 0.001) and the Holladay 1 and SRK II formulas (P = 0.023). Moreover, within the 1.00 D range, the SRK/T and Holladay 1 formulas had a significant difference with the SRK II (*P *= 0.003 and P = 0.031, respectively). Other comparisons between formulas showed insignificant differences.
Due to the unavailability of ACD for some eyes, the postoperative SE prediction of Haigis, Barrett Universal II, Barrett True-K, EVO 2.0, Kane, and Kane KCN formulas were performed on a sample size of 11 eyes (seven patients). Among these eyes, four types of IOL were implemented, including Alcon AcrySof SN60WF (two eyes), Alcon AcrySof Toric SN6AT (2–9) (two eyes), Bausch & Lomb enVista toric MX60T (four eyes), and Bausch & Lomb enVista MX60P (three eyes). Seven eyes were classified as stage 1, and four eyes as stage 2 KCN. Table 4 lists the refractive PE of the Haigis, Barrett Universal II, Barrett True-K, EVO 2.0, Kane, and Kane KCN formulas. The Barrett True-K and Kane KCN exhibited a negative mean PE, whereas the other four formulas demonstrated a positive mean PE. The Friedman test revealed no statistically significant difference in the MAE between these formulas (P = 0.735). Barrett True-K demonstrated the lowest MAE (0.54 D), while Haigis exhibited the highest MAE (0.68 D). The proportion of eyes within a PE of 0.50 D was 54.5% for the Barrett True-K, Kane KCN, Barrett Universal II, and Kane formulas. For a PE of 1.00 D, the Barrett Universal II demonstrated the highest proportion of eyes, at 90.9% [Figure 2].
Stacked histograms comparing the percentage of eyes within different diopter (D) ranges of absolute prediction error for spherical equivalent (traditional formulas).
Stacked histograms comparing the percentage of eyes within different diopter (D) ranges of absolute prediction error for spherical equivalent (modern formulas).
DISCUSSION
Our study investigated the accuracy of IOL power calculation formulas in patients diagnosed with KCN. The SRK/T formula had the lowest MAE, indicating its superior accuracy compared to other formulas. The SRK II formula, with the highest MAE, was the least accurate. Among the six newer formulas (Haigis, Barrett Universal II, Barrett True K, EVO 2.0, Kane, and Kane KCN), Barrett True-K yielded the lowest MAE. The SRK/T formula demonstrated superior accuracy, with 70% of eyes achieving a PE within 0.50 D, while in normal eyes, this rate is approximately 75%.^[6,31]^ Notably, previous studies reported that the highest percentage of eyes achieving a PE within 0.50 D was 44% and 50% for patients with KCN.^[11,15]^ In KCN, the predictive accuracy of all formulas further decreases as ectasia severity progresses.^[16]^ The reduced accuracy in KCN can be attributed to several factors. First, IOL calculation formulas are primarily designed for patients with normal anterior and posterior corneal curvature, and IOL calculation formulas heavily rely on anterior corneal power while estimating posterior corneal power. Implementing these formulas for eyes with KCN that have asymmetry in corneal curvatures from early stages could reduce their final accuracy.^[32]^ Additionally, in higher stages of KCN, the ratio between the anterior and posterior curvatures could be even more disrupted, highlighting the importance of posterior curvature measurement.^[32]^ Heath et al^[17]^ showed that integrating total keratometry, rather than simply standard keratometry, improves the accuracy of IOL calculation formulas in patients with KCN. For all formulas in which both standard keratometry and total keratometry were available, applying total keratometry resulted in a lower MAE for each formula. Second, using the standard keratometric index (1.3375) for these patients may also lead to inaccurate IOL power estimations.^[33,34]^
In line with our findings, Savini et al^[15]^ and Kamiya et al^[35]^ found that SRK/T had the lowest MAE and the highest percentage of eyes within 0.50 D of PE (44% and 36 %, respectively). In another study, the superiority of the SRK/T over the Holladay 1, Hoffer Q, and SRK II formulas has been shown.^[14]^ However, these studies^[14,15][35]^ reported a positive MPE for SRK/T. This might be related to the inclusion of severe KCN cases in their studies, whereas our investigation focused on stages 1 and 2 of KCN. Studies suggest a correlation between increased KCN severity and higher PE, potentially leading to a hyperopic shift.^[35,36]^ Kane et al^[11]^ found a negative MPE for SRK/T in mild cases of KCN. Additionally, among IOL power calculation formulas (Barrett Universal II, Haigis, Hoffer Q, Holladay 1, Holladay 2, Kane, and SRK/T), the SRK/T formula showed the lowest tendency toward hyperopic refractive surprise. As described by Hagis et al^[37]^ and Sheard et al,^[38]^ SRK/T has a tendency toward myopic PE, and this could balance the hyperopic tendency seen in patients with KCN. Notably, studies have also shown that SRK/T is the most accurate formula in long eyes.^[21]^ Although in our study, only eight patients (17.02%) had an AL of 26 mm, the SRK/T was the most accurate formula.
In our study, Holladay 1 resulted in a higher MAE compared to SRK/T, but the difference between these two formulas was not significant, suggesting that Holladay 1 may also be a reliable option for IOL power calculation in patients with KCN. Kamiya et al^[35]^ reported that among several IOL calculation formulas, Holladay 1 exhibited the second lowest MAE compared to SRK/T, with no statistically significant difference noted. Additionally, they identified a significant difference between the SRK/T and Hoffer Q formulas, which is consistent with our research findings. Similar studies have also found higher MEA for Holladay 1 and Hoffer Q compared to SRK/T.^[11,15][16][17]^
Kamiya et al^[35]^ identified the SRK II as having the highest MAE and a negative MPE. In another study conducted by Hashemi et al,^[14]^ SRK II had a higher MEA compared to SRK/T in all stages of KCN. However, Thebpatiphat et al^[5]^ reported the SRK II formula to be more accurate for IOL power calculation in mild KCN compared to the SRK/T formula. Nevertheless, their study included only five eyes, limiting the generalizability of their findings due to insufficient sample size for statistical analysis.
A few studies have compared the accuracy of Haigis, Barrett Universal II, EVO 2.0, and Kane formulas in patients with KCN. Wang et al^[16]^ showed the statistically significant superiority of the Barrett Universal II over Haigis in KCN stages 1 and 2. Similarly, Savini et al^[15]^ reported a lower MedAE with Barrett Universal II compared to Haigis. Another study found that the Barrett True-K had a lower MAE compared to the Kane, Kane KCN, Barrett Universal II, EVO 2, and Haigis formulas in eyes with severe and non-severe KCN.^[17]^
In another study by Kane et al,^[11]^ Kane KCN was the most accurate formula. In KCN stage 1, the Kane KCN formula had a significantly lower MAE than both Barrett Universal II and Haigis.^[11]^ In our study, Kane KCN also had a lower MAE compared to other modern formulas except Barrett True-K; however, no statistical significance was found. These differences in outcomes may be attributed to differences in KCN stages or biometric values, as well as differences in sample size. Additionally, another study reported that Barrett Universal II exhibited a lower MAE compared to the Kane and Haigis formulas among all patients,^[11]^ which aligns with our findings.
Our study had several limitations. First, the sample size was relatively small, and patients with stage 3 KCN were not included. Second, the use of different types of IOLs prevented the optimization of IOL constants due to the retrospective design of the study. Instead, we used the IOL constant from the ULIB website, which is recommended by Savini et al^[15]^ and Hoffer et al.^[39]^ Third, the unavailability of lens thickness measurements precluded the assessment of some formulas that require this parameter. Fourth, due to the limited availability of ACD, modern formulas were investigated with fewer cases. Moreover, the distribution of KCN stages was different in this subgroup compared with the total sample size. These factors hindered the comparison of traditional and modern formulas with each other. Fifth, our calculations relied solely on anterior corneal curvature, and incorporating total corneal power by measuring both anterior and posterior corneal curvatures might have enhanced the precision of our calculations.
In summary, the SRK/T formula was the most accurate IOL power calculation formula for patients with KCN. The Holladay 1 formula, with the second lowest MAE, was an alternative choice for these patients. Regarding newer formulas, Barrett True-K had the lowest MAE. However, our findings revealed lower predictive accuracy in KCN compared to normal eyes, indicating the challenge in IOL power calculation for KCN and the necessity for further investigation.
Financial Support and Sponsorship
None.
Conflicts of Interest
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Krachmer JH Feder RS Belin MW Keratoconus and related noninflammatory corneal thinning disorders Surv Ophthalmol 198428293322623074510.1016/0039-6257(84)90094-8 · doi ↗ · pubmed ↗
- 2Asimellis G Kaufman EJ Keratoconus 201729262160 · pubmed ↗
- 3Thebpatiphat N Hammersmith KM Rapuano CJ Ayres BD Cohen EJ Cataract surgery in keratoconus Eye Contact Lens 2007332442461787362710.1097/ICL.0b 013e 318030 c 96d · doi ↗ · pubmed ↗
- 4Aiello F Nasser QJ Nucci C Angunawela RI Gatzioufas Z Maurino V Cataract surgery in patients with keratoconus: Pearls and pitfalls Open Ophthalmol J 2017111942002893233510.2174/1874364101711010194 PMC 5585461 · doi ↗ · pubmed ↗
- 5Thebpatiphat N Hammersmith KM Rapuano CJ Ayres BD Cohen EJ Cataract surgery in keratoconus Eye Contact Lens 2007332442461787362710.1097/ICL.0b 013e 318030 c 96d · doi ↗ · pubmed ↗
- 6Melles RB Holladay JT Chang WJ Accuracy of intraocular lens calculation formulas Ophthalmology 20181251691782895107410.1016/j.ophtha.2017.08.027 · doi ↗ · pubmed ↗
- 7Yahalomi T Achiron A Hecht I Arnon R Levinger E Pikkel J Refractive outcomes of non-toric and toric intraocular lenses in mild, moderate and advanced keratoconus: A systematic review and meta-analysis J Clin Med 20221124563556658310.3390/jcm 11092456 PMC 9101494 · doi ↗ · pubmed ↗
- 8Camps VJ Piñero DP Caravaca-Arens E de Fez D Pérez-CambrodíRJ Artola A New approach for correction of error associated with keratometric estimation of corneal power in keratoconus Cornea 2014339609672509016210.1097/ICO.0000000000000190 · doi ↗ · pubmed ↗