Role of Trace Elements in Diabetic Retinopathy: A Systematic Review
Niranjan Gopal, Deepa Telgote, Mustakiz Z Manir, Anjali S, Utsav Haldar, Dnyanesh Amle

TL;DR
This systematic review explores how imbalances in trace elements like magnesium and zinc are linked to diabetic retinopathy, suggesting they could serve as early biomarkers for the condition.
Contribution
The study systematically reviews the role of specific trace elements in diabetic retinopathy, highlighting their potential as biomarkers for risk stratification.
Findings
Lower serum levels of magnesium, zinc, manganese, and chromium are consistently observed in diabetic retinopathy patients.
Selenium shows a U-shaped relationship with increased DR risk at both low and high levels.
Iron dysregulation, including deficiency and ferroptosis, is linked to retinal hypoxia and oxidative stress in DR.
Abstract
Diabetic retinopathy (DR) is a leading cause of vision impairment worldwide and a major microvascular complication of type 2 diabetes mellitus (T2DM). While chronic hyperglycemia remains the principal driver of DR, growing evidence suggests that dysregulation of essential trace elements, including magnesium, zinc, manganese, chromium, selenium, and iron, may contribute to retinal microvascular injury through oxidative stress and impaired endothelial function. This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines, with a comprehensive search of PubMed, Scopus, Embase, Web of Science, Cochrane Library, and Google Scholar for studies published between January 2000 and June 2024. Search terms included "diabetic retinopathy," "trace elements," "magnesium," "zinc," "manganese," "chromium,"…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
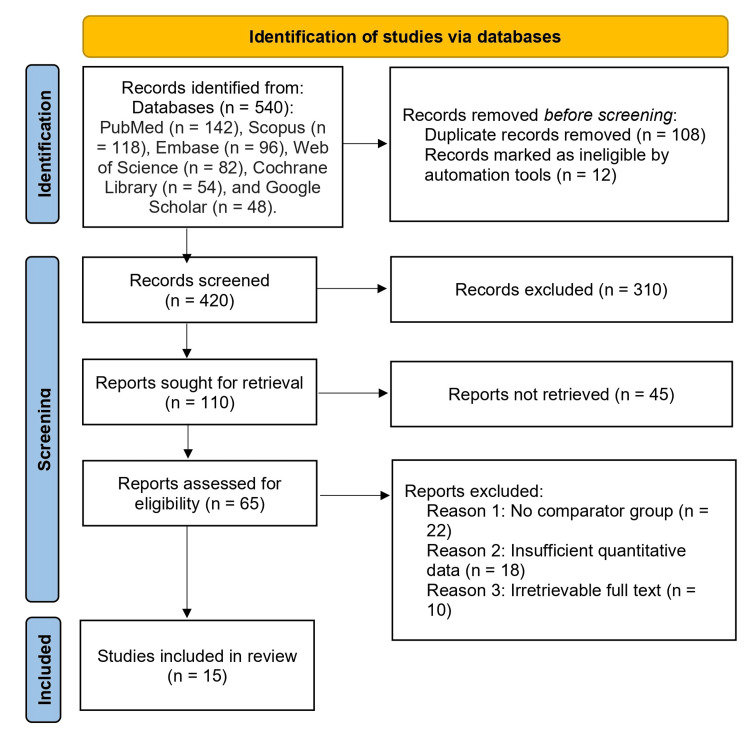 Figure 1
Figure 1| Author | Study design | Assessment tool | Risk of bias | Key limitation |
| Zhu et al. [ | Retrospective study | JBI checklist (cross-sectional) | Moderate | Limited control for confounding factors |
| Shivakumar et al. [ | Cross-sectional | JBI | Moderate | Small sample size; single-center study |
| Alkhalidi et al. [ | RCT (single-blind) | Cochrane RoB 2 | Low | Short duration; no long-term follow-up |
| Chen et al. [ | Cross-sectional (NHANES) | JBI | Low | Secondary data; possible reporting bias |
| Chen et al. [ | Cross-sectional (NHANES 2005–08) | JBI | Low | Cross-sectional design limits causality |
| Kumar et al. [ | Cross-sectional | JBI | Moderate | Potential selection bias; hospital-based sample |
| Xu et al. [ | Cross-sectional | JBI | Moderate | No adjustment for dietary intake or duration of DM |
| Dascalu et al. [ | Systematic review | JBI (systematic reviews) | Low | Heterogeneity among included studies |
| Miao et al. [ | Narrative review | JBI (narrative review) | Moderate | Lack of quantitative synthesis |
| Zhang et al. [ | NHANES (2011-2020) | JBI | Low | Limited to the U.S. population; self-reported data |
| Nugrahani et al. [ | Meta-analysis | JBI (systematic reviews) | Low | Between-study heterogeneity |
| Ghosh et al. [ | RCT (double-blinded) | Cochrane RoB 2 | Moderate | Small sample; incomplete blinding |
| Sonkar et al. [ | Observational | JBI | Moderate | No adjustment for confounding variables |
| Ganiger et al. [ | Case-control | JBI | Moderate | Single-center; small sample |
| Srikanth [ | Case-control | JBI | Moderate | Limited generalizability; small sample size |
| Author & year | Country | Study design | Sample size | Population | Trace element studied | Comparator group | Outcome measured |
| Zhu et al. [ | China | Retrospective study | 112 | T2DM patients with and without DR & healthy controls | Zinc, manganese | DR vs non-DR vs controls | Serum Zn and Mn levels and correlation with DR |
| Shivakumar et al. [ | India | Cross-sectional | 104 | T2DM patients with and without DR | Magnesium | DR vs No DR | Mean serum Mg level and correlation with DR severity |
| Alkhalidi et al. [ | Iraq | RCT (single-blind) | 60 | T2DM | Chromium | Chromium supplement (200 mcg BID) + standard drug vs standard drug only | Impact of chromium supplementation on glycemic parameters |
| Chen et al. [ | USA | Cross-sectional (NHANES) | 645 | Adults with T2DM | Selenium | DR vs non-DR | Association between Se and DR |
| Chen et al. [ | USA | Cross-sectional (NHANES 2005-08) | 5321 | T2DM | Iron | DR vs No DR | Serum iron levels & DR prevalence |
| Kumar et al. [ | India | Cross-sectional | 250 | T2DM patients | Magnesium | Normal Mg vs Low Mg groups | Prevalence of NPDR, PDR |
| Xu et al. [ | China | Cross-sectional | 239 | Prediabetes & T2DM | Magnesium | Non-diabetic controls vs T2DM | Association of Mg levels with DR & other complications |
| Dascalu et al. [ | Romania | Systematic review | – | T2DM patients | Zinc | DR vs non-DR vs healthy | Serum zinc levels, DR severity |
| Miao et al. [ | China | Narrative review | – | T2DM patients | Zinc | DR vs non-DR | Association of zinc with DR |
| Zhang et al. [ | USA | NHANES (2011-2020) | 1583 | T2DM patients | Manganese, selenium | DR vs No DR | Association between Mn and Se with DR |
| Nugrahani et al. [ | Multi-country | Meta-analysis | 2132 | T2DM | Manganese (MnSOD polymorphism) | VV vs AA genotypes | DR risk (OR, 95% CI) |
| Ghosh et al. [ | India | RCT (double-blind) | 100 | Uncontrolled T2DM | Chromium | Study group vs placebo | Effect of Cr supplementation on HbA1c, FBS, PPBS, Insulin |
| Sonkar et al. [ | India | Observational | 200 | T2DM patients (some with DR) | Zinc, selenium, magnesium, chromium | T2DM vs healthy | Trace element levels vs glycemic control and DR presence |
| Ganiger et al. [ | India | Case-control | 150 | T2DM patients with and without DR & healthy controls | Zinc | DR vs non-DR vs healthy | Serum Zn levels and correlation with HbA1c |
| Srikanth [ | India | Case-control | 190 | T2DM patients with and without DR & healthy controls | Magnesium | DR vs non-DR vs controls | Serum Mg levels and correlation with DR |
| Trace element | Author (year) | Key findings | Statistical significance |
| Magnesium | Shivakumar et al. [ | Serum Mg significantly lower in DR group vs. non-DR group | p = 0.029 |
| Kumar et al. [ | Hypomagnesemia group had higher prevalence of NPDR (62.7%) and PDR (21.8%) vs. normal Mg group (14.3% and 8.6%) | p < 0.001 | |
| Xu et al. [ | Serum Mg levels significantly lower in DR group compared to T2DM without complications (T2DCON) | p < 0.01 | |
| Srikanth MP [ | Serum Mg significantly lower in DR group vs. non-DR group | p = 0.022 | |
| Sonkar et al. [ | No direct association between Mg and DR, but deficiency worsened glycemic control | NA | |
| Zinc | Zhu X et al. [ | Zinc levels significantly lower in DR group compared to DM group | p < 0.05 |
| Dascalu et al. [ | Zinc levels lower in DR patients, correlated with poor glycemic control | NA | |
| Miao et al. [ | Zinc deficiency worsens oxidative stress, promotes pericyte apoptosis and retinal neovascularization | NA | |
| Sonkar et al. [ | No direct association between Zn and DR, but deficiency worsened glycemic control | NA | |
| Ganiger A et al. [ | Strong negative correlation between serum zinc and HbA1c in retinopathy cases | p < 0.001 | |
| Manganese | Zhu X et al. [ | Mn levels significantly lower in the DR group compared to the DM group | p < 0.05 |
| Nugrahani et al. [ | MnSOD Ala16Val polymorphism (VV genotype) significantly increased DR risk | p < 0.0001 | |
| Zhang et al. [ | Inverse association between serum Mn levels and DR prevalence; strongest in older men with BMI ≥ 30 | p = 0.015 | |
| Chromium | Alkhalidi et al. [ | Chromium supplementation reduced HbA1c from 10.4% to 7.2% in 3 months | p = 0.001 |
| Ghosh et al. [ | Chromium supplementation improved FBS, PPBS, HbA1c, and insulin sensitivity | p < 0.0001 | |
| Sonkar et al. [ | No direct association between chromium and DR, but deficiency worsened glycemic control | NA | |
| Selenium | Chen X et al. [ | U-shaped relationship between Se and DR; optimal level ≈ 106.8 µg/L | Significant nonlinear association |
| Zhang et al. [ | No association between serum Se levels and DR | p = 0.125 (NS) | |
| Sonkar et al. [ | No direct association between Se and DR, but Se deficiency worsened glycemic control | NA | |
| Iron | Chen et al. [ | Lower serum iron levels significantly associated with higher DR prevalence | p < 0.004 |
| Wang et al. [ | Ferroptosis (iron-driven cell death) linked to retinal neurodegeneration in diabetic rats | Preclinical experimental evidence |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrace Elements in Health · Heavy Metal Exposure and Toxicity · Neurological Disorders and Treatments
Introduction and background
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder characterized by impaired insulin secretion from pancreatic β-cells and reduced insulin sensitivity, leading to persistent hyperglycemia [1]. It is strongly associated with obesity, sedentary lifestyle, and aging, and is perpetuated by complex genetic, environmental, and inflammatory interactions that culminate in insulin resistance and β-cell dysfunction [1,2].
T2DM has emerged as a global public health crisis, with an estimated 463 million adults affected in 2019, projected to rise to 700 million by 2045, a 51% increase [2]. The global prevalence stands at 8.8%, with slightly higher rates in men (9.6%) than women (9.0%), and the burden is disproportionately high in low- and middle-income countries [2,3]. India ranks second only to China, with 77 million cases in 2019, expected to escalate to 134 million by 2045 [2]. Alarmingly, nearly 57% of diabetes cases remain undiagnosed in India, contributing to late detection of complications and higher morbidity [2,4].
Diabetic retinopathy (DR): a growing concern
DR is a leading microvascular complication of diabetes and one of the foremost causes of vision impairment and blindness worldwide, particularly in the working-age population [5]. Chronic hyperglycemia initiates a cascade of biochemical disturbances, including oxidative stress, polyol pathway activation, protein kinase C signalling, and advanced glycation end-product accumulation, resulting in progressive microvascular damage, capillary leakage, neovascularization, and retinal neurodegeneration [3,6].
Globally, approximately 30-40% of individuals with T2DM develop some degree of DR. By 2045, it is projected that 161 million people will have DR, including 45 million with vision-threatening DR (VTDR) [4,5]. In India, a nationally representative survey reported a DR prevalence of 12.5% and VTDR prevalence of 4% among adults with diabetes aged ≥40 years [4,7,8]. This translates to nearly 3 million individuals with VTDR, highlighting the urgent need for improved risk stratification and early intervention strategies.
Emerging Role of Trace Elements in DR
Although chronic hyperglycemia is the principal driver of DR, growing evidence suggests that imbalances in essential trace elements also play a key role in its pathogenesis [9]. Micronutrients such as magnesium, zinc, manganese, chromium, selenium, and iron are crucial cofactors in enzymatic reactions regulating glucose metabolism, insulin signalling, antioxidant defence, and vascular homeostasis [10,11].
Magnesium (Mg): A cofactor in carbohydrate metabolism and insulin receptor function, hypomagnesemia is common in T2DM and linked with insulin resistance, endothelial dysfunction, and DR severity [7,12,13].
Zinc (Zn): Essential for insulin synthesis and antioxidant defense, zinc deficiency is associated with increased oxidative stress, vascular endothelial growth factor (VEGF) upregulation, and progression of DR [14,15].
Manganese (Mn): Required for mitochondrial function and manganese superoxide dismutase (MnSOD) activity, low Mn levels or MnSOD polymorphisms have been linked to higher DR risk [16,17].
Chromium (Cr): It enhances insulin receptor activity and glucose uptake; its deficiency contributes to hyperglycemia and may worsen microvascular complications [8,18,19].
Selenium (Se): Through selenoproteins such as glutathione peroxidase, selenium reduces oxidative stress and supports endothelial health, though a U-shaped association with DR risk has been reported [9,20,21].
Iron (Fe): Both deficiency and dysregulated iron metabolism may promote retinal hypoxia, oxidative injury, and ferroptosis, contributing to neurodegeneration in DR [10,22].
In countries with a high diabetes burden, such as India, regional variations in micronutrient intake and nutritional status may further influence trace element profiles and associated DR risk [23,24].
Rationale for this systematic review
Despite numerous observational studies and some clinical trials, evidence regarding the association between trace elements and DR remains fragmented. Causal relationships are unclear, and optimal supplementation strategies have not been established. Moreover, data on stage-specific associations (mild nonproliferative DR (NPDR) vs. proliferative DR (PDR) and the impact of genetic polymorphisms on trace element metabolism are limited.
Therefore, we conducted a systematic review of published literature to synthesize current evidence on the association of magnesium, zinc, manganese, chromium, selenium, and iron with DR, summarize mechanistic insights, and identify research gaps to guide future interventional studies.
Review
Study design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines.
Research question
The review aimed to evaluate the association of trace elements (zinc, magnesium, copper, selenium, chromium, and others) with the development and progression of DR in patients with diabetes mellitus.
Eligibility criteria
Inclusion Criteria
The inclusion criteria were as follows: studies enrolling adults aged 18 years or older diagnosed with type 1 or T2DM; those assessing serum or plasma levels of trace elements such as zinc, magnesium, copper, selenium, chromium, manganese, and iron; studies including a comparator group of diabetic patients without retinopathy or healthy controls where applicable; studies reporting an association between trace element levels and DR; and observational studies (cross-sectional, case-control, cohort), review articles, and clinical trials published in peer-reviewed journals, in English, between January 2000 and June 2025.
Exclusion Criteria
The exclusion criteria included case reports, letters to the editor, and conference abstracts without full text; studies lacking a comparator group or not reporting quantitative data on trace elements; and animal or in vitro studies.
Search strategy
A comprehensive literature search was conducted in PubMed, Scopus, Web of Science, Cochrane Library, and Google Scholar. The following combination of keywords and Medical Subject Headings (MeSH) was used: (“diabetic retinopathy” OR “DR”) AND (“trace elements” OR “zinc” OR “magnesium” OR “copper” OR “selenium” OR “chromium” OR “manganese” OR “iron”). Boolean operators AND/OR were used to refine results. Reference lists of relevant articles and reviews were manually screened to identify additional eligible studies.
Study selection
Two independent reviewers screened titles and abstracts. Full texts of potentially relevant studies were assessed for eligibility. Discrepancies were resolved by consensus or third-party adjudication.
Data extraction
Data from each included study were extracted into a predesigned MS Excel (Microsoft Corporation, Redmond, Washington, United States) sheet, recording author, year, country, study design, sample size, population characteristics, type of trace element measured, method of assessment, DR grading system used, and key results.
Quality assessment and risk of bias
The methodological quality of included studies was independently assessed by two reviewers using the Joanna Briggs Institute (JBI) critical appraisal tools appropriate for study design (cross-sectional, case-control, or cohort). Randomized controlled trials were evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool. Each study was rated as having low, moderate, or high risk of bias based on criteria such as participant selection, measurement reliability, confounding control, and outcome reporting (Table 1).
Data synthesis
A narrative synthesis was performed, summarizing associations between trace elements and DR across studies. Where possible, trends were reported (e.g., lower zinc/magnesium levels or higher copper levels in DR vs. controls). Due to heterogeneity in study design, populations, and measurement techniques, a meta-analysis was not performed (Figure 1).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagramA total of 540 records were identified from the following databases: PubMed (n = 142), Scopus (n = 118), Embase (n = 96), Web of Science (n = 82), Cochrane Library (n = 54), and Google Scholar (n = 48). After removing 108 duplicate records and 12 records marked ineligible by automation tools, 420 records were screened. Of these, 310 were excluded based on title and abstract screening. A total of 110 reports were sought for retrieval, and 45 were not retrieved. A total of 65 reports were assessed for eligibility, of which 50 were excluded for the following reasons: no comparator group (n = 22), insufficient quantitative data (n = 18), and irretrievable full text (n = 10). Finally, 15 studies were included in the qualitative synthesis
Results
The systematic review collectively evaluated the association between various trace elements and DR. The included studies spanned multiple regions (India, China, the USA, and Europe) and represented diverse study designs, including cross-sectional studies, randomized controlled trials, meta-analyses, and secondary data analyses. Table 2 summarizes the key characteristics of these studies, including population details, study design, and outcomes assessed.
Magnesium
Lower serum magnesium levels were consistently associated with higher prevalence and severity of DR across multiple studies. Kumar et al. [12] reported significantly greater rates of NPDR (62.7%) and proliferative DR (21.8%) among patients with hypomagnesemia compared to those with normal magnesium levels (14.3% and 8.6%, respectively; p < 0.05). Similar results were observed in the studies by Xu et al. [13] and Shivakumar et al. [7], strengthening the evidence that hypomagnesemia may contribute to microvascular complications in diabetes.
Zinc
Zinc deficiency was commonly observed in DR patients. Dascalu et al. [14] demonstrated lower zinc levels in DR cases, particularly in those with poor glycemic control. Experimental data from Miao et al. [15] further support zinc’s protective role, showing that deficiency enhances oxidative stress, pericyte apoptosis, and pathological neovascularization, all of which are key mechanisms in DR progression.
Manganese
Evidence suggests that manganese may play a protective role against DR. Zhang et al. [16], using the National Health and Nutrition Examination Survey (NHANES) data, reported a negative association between serum manganese and DR prevalence, particularly in obese, older men. Additionally, Nugrahani et al. [17] identified a genetic risk factor, MnSOD Ala16Val polymorphism (VV genotype), that increased susceptibility to DR (p < 0.01).
Chromium
Chromium supplementation was shown to improve glycemic parameters and may lower DR risk. Alkhalidi et al. [8] observed a significant reduction in HbA1c levels from 10.4% to 7.2% after three months of chromium supplementation (p < 0.05). Ghosh et al. [19] also reported significant improvements in fasting blood glucose, postprandial glucose, HbA1c, and insulin sensitivity following chromium therapy.
Selenium
The association between selenium and DR appears to follow a U-shaped curve. Chen et al. [9] reported that both selenium deficiency and excess were linked with increased DR prevalence, with an optimal level near 106.8 µg/L. Sonkar et al. [21] found no direct association with DR but noted that selenium deficiency was correlated with poor glycemic control, potentially influencing disease progression indirectly.
Iron
Two studies highlighted the role of iron in DR pathogenesis. Chen et al. [10] demonstrated that lower serum iron levels were independently associated with higher DR prevalence, even after multivariate adjustment. Wang et al. [22] provided experimental evidence linking iron-driven ferroptosis to retinal neurodegeneration in diabetic models, suggesting a possible mechanistic pathway.
Taken together, these findings indicate that dysregulation of trace elements, particularly magnesium, zinc, manganese, chromium, selenium, and iron, plays a significant role in the development and progression of DR. The detailed summary of individual study findings is presented in Table 3.
Discussion
DR remains one of the most significant microvascular complications of diabetes mellitus and a leading cause of vision loss worldwide. The current systematic review synthesizes available evidence on the role of trace elements in the pathogenesis and progression of DR, providing important insights into their potential utility as biomarkers or therapeutic targets. Our review found consistent evidence linking hypomagnesemia with increased risk and severity of DR. Kumar et al. [12] reported that patients with hypomagnesemia exhibited markedly higher prevalence of NPDR and PDR compared to those with normal magnesium levels. These findings were corroborated by Xu et al. [13] and Shivakumar et al. [7], suggesting that magnesium deficiency may exacerbate microvascular dysfunction through mechanisms such as impaired endothelial function, increased oxidative stress, and altered glucose metabolism.
Zinc, another critical micronutrient, was also found to be significantly lower in patients with DR. Dascalu et al. [14] observed that zinc levels inversely correlated with DR severity, particularly in those with poor glycemic control, while Miao et al. [15] demonstrated that zinc deficiency promotes oxidative stress and pericyte apoptosis, processes central to DR pathogenesis. These results underscore zinc’s role as a potent antioxidant and a cofactor for numerous enzymes involved in retinal protection.
The relationship between manganese and DR has been explored less extensively but appears to suggest a protective effect. Zhang et al. [16] reported a negative association between manganese levels and DR prevalence, with the strongest association seen in older men with obesity, possibly reflecting manganese’s role in antioxidant defence through the MnSOD pathway. This is further supported by Nugrahani et al. [17], who showed that the MnSOD Ala16Val polymorphism (VV genotype) increased DR susceptibility, indicating a gene-environment interaction that warrants further exploration.
Chromium supplementation studies showed improvements in glycemic control, with Alkhalidi et al. [8] reporting significant reductions in HbA1c levels, while Ghosh et al. [19] demonstrated improvements in multiple metabolic parameters. Given that poor glycemic control is a key risk factor for DR, chromium’s role in enhancing insulin sensitivity may indirectly reduce DR risk. Selenium displayed a more complex, nonlinear relationship with DR, as reported by Chen et al. [9], who demonstrated a U-shaped curve with both low and high selenium levels associated with increased DR prevalence. This finding highlights the need for maintaining optimal selenium status rather than indiscriminate supplementation. Iron dysregulation was also implicated, with Chen et al. [10] reporting lower serum iron levels in DR patients, while Wang et al. [22] demonstrated that iron-driven ferroptosis may contribute to retinal neurodegeneration in diabetic models, suggesting a potential mechanistic link between iron metabolism and retinal damage.
Despite these important findings, our review has limitations. The majority of included studies were cross-sectional, limiting causal inference. There was heterogeneity in study design, sample size, and methods of trace element measurement, which precluded meta-analysis. Additionally, few interventional studies were available, making it difficult to determine whether correcting trace element deficiencies would translate into clinically meaningful reductions in DR incidence or severity. Future well-designed prospective studies and randomized controlled trials are needed to validate these associations and explore therapeutic implications.
Conclusions
This systematic review highlights the significant association between essential trace elements magnesium, zinc, manganese, chromium, selenium, and iron and the development and progression of DR in patients with T2DM. The evidence suggests that deficiencies in magnesium, zinc, manganese, and chromium, as well as dysregulation of selenium and iron, may contribute to oxidative stress, endothelial dysfunction, and microvascular injury, thereby accelerating retinal damage. These findings underscore the potential of trace element assessment as a cost-effective tool for early risk stratification and targeted preventive interventions, particularly in resource-limited settings with a high diabetes burden, such as India. However, given the heterogeneity of available studies and the predominance of observational designs, further large-scale, prospective studies and randomized controlled trials are warranted to establish causality and clarify whether supplementation or correction of these deficiencies can translate into reduced incidence or severity of DR.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pathophysiology of type 2 diabetes mellitus Int J Mol Sci Galicia-Garcia U Benito-Vicente A Jebari S 62752120203287257010.3390/ijms 21176275 PMC 7503727 · doi ↗ · pubmed ↗
- 2Epidemiology of type 2 diabetes in India Indian J Ophthalmol Pradeepa R Mohan V 293229386920213470872610.4103/ijo.IJO_1627_21PMC 8725109 · doi ↗ · pubmed ↗
- 3Diabetic retinopathy: looking forward to 2030 Front Endocrinol (Lausanne) Tan TE Wong TY 10776691320223669902010.3389/fendo.2022.1077669 PMC 9868457 · doi ↗ · pubmed ↗
- 4Prevalence of diabetic retinopathy in India stratified by known and undiagnosed diabetes, urban-rural locations, and socioeconomic indices: results from the SMART India population-based cross-sectional screening study Lancet Glob Health Raman R Vasconcelos JC Rajalakshmi R 1764177310202210.1016/S 2214-109X(22)00411-936327997 · doi ↗ · pubmed ↗
- 5Prevalence of diabetic retinopahty in India: Results from the National Survey 2015-19Indian J Ophthalmol Vashist P Senjam SS Gupta V 308730946920213470874710.4103/ijo.IJO_1310_21PMC 8725073 · doi ↗ · pubmed ↗
- 6Serum essential trace elements and toxic metals in Chinese diabetic retinopathy patients Medicine (Baltimore) Zhu X Hua R 099202010.1097/MD.0000000000023141 PMC 767660033217819 · doi ↗ · pubmed ↗
- 7Serum magnesium in diabetic retinopathy: the association needs investigation Ther Adv Ophthalmol Shivakumar K Rajalakshmi AR Jha KN Nagarajan S Srinivasan AR Lokesh Maran A 13202110.1177/25158414211056385 PMC 865582734901747 · doi ↗ · pubmed ↗
- 8A comparative study to assess the use of chromium in type 2 diabetes mellitus J Med Life Alkhalidi F 117811821620233802482010.25122/jml-2023-0081 PMC 10652672 · doi ↗ · pubmed ↗