What are the exercise barriers, facilitators and preferences of community-dwelling older adults with heart failure with preserved ejection fraction? A qualitative best fit framework analysis
Faye Forsyth, Peter Hartley, Jonathan Mant, Scott Rowbotham, John Sharpley, Alison Wood, Christi Deaton

TL;DR
This study explores what helps and hinders older adults with heart failure to exercise, using insights from patient and public involvement events.
Contribution
The study identifies specific capability, opportunity, and motivation factors influencing exercise behavior change in heart failure patients.
Findings
Exercise barriers include negative symptoms and lack of self-efficacy in HFpEF patients.
Facilitators include appealing components and adequate support for exercise engagement.
Motivation factors like well-being and goal achievement are crucial for behavior change.
Abstract
To establish, through patient and public involvement (PPI) events, the exercise barriers, facilitators and preferences of people with heart failure with preserved ejection fraction (HFpEF). Qualitative ‘best fit’ framework analysis was used to analyse field notes and transcripts collected during three patient and public involvement meetings and three workshops. The best fit framework was based on the COM-B model of behaviour change, which has identified that Capability, Opportunity and Motivation components are essential for Behaviour change. The Consolidated criteria for Reporting Qualitative research checklist was used to structure the report. Setting and participants: Community dwelling older adults with HFpEF. 24 people with HFpEF (n=16 female, 66%), 2 spouses and 2 people with chronic conditions participated in the PPI meetings and workshops. Multiple exercise-related capability…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
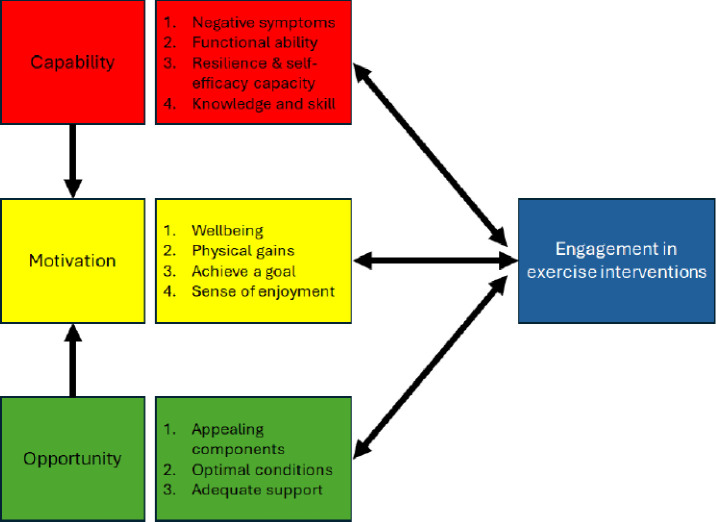 Figure 1
Figure 1| Author±trial name | Sample | Intervention development work and description of patient involvement in design | Description of intervention components | Category | |
|---|---|---|---|---|---|
| Gary | HFpEF | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 12 weeks | ||||
| n=32 | Description | Warm-up, aerobic training in form of walking, cool-down. | |||
| Intensity | 40–60% of maximal heart rate. | ||||
| Wall | Mixed heart failure | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 52 weeks | ||||
| n=19 | Description | Warm-up, aerobic treadmill-based exercise, cool-down. | |||
| Intensity | Guided by symptom severity. | ||||
| Kitzman | HFpEF | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 16 weeks | ||||
| n=53 | Description | Warm-up, aerobic training walking or cycling, cool-down. | |||
| Intensity | 2 weeks at 40–50% of heart rate reserve, increasing to 60–70%. | ||||
| Alves | Mixed heart failure | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 6 months | ||||
| n=98 | Description | Warm-up, treadmill/stationary cycle, cool-down. | |||
| Intensity | 70–75% of maximal heart rate. | ||||
| Smart | HFpEF | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 16 weeks | ||||
| n=98 | Description | Warm-up, aerobic cycle training, cool-down. | |||
| Intensity | 60–70% VO2 peak or respiratory rate <30 breaths/minute. | ||||
| Kitzman | HFpEF | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 16 weeks | ||||
| n=63 | Description | Warm-up, aerobic training (walking or cycling), arm ergometry, cool-down. | |||
| Intensity | 40–50% of heart rate reserve, increasing to 70%. | ||||
| Angadi | HFpEF | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 4 weeks | ||||
| n=15 | Description | Warm-up, 2 min intervals of high intensity interval training, cool-down. | |||
| Intensity | 80–85% of maximal heart rate | ||||
| Fu | Mixed heart failure | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 12 weeks | ||||
| n=129 | Description | Warm-up, aerobic interval training, cool-down. | |||
| Intensity | Intervals at 40% VO2 peak and 80% VO2 peak. | ||||
| Antinocelli | Mixed heart failure | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 50 min classes | ||||
| n=343 | Description | Warm-up, cycle ergometer use, cool-down. | |||
| Intensity | 60–70% of predicted maximal heart rate. | ||||
| Kitzman | HFpEF | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 20 weeks | ||||
| SECRET-II | n=100 | Description | Warm-up, walking exercise, cool-down. | ||
| Intensity | Progressed as tolerated based on heart rate reserve. | ||||
| Donelli da Silveira | HFpEF | Nil described | Frequency | 3× weekly | Aerobic |
| Duration | 12 weeks | ||||
| n=19 | Description | High intensity: warm-up, moderate and high intensity aerobic exercise on treadmill, cool-down. Moderate continuous training: warm-up, moderate-intensity aerobic exercise, cool-down. | |||
| Intensity | High: 80–90% of VO2 peak; moderate: 50–60% of VO2 peak. | ||||
| Lang | HFpEF | Six-step intervention mapping framework that included two systematic reviews. A PPI group (n=6 with ‘a range of heart failure experiences’, n=3 carers) participated in: design of the interview topic guide and the needs assessment survey, summaries of information from the focus groups. | Frequency | Home-based, encouraged regular activity/use of manual. | Aerobic |
| Duration | 12 weeks | ||||
| n=50 | Description | Walking programme or chair-based exercise DVD or combination. | |||
| Intensity | Unclear—tailored to initial fitness assessment. | ||||
| Mueller | HFpEF | Nil described | Frequency | 3× weekly high intensity interval training, 5× weekly moderate continuous training. | Aerobic |
| Duration | 12 months | ||||
| OptimEx-Clin | n=180 | Description | HIIT: warm-up, moderate-intensity cycling, high intensity training intervals with active recovery, cool-down. Moderate-intensity continuous training: warm-up, cycle ergometers, cool-down. | ||
| Intensity | HIIT: 85–95% VO2 peak; moderate-intensity continuous training: 50–60% VO2 peak. | ||||
| Jaarsma | Mixed heart failure | Longitudinal case study of one patient. | Frequency | 5× weekly | Aerobic |
| Duration | 12 months | ||||
| HF-Wii | n=605 | Description | Exergame for 30 min/day | ||
| Intensity | Not described | ||||
| Nilsson | Mixed heart failure | Nil described | Frequency | 2× weekly | Aerobic and resistance |
| Duration | 16 weeks | ||||
| n=80 | Description | Warm-up, aerobic dance movements, resistance training, cool-down. | |||
| Intensity | Aerobic exercises: 15–18 on Borg rating of perceived exertion. | ||||
| Davidson | Mixed heart failure | Nil described | Frequency | 1× week | Aerobic and resistance |
| Duration | 12 weeks | ||||
| n=105 | Description | Warm-up, treadmill/stationary cycle, resistance training, cool-down. | |||
| Intensity | Not described | ||||
| Edelmann | HFpEF | Nil described | Frequency | 2× weekly (week 1–4); 3× weekly (week 5–12) | Aerobic and resistance |
| Duration | 12 weeks | ||||
| Ex-DHF-P | n=64 | Description | Warm-up, cycle-based aerobic endurance training, resistance training, cool-down. | ||
| Intensity | Week 1–4: 50–50% VO2 peak. Week 5–12: 70% VO2 peak. | ||||
| Palau | HFpEF | Nil described | Frequency | 2× daily for 20 min | Inspiratory muscle training |
| Duration | 12 weeks | ||||
| n=26 | Description | Diaphragmatic breathing | |||
| Intensity | At a resistance of 25–30% of maximal inspiratory mouth pressure. | ||||
| Reeves | Mixed heart failure | Nil described | Frequency | 3× weekly | Aerobic, resistance, balance, mobility |
| Duration | 12 weeks | ||||
| REHAB-HF (pilot) | n=27 | Description | Warm-up, balance, mobility, strength and aerobic, cool-down. | ||
| Intensity | 1–2 weeks: <12 on Borg RPE; 13 for endurance and 15–16 for strength training. | ||||
| Kitzman | Mixed heart failure | Pilot trial, | Frequency | 3× weekly | Aerobic, resistance, balance, mobility |
| Duration | 12 weeks | ||||
| REHAB-HF (full trial) | n=349, Mean age=73.1 | Description | Warm-up, balance, mobility, strength and aerobic, cool-down. | ||
| Intensity | 1–2 weeks: <12 on Borg rating of perceived exertion; 13 for endurance and 15–16 for strength training. | ||||
| Alonso | Mixed heart failure | Pilot trial with patients with HFrEF only, | Frequency | Patient directed | Aerobic and resistance |
| Duration | 18 months | ||||
| HEART CAMP | n=204 | Description | Warm-up, moderate-intensity continuous training, resistance training, cool-down. | ||
| Intensity | Continuous training: 40%–80% heart rate reserve. Resistance training: 10–15 repetitions or to fatigue. | ||||
| Brubaker | HFpEF | Previous pilot trials (SECRET-I, | Frequency | 3× weekly | Aerobic and resistance |
| Duration | 70 min | ||||
| SECRET-III | n=77 | Description | Warm up and cool down (stretching, walking), 40 min aerobic training, 20 min resistance training. | ||
| Intensity | Individualised and progressive according to baseline exercise test. | ||||
- —http://dx.doi.org/10.13039/501100004282Evelyn Trust
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Cardiovascular and exercise physiology · Cardiovascular Function and Risk Factors
Introduction
Heart failure with preserved ejection fraction (HFpEF) is defined as symptoms of heart failure within the context of a left ventricular ejection fraction ≥50%, structural remodelling and/or diastolic dysfunction plus abnormal biomarkers.1 In the most recent update of the global burden of heart failure, Shahim et al2 highlighted several studies in Europe and North America which demonstrate that the proportion of people with HFpEF is increasing. In older women, where HFpEF is more common,3 it accounts for approximately 90% of incident heart failure.4 Several factors have been implicated in the rise of cases, including increases in life expectancy, cardiac comorbidities like coronary artery disease and atrial fibrillation and non-cardiac comorbidities like obesity, metabolic disease and diabetes.5
Until recently, there were no positive trials of pharmacological therapies in HFpEF,6 and management advice focused on treating symptoms and comorbid conditions.1 Exercise trials, on the other hand, have a long history of returning favourable results across a broad range of outcomes.7 Indeed, consecutive meta-analyses have demonstrated exercise delivers important gains in cardiorespiratory fitness and quality of life in patients with HFpEF.810 Mean improvement in volume of oxygen uptake during peak exercise (VO_2_ peak) in these reviews ranges from 2.28 to 2.6 mL/min/kg. According to Swank et al11 even modest increases in peak VO_2_ are associated with a favourable outcome. Quality of life improvements from exercise interventions have been more variable. Mean differences in quality of life outcomes between treatment and control arms have ranged from 3.7 points when measured by the Kansas City Cardiomyopathy Questionnaire (not clinically meaningful),12 to 10.9 points (clinically meaningful)13 in studies employing the Minnesota Living with Heart Failure Questionnaire.10 Based on these improvements, exercise training is a Class I recommendation in most national and international guidelines.1 14 15 However, multiple gaps in the evidence base remain, including optimal exercise combinations, doses and patient preferences.7 This research sought to explore patients with HFpEF’s’ preferences for exercise interventions, and thereby address this gap in the evidence base.
Background
Exercise intolerance, the cardinal symptom of HFpEF,1 causes significant distress and difficulties for patients.16 There is consistent evidence that exercise training improves exercise tolerance and functional capacity in patient with heart failure.17 18 However, there is a paucity of exercise trials exclusively targeting HFpEF (table 1). Further, completed trials present limitations in their intervention design.7 18 For example, the variety of exercises and exercise combinations that have been evaluated is limited. 75% of exercise studies with exclusively HFpEF samples (n=12) have tested conventional aerobic exercises. A very small number of studies (n=2) have evaluated multi-component approaches, and there are few examples of high intensity interval training. Although peripheral non-cardiac mechanisms and oxygen pathway defects are postulated to be pathophysiologically potent in HFpEF,19 20 few interventions have assessed alternative types of exercise that have been postulated to better address these causes of exercise intolerance (ie, resistance or inspiratory muscle training).21 There are also problems with small sample sizes (mean n=65), mean age of participants (68 years) and clinical status (limited samples include typical multimorbid and frail participants), which raises questions of the generalisability of the results to older individuals. Real-world samples of people with HFpEF indicate a far greater average age.3 In the UK, the mean age of the community dwelling OPTIMISE HFpEF cohort was 79 years.22 Two contemporary analyses of clinical services indicate a mean age of 80 years23 and 78 years,24 respectively. Younger samples tend to be healthier with a lower comorbidity burden; a previous review of exercise trials in HFpEF has confirmed the relative lack of comorbid conditions in enrolled subjects.8
The mismatch between intervention designs and clinical characteristics of enrolled patients has led some to claim we are ‘fitting a square peg into a round hole’.25 There are also concerns about the lack of consideration of HFpEF phenotypes and social determinants of exercise behaviour within trials. As exercise interventions are by their nature complex, key development steps are necessary to ensure the end design takes into account existing evidence on: (1) mechanisms of exercise intolerance; (2) efficacy of exercise modes in addressing these mechanisms; (3) barriers, facilitators and patients’ preferences for operationalisation of exercise interventions.26 As table 1 demonstrates, few studies have described undertaking any development work or patient involvement work that satisfies these development pre-requisites, prior to testing their intervention. Even in those programmes that have engaged in development work,27 28 there is only one reference to consultation work conducted with people with heart failure and it is unclear whether this sample was comprised of people with HFpEF.27
Aim
The aim of this research was to establish patients with HFpEF patients’ preferences regarding a future exercise intervention.
Methods
For this analysis, we collated field notes and anonymised transcripts from three patient and public involvement (PPI) meetings (n=15 patients with HFpEF, n=2 with other chronic diseases), and three workshops (n=9 patients with HFpEF, n=2 spouses). Qualitative ‘best fit’ framework analysis was undertaken by an experienced qualitative researcher (FF), supported by specialists in HFpEF (CD) and behaviour change (PH).29 The analysis progressed as follows: (1) data sources were imported into NVivo V.12; (2) the best fit framework, based on the COM-B model components, was created within the nodes section; (3) data was coded against the a priori COM-B framework; (4) new themes were created from each node of the framework; (5) the framework, supported by themes and evidence (quotes), formed the basis of this report. Trustworthiness was confirmed by another author (PH) who is familiar with COM-B. They confirmed coded data matched the framework and/or challenged coding decisions; discrepancies were resolved via revisiting the COM-B papers and discussion. Direct quotations have been used to support the theme and framework construct. Pseudonyms have been used and age in decades has been provided to maintain anonymity. Findings are reported in line with the COREQ checklist (Consolidated criteria for Reporting Qualitative research.)30
Sample
Only minimal demographic data (age and sex) were collected as this was a PPI initiative. For workshops, which generated the majority of the data presented, 30 people with a confirmed diagnosis of HFpEF who resided in the East of England were contacted from a completed study, OPTIMISE HFpEF.31 Those who responded positively (n=9 people with HFpEF) were asked to sign an informed consent form and cascade information to interested spouses (n=2). People attending PPI meetings (n=15 HFpEF) included some patients with HFpEF who were invited to become a PPI group member during participation in the OPTIMISE HFpEF cohort study,22 32 supplemented with members of the National Institute for Health and Care Research Cambridge Biomedical Research Centre, PPI panel.33 The latter members (n=2), who had chronic health conditions, had experience of PPI work and were asked to bring this expertise to an otherwise novice PPI group. Meetings and workshops were held in conference style rooms; only workshops were digitally recorded and transcribed verbatim. Meetings and workshops were held between the period 2018 and 2024, meetings lasted 1.5 hours, and workshops were scheduled for 4 hours. All sessions included lunch or refreshments and transportation was arranged; however, there was no reimbursement for time. Rapport had been established via previous participation or regular meetings and communications. Transcripts were not returned to participants for review. There were no topic guides; rather, participants were asked to discuss findings generated from a programme of work seeking to design an optimised diet and exercise intervention in HFpEF163437 and to share their views and suggestions for a future exercise intervention. These findings were presented in PowerPoint format as part of the meetings or workshops, concluding slides had prompts such as ‘what are your views’ and ‘what should we do next’.
Ethical considerations
Ethical approval to recall participants from the OPTIMISE HFpEF study was granted by the London–Surrey Research Ethics Committee (REC reference: 17/LO/2136.) All participants provided informed consent, including before PPI meetings.
Data analysis
Transcripts and field notes were imported into NVivo V.12 software38 for analysis. Qualitative ‘best fit’ framework methods, as described by Dixon-Woods,29 were used. This method was employed as it allows for selection of an a priori conceptual framework, in our case the COM-B model for behaviour change,39 which then serves as an initial starting point for coding. Having (1) moderated and contributed to all of the meetings and workshops, (2) visited the data regularly over a 6-year period to generate reports and presentations and (3) transcribed recordings or made detailed field notes, we were confident the COM-B model was the best fit for the data. The authors of the COM-B model class it as a ‘behavior system’ which involves three interacting conditions necessary for a behaviour to occur: capability, opportunity and motivation (figure 1).39 Within the system, capability is defined as ‘an individual’s psychological and physical capacity to engage in the activity concerned’; motivation as ‘brain processes that energize and direct behaviour’; and opportunity as ‘factors that lie outside the individual that make the behaviour possible or prompt it’. While the authors note that COM-B is a model of behaviour, they stress its utility in designing interventions that intend to change behaviour.39 The latter provides further justification for using the COM-B model as a framework for analysis.
The COM-B behaviour system.
Trustworthiness
Data were coded by one author (FF) and verified by a second author (PH) who co-facilitated the PPI events and who was familiar with the COM-B model through a prior project.40 Verification was performed via triangulation of the transcripts with the coded framework and published descriptions of the COM-B model system.
Results
24 people with HFpEF (n=16 female, 66%, mean age 82 years), 2 spouses and 2 people with chronic conditions participated in this programme of work that included three face-to-face PPI meetings and three workshops. Using the COM-B model of behaviour change, we have identified exercise-related capability, opportunity and motivation conditions that older adults with HFpEF consider essential or preferential to be present, addressed or acknowledged within an intervention designed to elicit behaviour change in this domain. For each COM-B model component, we present a summary of the essential conditions identified and provide quotes in support of these factors. Where multiple factors have been identified, we have prioritised presenting quotes that refer to novel conditions (ie, those not already identified within the HFpEF literature.)
Exercise capability
To elicit behaviour change, any exercise intervention must acknowledge or address key physical capability and psychological capability factors. Physical capability conditions include: (1) functional ability and (2) negative exercise symptoms. Psychological factors comprise: (1) psychological resilience and self-efficacy and (2) knowledge and skill.
Functional ability impacting on capability
According to older adults with HFpEF, functional ability significantly impacts capability to participate in, or attend, exercise interventions. Therefore, this must be accommodated for behaviour change to occur. Age-related deconditioning and post-hospitalisation functional states, which have been identified in previous research,4143 were highlighted as important. Novel functional factors included bodily pain. Sources of pain were numerous; however, it frequently included musculoskeletal pain that resulted from falling, joint replacements, oedema and deconditioning.
I had pain in my feet and legs before, but having fallen and getting the pin in my leg, it is very painful. Rosie, 90+ years, female with HFpEFSo if I’m walking… and I have to take a trolley now, only these last two weeks, because my back’s been so bad… I make sure I have some Paracetamols before.” Arlene, 85+years, female with HFpEF
Negative symptoms associated with or exacerbated by exercise
Negative symptoms associated with or exacerbated by exercise could be actual or anticipated. Common symptoms of HFpEF like breathlessness and fatigue were frequently cited as problems that must be addressed by, or adjusted for, within an exercise intervention. In most cases, participants perceived that behaviour change could not be achieved in the face of these symptoms, as they either prohibited or limited engagement:
I do get breathless when I exercise so I just stop, …I am often breathless. Colleen, 80+years, female with HFpEFI just don’t seem to be able to have the energy or be able to get in the right position to be able to do it [exercise]. Derek, 80+years, male with HFpEF
Exercise-related psychological resilience and self-efficacy
Participants discussed the importance of having or developing psychological resilience and self-efficacy skills to deal with the stressors associated with exercise such as actual or anticipated symptoms and/or anxiety of these. Fatigue and pain were the most frequently referenced psychological stress triggers or barriers. They required implementation of pre-emptive adaptations for practical, safety or coping reasons. Planning for and overcoming these stressors drew heavily on psychological reserves. Psychological capability to overcome fear of falling was also voiced as an important factor that should be addressed within an intervention to enable participation.
I dread it [exercising], because I know my back’s going to play me up, and I wonder how I’m going to walk back, with difficulty, you know….and that is daunting, really. Arlene, 85+years, female with HFpEFPrevious experience of falling does [affect things], it takes away your confidence, so you are really thinking too hard about what you are doing and it is always there. Rosie, 90+years, female with HFpEF
Exercise knowledge and skills
In addition to facilitating psychological resilience, there is the need to provide adequate knowledge and skills to generally exercise correctly and/or to resource patients to exercise safely and effectively in the context of their existing physical capacity issues. Multiple participants were concerned that they may not be performing the exercises in the correct form and/or reported that they could not always follow generic instructions due to problems resulting from pre-existing medical issues.
I think the other thing is when you’re doing it by yourself you might be doing the exercises but you might not be doing them correctly. Martin, 80+years, male with HFpEF
Exercise opportunity factors necessary for behaviour change
For exercise-related behaviour change to occur, or to enhance the chances of it occurring, participants stated that the ‘right’ opportunities needed to be in place. For this group of older adults with HFpEF and multimorbidity, this meant an intervention that had appealing programme components, that was offered in acceptable conditions and that was accompanied by adequate support. It also meant that certain resources had to be in place or offered for these opportunities to be realised.
Appealing programme components
While there was some variability, there was broad consensus among participants that exercise interventions should be enjoyable, fun or social. Those endorsing social programmes preferred group-based exercises. Other programme characteristics deemed essential were content that was: gradually built up; challenging; varied; that could be maintained, extended or routinised into home life; and which had embedded targets and goals.
I do it [exercise]partly because it keeps all the bits of your body moving and partly because it is very social. Maeve, 75+years, female with HFpEF
Optimal programme conditions for exercise
To increase the likelihood of people with HFpEF attending or adhering to an exercise intervention and thus affecting behaviour change, participants suggested optimal programme conditions. These included sessions that were provided at an appropriate time and in a convenient place that was of an adequate size to accommodate freedom of movement and equipment for mobilising. Other conditions that were considered essential were flexibility and an indefinite duration.
As long as it’s not in the evening, because unless it’s in [local area]and I could try and walk, but there again I don’t like to do walking out at nine o’clock at night back home. Arlene, 85+years, female with HFpEF
Adequate support for exercising
Some participants stressed the importance of having knowledgeable instructors whom they trusted and could access for feedback. For others, support to personalise programmes or information to reinforce any new knowledge and skills was essential to drive behaviour change. Adequate support also encompassed provision of resources that would help people with HFpEF realise any opportunities. This included financial and travel support, as well as assistance to alleviate people from care duties.
That [transportation] is for me now problematic, because if I go, costs me £15 there, £15 back….Twice a week, £60 a week. Graham, 85+years, male with HFpEF
Motivations for engaging in an exercise intervention
Participants spoke of their aspiration that an exercise intervention would lead to them feeling better or happier, or that it would result in an increase in general well-being. Specific motivators included regaining physical ability, seeing results or a future result trajectory, achieving a goal, or a sense of achievement/enjoyment.
Well a lot of my exercise is to do with the garden, and I do absolutely enjoy that, because I can see results, so to see a result of some sort, especially if it’s on the plus side, then you’re gaining two-fold, you’ve enjoyed doing it, and then you’ve seen the results. Arlene 85+years, female with HFpEF
Discussion
To our knowledge, this is the first study to prospectively explore what intervention conditions people with HFpEF consider essential to affect behaviour change in the domain of exercise (figure 1). Multiple behaviour change challenges were noted and strategies to address these within any future exercise intervention would be needed. This research has also identified ‘optimal’ conditions which people with HFpEF consider essential to enable exercise-related behaviour change. Reflecting back to the list of exercise interventions summarised in table 1, it would seem that few exercise interventions evaluated to date have undertaken development or PPI work that would help ensure the end intervention is cognisant of the conditions people with HFpEF consider essential for behaviour change. Further, based on our review of their reported outcome measures, it does not appear as though any intervention thus far tested has aimed to assess outcomes that people with HFpEF consider essential (well-being or enjoyment). While we accept that many of these studies were mechanistic or proof of concept, there is sufficient evidence of efficacy to be able to extend research programmes beyond proving exercise has a role in managing HFpEF. Arguably, all interventions should be accompanied by process evaluations, so that we can start to improve intervention design and implementation.
Participants were clear that they had significant functional capacity issues relating to exercise performance and experienced multiple negative symptoms on exercising, that must be accommodated and addressed within an intervention designed to change behaviour patterns. In other words, an intervention that focuses only on delivering a programme of exercise without building in strategies to screen, assess and manage physical inability, pain, breathlessness or fatigue could result in an intervention that people with HFpEF feel incapable of engaging with. There is emerging evidence confirming the importance of distinct mechanisms of exercise intolerance in HFpEF, that are based on phenotypic presentation.44 It is possible that phenotypic evaluation coupled with an assessment of patients’ descriptions of barriers and preferences could be simultaneously undertaken, thus enabling personalised approaches. Participants also stressed the need for knowledge and skills (what, why, how) to exercise safely and effectively and psychological resilience and self-efficacy capacity to overcome psychological barriers like fear, low confidence and anticipated symptoms. Any intervention must address these capability conditions to be effective; however, they must equally be mindful to embed these strategies within the right opportunities to make the execution of a new behaviour possible. In this respect, people with HFpEF have varied opinions of what is ‘right’ for them, be it programme components, conditions of delivery or support. However, there was broad agreement that overall, any exercise intervention should be enjoyable, fun and social. Lastly, interventions must ensure they are tapping into motivators that embed behaviour change, which might be achieved by goal setting and regular reflection or simple well-being scales. Previous research has demonstrated that adherence can be difficult to achieve in heart failure;45 therefore, motivators are of particular importance.
Comparison with other literature
We believe this is the first qualitative report to describe capability, opportunity and motivation conditions for exercise behaviour change, as expressed by people with HFpEF. However, we were able to retrieve one abstract and two reports that offer relevant comparisons. De Wilde et al46 assessed barriers to exercise and self-efficacy using a survey methodology in 60 patients with HFpEF participating in the PRIORITY (PeRsonalIzed remOtely guided preventive exeRcIse therapy for a healThY heart) randomised controlled trial.47 The authors reported that most participants (50%) would not engage with an exercise programme if they perceived it to be boring or not fun; or if they had to exercise alone (40%). They also indicated that a good instructor was essential and that there must be flexibility in a programme to accommodate life events. When they compared different severities of HFpEF (ie, Stage A vs B vs C), they found that those with more severe symptomology (Stage C) were less confident that they could overcome resource and symptom-related barriers to engage in exercise.
Smith et al48 interviewed 15 patients and 7 carers following participation in the REACH-HFpEF intervention, which included a DVD led, chair-based exercise component. They determined that personalised exercise support, goal setting and feedback enhanced engagement, motivation and self-efficacy. Those engaging well reported improved social, emotional and physical outcomes from participation. Concurrent multimorbidity, functional capacity issues and limited perceived gains were reported to reduce or restrict participation. Salahshurian et al49 analysed 67 interviews, conducted longitudinally throughout an exercise intervention (HEART Camp), to establish factors that affected adherence. Important adherence barriers included low functional capacity and negative emotional states. These influenced decisions to continue or cease participation via motivation pathways. Those continuing in the programme reported multiple improvements across a range of domains, not necessarily specific to their heart failure. The interviewers also established critical recommendations that patients with HFpEF would give to other patients embarking on a similar endeavour such as establishing routines, finding ways to make it enjoyable and tracking down the optimal conditions that made exercise easy to action.
There are more reports that have looked at perceptions of exercise,50 exercise influencers,51 exercise barriers and enablers52 and long-term adherence53 in unspecified heart failure or heart failure with reduced ejection fraction (HFrEF). Albert et al50 interviewed 48 patients with HFrEF who took part in the HF-ACTION trial and determined that participants reported a lack of knowledge or access to information and that if accessed, information provided was often not meaningful. They also reported that fear was a driver of action and inaction, life often got in the way of being active and emotions and perceptions of capability played a role in regulating activity. Tierney et al51 interviewed 22 people with presumed HFrEF and reported that cognitive, emotional, interpersonal and environmental factors played a role in willingness to exercise. Within these categories, mental outlook, fluctuating health, environmental influences and others’ expectations were key in enabling or inhibiting engagement in exercise. Warehime et al53 interviewed 22 participants about long-term adherence to an exercise programme. Important adherence enablers identified within interviews included having sufficient knowledge, support from trainers and family and adequate motivation. In the most recent analysis, Amirova et al52 used the Theoretical Domains Framework,39 which complements the COM-B model, to identify perceived barriers and enablers to exercise in patients with HFrEF (n=16). They elicited 39 belief statements about exercise that functioned as barriers of facilitators. Most commonly expressed inhibitors were beliefs about physical ability, low self-efficacy, lack of social support and concern about adverse events. Facilitators included goal setting and action planning. There are multiple overlaps between themes from these investigations and the data presented here, particularly around capacity, knowledge, skills and motivation. However, these studies limit their remit to broad suggestions of how these factors may influence activity. They did not explore how these influencers may be addressed through study design as we have done.
Study limitations
This study is limited by the small sample size and reliance on field notes for some data which may introduce bias. Two participants did not have HFpEF, and were co-opted on the basis of their PPI experience; this may have influenced results. The study is further limited by the lack of data on broader psychosocial and biological factors that may influence exercise engagement. While the sample was representative in terms of established characteristics of HFpEF (older, predominantly female, multimorbid), it is constrained by the fact that participants were recruited from a single site in the East of England. Further bias may be introduced through the use of workshops, which are akin to focus groups in that there is a risk of social acceptability bias. However, the diversity of the responses and the concordance with the breadth of findings from other studies suggests that the risk of social desirability bias is low.
Conclusions
Findings from this study provide insight into capability, opportunity and motivation conditions that are necessary to enable people with HFpEF to change exercise behaviours. This work extends previous research by moving beyond establishing broad influences that may enable or impede behaviour change to identify intervention conditions necessary to affect change. In identifying these conditions, participants have also elucidated potential methods through which these behaviour change conditions can be met. For example, future interventions might wish to offer group classes that build in social components that make the experience fun and enjoyable. Further, this research indicates that additional outcome measures will be needed to capture the type of changes that motivate people with HFpEF to execute behaviour change. These measures could in turn help people with HFpEF reflect on the benefits of performing any new behaviours (which might not be immediately obvious or recalled), thus changing the behaviour from something they must do as part of an intervention, to something they want to do. We know that exercise is efficacious in HFpEF. Ongoing research to identify the optimal modes of exercise, combined with larger explorations of patient preferences and process evaluations of interventions tested, is vital to moving the field forward.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Donagh TA Metra M Adamo M et al ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC Eur J Heart Fail 202124413110.1002/ejhf.233335083827 · doi ↗ · pubmed ↗
- 2Shahim B Kapelios CJ Savarese G et al Global public health burden of heart failure: an updated review Card Fail Rev 2023910.15420/cfr.2023.05PMC 1039842537547123 · doi ↗ · pubmed ↗
- 3Dunlay SM Roger VL Redfield MM Epidemiology of heart failure with preserved ejection fraction Nat Rev Cardiol 20171459160210.1038/nrcardio.2017.6528492288 · doi ↗ · pubmed ↗
- 4Warraich HJ Kitzman DW Whellan DJ et al Physical function, frailty, cognition, depression, and quality of life in hospitalized adults ≥60 years with acute decompensated heart failure with preserved versus reduced ejection fraction Circ Heart Fail 20181110.1161/CIRCHEARTFAILURE.118.005254 PMC 638036030571197 · doi ↗ · pubmed ↗
- 5Oktay AA Rich JD Shah SJ The emerging epidemic of heart failure with preserved ejection fraction Curr Heart Fail Rep 2013104011010.1007/s 11897-013-0155-724078336 PMC 3870014 · doi ↗ · pubmed ↗
- 6Campbell P Rutten FH Lee MM et al Heart failure with preserved ejection fraction: everything the clinician needs to know Lancet 202440310839210.1016/S 0140-6736(23)02756-338367642 · doi ↗ · pubmed ↗
- 7Sachdev V Sharma K Keteyian SJ et al Supervised exercise training for chronic heart failure with preserved ejection fraction: a scientific statement from the American Heart Association and American College of Cardiology Circulation 2023147 e 69971510.1161/CIR.000000000000112236943925 PMC 12019885 · doi ↗ · pubmed ↗
- 8Pandey A Parashar A Kumbhani D et al Exercise training in patients with heart failure and preserved ejection fraction: meta-analysis of randomized control trials Circ Heart Fail 20158334010.1161/CIRCHEARTFAILURE.114.00161525399909 PMC 4792111 · doi ↗ · pubmed ↗