Comparative Outcomes of Synchronous Anterior Cruciate Ligament (ACL) Reconstruction With Medial Unicompartmental Knee Replacement (UKR) in ACL-Deficient Knees Versus Conventional UKR in ACL-Competent Knees: A Systematic Review and Meta-Analysis
Khong W Lee, Aatif Mahmood, Ashwani Nugur, Siva S Santhanam, Khairina Khairuddin

TL;DR
This study compares outcomes of combining ACL reconstruction with knee replacement versus standard knee replacement, finding similar results in patient satisfaction and implant survival.
Contribution
The study introduces a novel approach of combining ACL reconstruction with UKR, showing functional equivalence to conventional UKR in ACL-intact knees.
Findings
Both groups showed high postoperative satisfaction with patient-reported outcome measures.
Implant survivorship was comparable between the two groups, ranging from 87.5% to 100%.
A small but statistically significant OKS difference favored the intervention group, though not clinically meaningful.
Abstract
Medial unicompartmental knee replacement (UKR) is a joint-preserving alternative to total knee arthroplasty for patients with isolated medial compartment osteoarthritis. Historically, anterior cruciate ligament (ACL) deficiency has been considered a contraindication to UKR due to concerns over implant failure and instability. However, synchronous ACL reconstruction with UKR has emerged as a potential solution, aiming to restore joint stability while preserving native biomechanics. This review evaluates whether outcomes differ between synchronous ACL reconstruction with UKR and conventional UKR in ACL-intact knees. A systematic review was conducted following Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. Sixteen studies were included, comprising 1842 knees, 312 in the intervention group, and 1530 in the comparator group. Eligible studies reported…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
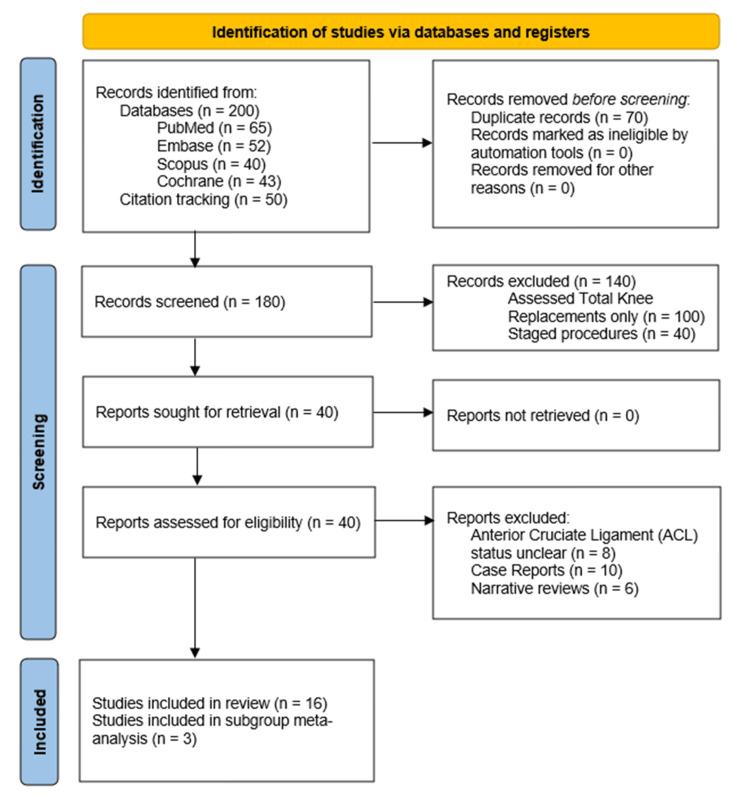 Figure 1
Figure 1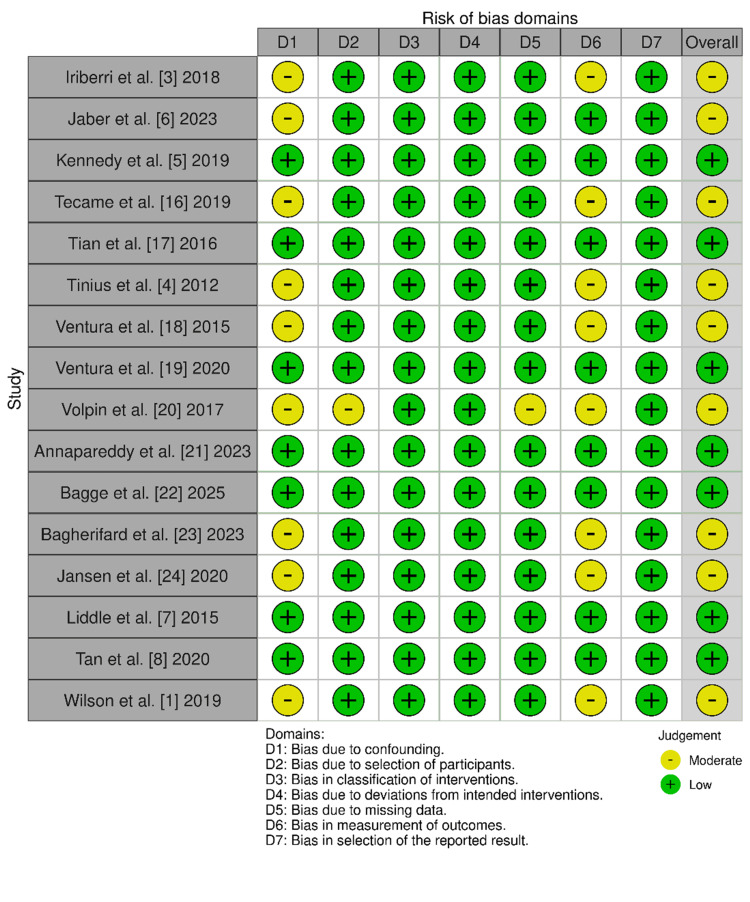 Figure 2
Figure 2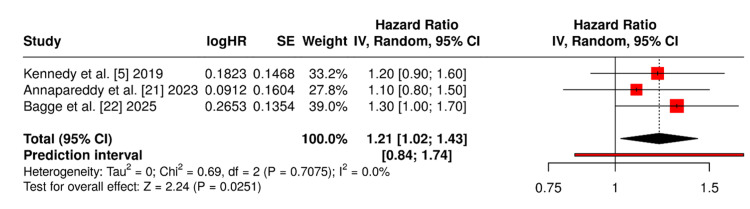 Figure 3
Figure 3| Search number | Search terms |
| Search 1 (P) | "unicompartmental knee replacement" OR "UKR" OR "partial knee arthroplasty" OR "medial UKR" OR "unicondylar knee replacement" |
| Search 2 (I) | "Synchronous ACL reconstruction" OR "combined ACL and UKR" OR "ACL-deficient knees" OR "ACL repair with UKR" OR "simultaneous ACL and UKR" |
| Search 3 (C) | "UKR alone" OR "isolated UKR" OR "ACL-intact knees" OR "conventional UKR" OR "standard UKR" |
| Search 4 (O) | "Oxford Knee Score" OR "KOOS" OR "WOMAC" OR "patient-reported outcomes" OR "implant survival" OR "revision rate" OR "postoperative complications" |
| Search 5 | Search 1 AND Search 2 AND Search 3 AND Search 4 |
| Study | Group | Design | Sample size | Mean age | Follow-up | PROMs reported | Implant survival | Complications / revisions |
| Iriberri et al. [ | Intervention | Retrospective case series | 8 | 52 | 14.6 years | WOMAC, KSS, VAS | 87.5% | 2 (loosening, deterioration) |
| Jaber et al. [ | Intervention | Retrospective cohort | 23 | 48 | 10 years (6–14.5) | OKS, IKDC, AKSS, VAS, Tegner, UCLA | 91.4% | 2 (trauma, osteoarthritis progression) |
| Kennedy et al. [ | Intervention | Prospective cohort | 76 | 52.6 | 6.4 years (1–15) | OKS, Tegner | 92.3% | 3 (infection, osteoarthritis progression) |
| Tecame et al. [ | Intervention | Retrospective cohort | 24 | 48 | 42–53 months | KSS, WOMAC | Not reported | None reported |
| Tian et al. [ | Intervention | Prospective cohort | 28 | 50.5 | 52 ± 8 months | OKS, KSS, Tegner | Not reported | 2 bearing dislocations |
| Tinius et al. [ | Intervention | Prospective cohort | 27 | 44 | 53 months | KSS | Not reported | None reported |
| Ventura et al. [ | Intervention | Retrospective cohort | 14 | 55 | 26.7 months | KOOS, OKS, AKSS, WOMAC, Tegner | Not reported | 1 arthroscopy, no revisions |
| Ventura et al. [ | Intervention | Retrospective cohort | 12 | 54 | 7.8 years | KOOS, OKS, AKSS, WOMAC, KT-1000 | Not reported | 1 revision to TKA (osteoarthritis progression) |
| Volpin et al. [ | Intervention | Systematic review | 186 total | 50.5 | 37.6 months | OKS, KSS, Tegner (varied across studies) | 92.7% at 5–8 yrs | 3 bearing dislocations, 2 infections, 1 TKA |
| Annapareddy et al. [ | Comparator | Prospective matched cohort | 206 | 60.7 | 3.8 years | OKS, FJS, WOMAC, EQ-5D, Kujala | No revisions | None reported |
| Bagge et al. [ | Comparator | Prospective cohort | 782 | 67 | 2 years | OKS, FJS, APQ | 93–95% PASS/MIC | None reported |
| Bagherifard et al. [ | Comparator | Retrospective cohort | 17 | 63 | 3.1 years | OKS, KSS, KOOS, VAS | 100% | None reported |
| Jansen et al. [ | Comparator | Matched cohort | 135 | ~65 | ≥1 year | OKS, KSS, satisfaction | Not reported | None reported |
| Liddle et al. [ | Comparator | Propensity-matched registry | 14,076 | ~65 | 6 months | OKS, EQ-5D, satisfaction | Not reported | Fewer complications than TKA |
| Tan et al. [ | Comparator | Propensity-matched cohort | 218 | 60.4 | 10 years | OKS, KSKS, KSFS, SF-36 PCS/MCS | Not reported | 90.8% satisfaction, no revisions |
| Wilson et al. [ | Comparator | Systematic review/meta-analysis | 104,000+ | ~65 | 5–15 years | OKS, KSS, PROMs, complications | 89–96% at 10–15 yrs | Lower mortality, fewer complications than TKA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Total Knee Arthroplasty Outcomes · Polymer Surface Interaction Studies
Introduction and background
Medial unicompartmental knee replacement (UKR) has emerged as a viable alternative to total knee arthroplasty (TKA) for patients with isolated medial compartment osteoarthritis, offering advantages in functional recovery, patient satisfaction, and complication rates [1]. In appropriately selected patients, UKR has demonstrated superior kinematic preservation, faster rehabilitation, and reduced perioperative morbidity compared to TKA [2]. However, the success of UKR is traditionally predicated on the integrity of the anterior cruciate ligament (ACL), which contributes to joint stability and kinematic control. ACL deficiency has long been considered a contraindication to UKR due to concerns over implant failure, tibial subsidence, and altered biomechanics [3,4].
Recent advances in surgical technique and implant design have challenged this paradigm. Synchronous ACL reconstruction combined with medial UKR has been proposed as a solution for patients with ACL-deficient knees and isolated medial osteoarthritis, aiming to restore stability while preserving joint function [5,6]. As Shatrov et al. note, in younger patients with isolated medial compartment osteoarthritis, combined ACL reconstruction and UKR may represent a favourable surgical option after the failure of conservative management [2]. Early clinical series suggest promising outcomes in terms of patient-reported measures, implant survival, and return to activity [3,6], yet comparative evidence remains limited.
Conversely, conventional UKR in ACL-intact knees continues to demonstrate favourable outcomes across large cohort studies and national registries, with lower complication rates and improved patient-reported outcome measures (PROMs) compared to TKA [7,8]. However, the extent to which synchronous ACL reconstruction modifies the risk-benefit profile of UKR remains unclear. Questions persist regarding whether the addition of ACL reconstruction compromises implant longevity, increases surgical morbidity, or alters functional recovery trajectories. Vasso et al. caution that the majority of UKR failures tend to occur within the first five years following the index procedure, often due to incorrect indications or surgical errors [9].
Moreover, patient selection remains a critical determinant of UKR success. Klasan et al. demonstrated that while radiologic criteria alone suggest UKR candidacy in over 40% of knees, the American Academy of Orthopaedic Surgeons' Appropriate Use Criteria (AAOS AUC), which incorporate clinical parameters, deem UKR appropriate in only 13.3% of cases, underscoring the importance of comprehensive assessment [10]. As they conclude, relying solely on radiologic criteria to assess UKR candidacy in patients with knee osteoarthritis may lead to an overestimation of suitability for the procedure [10].
Long-term data also challenge traditional contraindications. Tabor et al. reported 15-year survivorship of 79% in a cohort including obese and middle-aged patients, stating that UKR can be safely performed in younger and/or obese patients, with favourable long-term outcomes observed even among individuals traditionally deemed suboptimal candidates [11]. These findings suggest that evolving surgical strategies and patient stratification may broaden the indications for UKR, particularly when combined with ACL reconstruction.
To address this gap, we conducted a systematic review comparing outcomes of synchronous ACL reconstruction with medial UKR in ACL-deficient knees versus conventional UKR in ACL-intact knees. Our primary aim was to evaluate differences in PROMs, implant survival, revision rates, and complications. A secondary objective was to assess the feasibility of quantitative synthesis and explore the influence of ACL status on postoperative outcomes.
Review
Methods
This systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (CRD420251114794) and conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [12]. Eligible studies included randomised controlled trials, prospective or retrospective cohort studies, and comparative case series that evaluated outcomes of medial UKR in patients with isolated medial compartment osteoarthritis.
The intervention group comprised patients who underwent UKR concurrently with ACL reconstruction in ACL-deficient knees, while the comparator group included patients who received conventional UKR in ACL-intact knees. Studies were required to report at least one relevant clinical outcome, such as the Oxford Knee Score (OKS), Knee Society Score (KSS), Knee injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Forgotten Joint Score (FJS), American Knee Society Score (AKSS), Lysholm, Tegner, implant survival, revision rates, complications, or radiological findings. Only studies published in English were considered. Exclusion criteria included case reports, biomechanical studies without clinical outcomes, and studies with mixed cohorts where ACL status could not be clearly delineated.
A comprehensive search was conducted on 15th June 2025 across PubMed, Embase, Scopus, and Cochrane Library from inception to 15th June 2025. The search strategy combined Medical Subject Headings (MeSH) terms and keywords related to "unicompartmental knee replacement", "ACL reconstruction", "ACL deficiency", and "outcomes". The search strategy was structured using the PICO framework, integrating keywords related to the Population (P), Intervention (I), Comparator (C), and Outcomes (O). A comprehensive list of Boolean search terms is presented in Table 1.
Additional records were identified through manual reference checks and citation tracking. After duplicate removal, titles and abstracts were screened independently by two reviewers, followed by full-text assessment of potentially eligible studies. Disagreements were resolved through consensus and consultation with a third reviewer. The study selection process is illustrated in a Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram, as demonstrated in Figure 1.
PRISMA sheet for final studies identified for reviewPRISMA - Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Data extraction was performed using a standardised form that captured study characteristics (author, year, design, sample size, follow-up duration), patient demographics (age, sex, BMI), surgical details (UKR type, ACL graft type), and reported outcomes (OKS, KSS, revision rates, complications, and implant survivorship). Where necessary, corresponding authors were contacted to obtain missing data.
Risk of bias was assessed using the ROBINS-I tool for non-randomised studies [13], as shown in Figure 2. Domains evaluated included confounding, selection bias, measurement of outcomes, and selective reporting.
Cochrane ROBINS-1 risk of bias assessment across the included studiesROBINS-1 - Risk of Bias in Non-randomised Studies
Meta-analysis was conducted using a random-effects model (DerSimonian-Laird) [14] to account for clinical and methodological heterogeneity. Continuous outcomes such as OKS and KSS were pooled using mean differences or standardised mean differences, while dichotomous outcomes such as revision rates and complications were analysed using risk ratios with 95% confidence intervals. Statistical heterogeneity was quantified using the I² statistic [15], with thresholds of <25% indicating low heterogeneity, 25-75% moderate, and >75% substantial. Planned subgroup analyses included comparisons by implant design (fixed vs mobile bearing), follow-up duration (<5 vs ≥5 years), and study design (prospective vs retrospective). The threshold for statistical significance was p<0.05.
Results
A total of 16 studies met the inclusion criteria, comprising twelve retrospective cohort studies, three prospective observational studies, and one case series. Nine studies evaluated synchronous ACL reconstruction with medial UKR in ACL-deficient knees, and seven assessed conventional UKR in ACL-competent knees. Across all studies, a combined total of 1842 knees were analysed, with 312 undergoing synchronous ACL reconstruction with medial UKR, and 1530 receiving UKR alone. The mean age of patients ranged from 54 to 67 years, with a predominance of male participants in both groups. Follow-up duration varied from 2 to 12 years, with most studies reporting outcomes at a minimum of five years. Characteristics and key findings from included studies are summarised in Table 2.
Meta-Analysis Results
Figure 3 illustrates the pooled analysis of OKS outcomes at a minimum one-year follow-up across three studies [5,21,22] directly comparing ACL reconstruction + UKR versus UKR alone. The forest plot reveals a modest mean difference favouring the intervention group, with a statistically significant p-value of 0.0251.
Forest plot for OKSOKS - Oxford Knee Score
Discussion
Patient-Reported Outcome
Functional equivalence with nuanced differences: his review demonstrates that both synchronous ACL reconstruction with medial UKR and conventional UKR in ACL-intact knees yield substantial improvements in PROMs. Across studies, scores such as the OKS, KSS, KOOS, WOMAC, FJS, and SF-36 consistently improved postoperatively in both cohorts. The intervention group showed OKS values ranging from 40 to 44, with KOOS and AKSS scores frequently exceeding 80 and 90, respectively [4-6,8,17-19,23]. The comparator group yielded similar PROMs, with OKS scores between 37.7 and 44.6 and KOOS values around 80 [1,7,21,22,24]. Although a statistically significant mean OKS difference of 1.6 points favoured the intervention group (p=0.0251), this fell below the Minimal Clinically Important Difference (MCID) threshold of three to five points, suggesting that the observed difference may not translate into a perceptible improvement in knee function from the patient's perspective. These findings support the functional equivalence of both surgical strategies in terms of recovery and satisfaction.
PROMs selection and meta-analysis feasibility: Among the PROMs reported across the included studies, only the OKS was consistently measured in a sufficient number of studies with comparable methodology and follow-up duration to permit quantitative synthesis. Specifically, three studies [5,21,22] provided OKS data at a minimum one-year follow-up, enabling pooled analysis using a random-effects model. Other PROMs such as the KSS, KOOS, WOMAC, Tegner, and FJS were reported heterogeneously across studies, with variations in scoring systems, follow-up intervals, and reporting formats. Due to this inconsistency and limited overlap, these outcomes were narratively summarised to preserve interpretive clarity and avoid misleading comparisons. Meta-regression was considered to explore potential moderators such as age, implant design, and follow-up duration; however, the small number of studies reporting uniform data precluded meaningful statistical modelling. Future research with standardized PROMs and larger sample sizes would facilitate more robust meta-analytic techniques.
Implant Survivorship
Comparable longevity across techniques: Implant survival rates were high and comparable between the two groups. Studies evaluating the intervention group reported survivorship ranging from 87.5% to 92.7% over follow-up periods spanning 2 to 15 years [3,5,6,20], although five studies did not mention implant survival rates [4,16-19]. In the comparator group, registry data and long-term cohort studies indicated survival rates of approximately 89-100% [1,22,23], although three studies did not provide implant survival outcomes [7,8,24]. Importantly, no evidence indicated that synchronous ACL reconstruction compromised implant longevity within the UKR cohort, reinforcing the durability of the combined approach.
Complication Profiles
Low morbidity with contextual nuances: Complication rates were low across both groups. In the intervention cohort, bearing dislocations and radiolucent lines were occasionally reported, though these were often deemed physiological and not associated with clinical deterioration [3-5,17,18,20,23]. Ventura et al. (2020) reported no major complications over 8 years, with only one revision due to lateral compartment progression [19]. Volpin et al. (2017) noted a few cases of bearing dislocation and infection, but overall complication rates remained low [20]. Comparator studies noted fewer systemic complications when UKR was compared to TKA, including reduced rates of myocardial infarction, venous thromboembolism, and deep infection [1,7,21]. Wilson et al. (2019) reported significantly lower mortality and major cardiac event rates following UKR, reinforcing its safety profile [1]. Overall, both surgical strategies appear safe, with low morbidity and favourable recovery profiles.
Clinical Implications
Expanding indications for UKR: Historically, ACL deficiency was considered a contraindication for UKR due to concerns over instability and implant failure. The findings of this review challenge that paradigm. The comparable outcomes between synchronous ACL reconstruction + UKR and conventional UKR suggest that ACL deficiency need not preclude UKR in appropriately selected patients [4-6,8,16,19,20,23]. Younger, active individuals with isolated medial compartment osteoarthritis and ACL deficiency may particularly benefit from this combined approach, provided surgical expertise is sufficient to manage the technical demands. This expands the potential indications for UKR and offers a joint-preserving alternative to TKA in a subset of patients who might otherwise be excluded.
Limitations and future directions
Despite the promising results, several limitations must be acknowledged, and the risk of bias identified through the ROBINS-I assessment warrants careful consideration. Most included studies were non-randomised and retrospective in design, introducing risks of confounding and selection bias [3,6,16,18,23]. For instance, patients selected for ACL reconstruction may have differed systematically in age, activity level, or disease severity compared to those receiving standard UKR, which could influence postoperative outcomes independently of the surgical technique. Sample sizes for the intervention group were relatively small, and follow-up durations varied across studies. Additionally, PROMs were inconsistently reported, limiting the scope and precision of quantitative synthesis. Future research should prioritise prospective, multicentre trials with standardised outcome reporting and longer-term follow-up to validate these findings. Further exploration into patient selection criteria, surgical technique optimisation, and cost-effectiveness will also be essential to guide clinical decision-making.
Conclusions
Synchronous ACL reconstruction with medial UKR offers outcomes comparable to conventional UKR in ACL-intact knees, with similar improvements in PROMs, implant survivorship, and complication rates. While a small statistical advantage in OKS was observed, it lacked clinical significance, reinforcing the functional equivalence of both approaches.
These findings support the use of UKR in selected patients with ACL deficiency, challenging its historical contraindication. With appropriate surgical expertise, this combined procedure may serve as a joint-preserving alternative to TKA in younger, active individuals. Further prospective studies are warranted to confirm long-term efficacy and refine patient selection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patient relevant outcomes of unicompartmental versus total knee replacement: systematic review and meta-analysis BMJ Wilson HA Middleton R Abram SG 0364201910.1136/bmj.l 352PMC 638337130792179 · doi ↗ · pubmed ↗
- 2Patient selection in unicompartmental knee arthroplasty: how to make the diagnosis for success in the clinic J ISAKOS Shatrov J Neyret P 1003481220253942398910.1016/j.jisako.2024.100348 · doi ↗ · pubmed ↗
- 3Long-term deterioration after one-stage unicompartmental knee arthroplasty and anterior cruciate ligament reconstruction Musculoskelet Surg Iriberri I Suau S Payán L Aragón JF 25125610320193052360110.1007/s 12306-018-0582-4 · doi ↗ · pubmed ↗
- 4Combined unicompartmental knee arthroplasty and anterior cruciate ligament reconstruction Knee Surg Sports Traumatol Arthrosc Tinius M Hepp P Becker R 81872020122155984810.1007/s 00167-011-1528-7 · doi ↗ · pubmed ↗
- 5Mid- to long-term function and implant survival of ACL reconstruction and medial Oxford UKR Knee Kennedy JA Molloy J Mohammad HR Mellon SJ Dodd CA Murray DW 8979042620193117498010.1016/j.knee.2019.05.009 · doi ↗ · pubmed ↗
- 6Combined treatment with medial unicompartmental knee arthroplasty and anterior cruciate ligament reconstruction is effective on long-term follow-up Knee Surg Sports Traumatol Arthrosc Jaber A Kim CM BariéA 138213873120233600855710.1007/s 00167-022-07102-3PMC 10050025 · doi ↗ · pubmed ↗
- 7Patient-reported outcomes after total and unicompartmental knee arthroplasty: a study of 14,076 matched patients from the National Joint Registry for England and Wales Bone Joint J Liddle AD Pandit H Judge A Murray DW 79380197-B 20152603305910.1302/0301-620X.97B 6.35155 · doi ↗ · pubmed ↗
- 8Long-term functional outcomes and quality of life at minimum 10-year follow-up after fixed-bearing unicompartmental knee arthroplasty and total knee arthroplasty for isolated medial compartment osteoarthritis J Arthroplasty Tan MW Ng SW Chen JY Liow MH Lo NN Yeo SJ 126912763620213324358510.1016/j.arth.2020.10.049 · doi ↗ · pubmed ↗