The Association Between Women's Perception of Birth During the Pandemic, Companion of Choice and Support From Health Professionals: A Cross‐Sectional Study in 20 Countries in the WHO European Region
Stephanie Batram‐Zantvoort, Céline Miani, Ilaria Mariani, Emanuelle Pessa Valente, Mehreen Zaigham, Ingvild Hersoug Nedberg, Magdalena Kurbanović, Elizabete Pumpure, Anja Bohinec, Antigone Sarantaki, Barbara Baranowska, Alessia Abderhalden‐Zellweger, Elise de La Rochebrochard

TL;DR
This study shows that having a chosen companion and good professional support during childbirth improves women's birth experiences, even during the pandemic.
Contribution
The study identifies specific factors linked to positive birth perceptions during the pandemic in the WHO European Region.
Findings
Having a companion of choice during birth was strongly associated with a positive perception of the birth experience.
Adequate attention, assistance, and availability from health professionals significantly improved birth perception.
Medical interventions like cesarean births and episiotomies were linked to less positive birth perceptions.
Abstract
Mitigation measures implemented in response to the COVID‐19 pandemic led to significant changes in maternity care across Europe, including restrictions on companions during labor and birth. This cross‐sectional study explores the association between the presence of a companion of choice and a positive perception of the birth experience. Additionally, it explores the association between health professionals' attention, assistance, and availability during labor and birth and a positive perception of birth. We utilized a structured, validated online questionnaire, available in 25 languages, to assess the quality of maternal care during the COVID‐19 pandemic from women's perspectives. We conducted logistic regression to explore associations between variables related to the presence of a companion of choice, health professionals' attention, assistance, and availability, and positive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
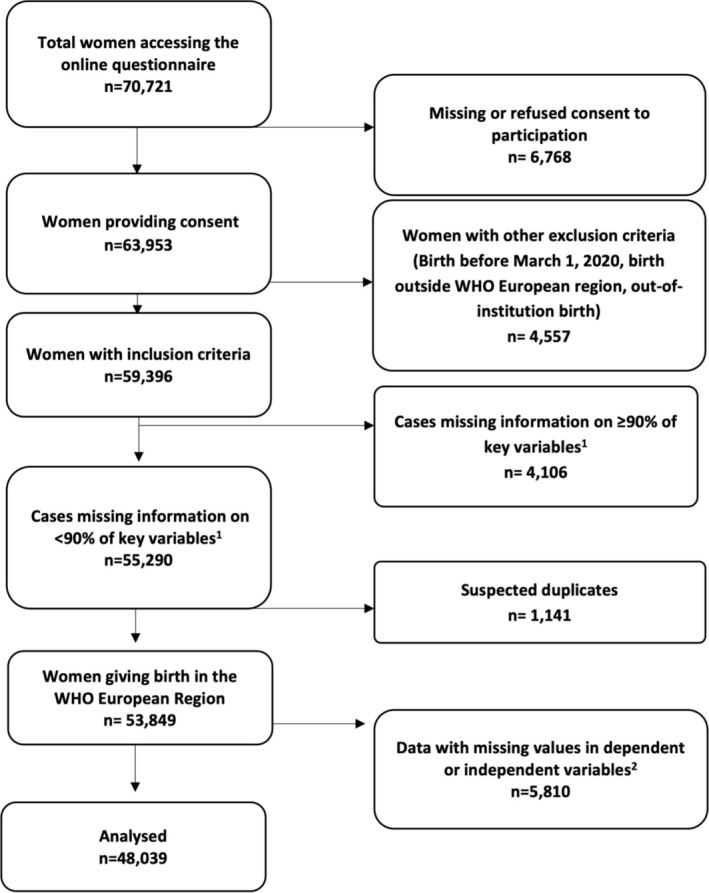 FIGURE 1
FIGURE 1| Overall | |
|---|---|
|
| |
| Parity | |
| Primiparous | 29,275 (60.9%) |
| Multiparous | 18,764 (39.1%) |
| Health professional(s) present | |
| Midwife | 42,700 (88.9%) |
| Nurse | 18,071 (37.6%) |
| Student | 6945 (14.5%) |
| Obstetrician, medical doctor, or medical resident | 30,073 (62.6%) |
| Woman gave birth in the same country where she was born | |
| Yes | 44,445 (92.5%) |
| No | 3594 (7.5%) |
| Educational level | |
| Junior high school or lower | 2589 (5.4%) |
| High school | 11,034 (23%) |
| University degree | 19,531 (40.7%) |
| Postgraduate/master/doctorate | 14,885 (31%) |
| Age | |
| 18–24 | 2389 (5%) |
| 25–30 | 16,544 (34.4%) |
| 31–35 | 19,264 (40.1%) |
| 36–39 | 7562 (15.7%) |
| > 40 | 2280 (4.7%) |
| Country | |
| Austria | 406 (0.8%) |
| Bosnia‐Herzegovina | 560 (1.2%) |
| Croatia | 3241 (6.7%) |
| France | 1410 (2.9%) |
| Greece | 2214 (4.6%) |
| Germany | 1300 (2.7%) |
| Italy | 10,130 (21.1%) |
| Latvia | 3220 (6.7%) |
| Lithuania | 1196 (2.5%) |
| Luxembourg | 515 (1.1%) |
| Norway | 5441 (11.3%) |
| Poland | 1866 (3.9%) |
| Portugal | 1400 (2.9%) |
| Romania | 1265 (2.6%) |
| Serbia | 1102 (2.3%) |
| Slovenia | 2558 (5.3%) |
| Spain | 355 (0.7%) |
| Sweden | 7729 (16.1%) |
| Switzerland | 1416 (2.9%) |
| Other | 715 (1.5%) |
| Overall | Dignified care | Emotional support | Involvement in decision‐making | Abuse | Effective communication | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Always | Sometimes | Never | Always | Sometimes | Never | Always | Sometimes | Never | Always | Sometimes | Never | Always | Sometimes | Never | ||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
| By mode of birth and medical interventions | ||||||||||||||||
| Vaginal birth | 23,863 (49.7%) | 18,932 (54.0%) | 4221 (39.8%) | 710 (30.4%) | 18,154 (55.1%) | 4084 (41.2%) | 1625 (31.6%) | 16,136 (56.3%) | 5560 (43.2%) | 2167 (33.4%) | 415 (33.3%) | 2198 (36.9%) | 21,250 (52.0%) | 17,373 (54.1%) | 5464 (42.2%) | 1026 (34.6%) |
| Vaginal birth with episiotomy | 7781 (16.2%) | 5210 (14.8%) | 2029 (19.1%) | 542 (23.2%) | 4783 (14.5%) | 1852 (18.7%) | 1146 (22.3%) | 3905 (13.6%) | 2364 (18.4%) | 1512 (23.3%) | 276 (22.1%) | 1193 (20.0%) | 6312 (15.5%) | 4690 (14.6%) | 2425 (18.7%) | 666 (22.4%) |
| Instrumental vaginal birth | 2141 (4.5%) | 1574 (4.5%) | 476 (4.5%) |
91 (3.9%) | 1490 (4.5%) | 470 (4.7%) |
181 (3.5%) |
1300 (4.5%) |
615 (4.8%) |
226 (3.5%) |
59 (4.7%) |
288 (4.8%) | 1794 (4.4%) | 1411 (4.4%) | 608 (4.7%) | 122 (4.1%) |
| Instrumental vaginal birth with fundal pressure | 1706 (3.6%) | 1046 (3.0%) | 510 (4.8%) | 150 (6.4%) | 932 (2.8%) | 455 (4.6%) |
319 (6.2%) |
802 (2.8%) |
585 (4.5%) |
319 (4.9%) |
88 (7.1%) |
336 (5.6%) | 1282 (3.1%) | 983 (3.1%) | 571 (4.4%) | 152 (5.1%) |
| Planned cesarean birth | 5192 (10.8%) | 3722 (10.6%) | 1210 (11.4%) | 260 (11.1%) | 3592 (10.9%) | 1049 (10.6%) |
551 (10.7%) |
2951 (10.3%) | 1394 (10.8%) |
847 (13.0%) |
112 (9.0%) |
604 (10.1%) | 4476 (11.0%) | 3406 (10.6%) | 1468 (11.3%) | 318 (10.7%) |
| Unplanned cesarean birth before the onset of labor | 2475 (5.2%) | 1653 (4.7%) | 658 (6.2%) | 164 (7.0%) | 1488 (4.5%) | 599 (6.0%) |
388 (7.5%) |
1220 (4.3%) |
743 (5.8%) |
512 (7.9%) |
75 (6.0%) |
371 (6.2%) | 2029 (5.0%) | 1492 (4.6%) | 782 (6.0%) | 201 (6.8%) |
| Unplanned cesarean birth, after the onset of labor | 4881 (10.2%) | 2952 (8.4%) | 1510 (14.2%) | 419 (17.9%) | 2533 (7.7%) | 1409 (14.2%) |
939 (18.2%) |
2354 (8.2%) | 1613 (12.5%) |
914 (14.1%) |
222 (17.8%) |
974 (16.3%) | 3685 (9.0%) | 2753 (8.6%) | 1644 (12.7%) | 484 (16.3%) |
| Immediate Attention from health professional | ||||||||||||||||
| Always | 32,295 (67.2%) | 28,865 (82.3%) | 3275 (30.9%) | 155 (6.6%) | 26,217 (79.5%) | 4927 (49.7%) | 1151 (22.4%) | 24,482 (85.4%) | 6275 (48.7%) |
1538 (23.7%) |
242 (19.4%) |
1849 (31%) | 30,204 (74%) | 28,107 (87.5%) | 4031 (31.1%) | 157 (5.3%) |
| Sometimes | 12,721 (26.5%) | 5819 (16.6%) | 5961 (56.2%) | 941 (40.3%) | 5969 (18.1%) | 4192 (42.3%) | 2560 (49.7%) |
3902 (13.6%) | 5662 (44%) |
3157 (48.6%) |
465 (37.3%) |
2970 (49.8%) | 9286 (22.7%) | 3783 (11.8%) | 7705 (59.4%) | 1233 (41.5%) |
| Never | 3023 (6.3%) | 405 (1.2%) | 1378 (13.0%) | 1240 (53.1%) | 786 (2.4%) | 799 (8.1%) | 1438 (27.9%) |
284 (1.0%) |
937 (7.3%) |
1802 (27.7%) |
540 (43.3%) |
1145 (19.2%) | 1338 (3.3%) |
218 (0.7%) | 1226 (9.5%) | 1579 (53.2%) |
| Birth companion of choice | ||||||||||||||||
| Always | 19,988 (41.6%) | 17,338 (49.4%) | 2399 (22.6%) | 251 (10.7%) | 16,072 (48.7%) | 3008 (30.3%) |
908 (17.6%) | 14,364 (50.1%) | 4353 (33.8%) |
1271 (19.6%) |
285 (22.9%) |
1515 (25.4%) | 18,188 (44.5%) | 15,688 (48.9%) | 3796 (29.3%) | 504 (17.0%) |
| Sometimes | 7341 (15.3%) | 5650 (16.1%) | 1464 (13.8%) | 227 (9.7%) | 5293 (16.1%) | 1481 (14.9%) |
567 (11.0%) |
4673 (16.3%) | 1941 (15.1%) |
727 (11.2%) |
145 (11.6%) |
841 (14.1%) | 6355 (15.6%) | 5176 (16.1%) | 1821 (14.0%) | 344 (11.6%) |
| Never | 20,710 (43.1%) | 12,101 (34.5%) | 6751 (63.6%) | 1858 (79.5%) | 11,607 (35.2%) | 5429 (54.7%) | 3674 (71.4%) | 9631 (33.6%) | 6580 (51.1%) | 4499 (69.2%) | 817 (65.5%) | 3608 (60.5%) | 16,285 (39.9%) | 11,244 (35.0%) | 7345 (56.7%) | 2121 (71.4%) |
| Adequate assistance by health professional | ||||||||||||||||
| Always | 19,861 (41.3%) | 17,969 (51.2%) | 1737 (16.4%) | 155 (6.6%) | 16,593 (50.3%) | 2570 (25.9%) |
698 (13.6%) | 15,586 (54.4%) | 3364 (26.1%) |
911 (14.0%) |
205 (16.4%) |
1100 (18.4%) | 18,556 (45.4%) | 17,266 (53.8%) | 2387 (18.4%) |
208 (7.0%) |
| Sometimes | 17,618 (36.7%) | 12,251 (34.9%) | 4646 (43.8%) | 721 (30.9%) | 11,157 (33.8%) | 4358 (43.9%) | 2103 (40.8%) |
9438 (32.9%) | 5628 (43.7%) |
2552 (39.3%) |
415 (33.3%) |
2386 (40.0%) | 14,817 (36.3%) | 10,992 (34.2%) | 5723 (44.2%) | 903 (30.4%) |
| Never | 10,560 (22.0%) | 4869 (13.9%) | 4231 (39.9%) | 1460 (62.5%) | 5222 (15.8%) | 2990 (30.1%) | 2348 (45.6%) |
3644 (12.7%) | 3882 (30.2%) |
3034 (46.7%) |
627 (50.3%) |
2478 (41.5%) | 7455 (18.3%) | 3850 (12.0%) | 4852 (37.4%) | 1858 (62.6%) |
| Adequate number of health professionals | ||||||||||||||||
| Always | 31,808 (66.2%) | 27,038 (77.1%) | 4309 (40.6%) | 461 (19.7%) | 24,789 (75.2%) | 5252 (53.0%) | 1767 (34.3%) | 22,751 (79.4%) | 6779 (52.7%) |
2278 (35.1%) |
383 (30.7%) |
2419 (40.6%) | 29,006 (71.0%) | 25,515 (79.5%) | 5683 (43.8%) | 610 (20.5%) |
| Sometimes | 12,088 (25.2%) | 6744 (19.2%) | 4420 (41.6%) | 924 (39.6%) | 6526 (19.8%) | 3487 (35.2%) | 2075 (40.3%) | 4926 (17.2%) | 4593 (35.7%) |
2569 (39.5%) |
439 (35.2%) |
2377 (39.9%) | 9272 (22.7%) | 5580 (17.4%) | 5322 (41.1%) | 1186 (39.9%) |
| Never | 4143 (8.6%) | 1307 (3.7%) | 1885 (17.8%) | 951 (40.7%) | 1657 (5.0%) | 1179 (11.9%) | 1307 (25.4%) |
991 (3.5%) | 1502 (11.7%) |
1650 (25.4%) |
425 (34.1%) |
1168 (19.6%) | 2550 (6.2%) | 1013 (3.2%) | 1957 (15.1%) | 1173 (39.5%) |
| Logistic model | |||
|---|---|---|---|
| Positive birth perception (composite outcome) | |||
| Odds ratio | 95% CI |
| |
| Companion of choice allowed | |||
| Always | 2.11 | 2; 2.23 | < 0.001 |
| Sometimes | 1.45 | 1.35; 1.55 | < 0.001 |
| Never | Ref | Ref | |
| Adequate number of health professionals | |||
| Always | 2.12 | 1.95; 2.31 | < 0.001 |
| Sometimes | 1.1 | 1.02; 1.19 | 0.013 |
| Never | Ref | Ref | |
| Adequate assistance by health professional | |||
| Always | 2.12 | 1.86; 2.43 | < 0.001 |
| Sometimes | 1.24 | 1.09; 1.41 | < 0.001 |
| Never | Ref | Ref | |
| Immediate attention by health professional | |||
| Always | 36.64 | 27.77; 49.55 | < 0.001 |
| Sometimes | 4.91 | 3.71; 6.66 | < 0.001 |
| Never | Ref | Ref | |
| By birth mode and medical interventions | |||
| Vaginal birth | Ref | Ref | |
| Vaginal birth with episiotomy | 0.74 | 0.69; 0.79 | < 0.001 |
| Instrumental vaginal birth | 0.76 | 0.68; 0.86 | < 0.001 |
| Instrumental vaginal birth with fundal pressure | 0.52 | 0.46; 0.59 | < 0.001 |
| Planned cesarean birth | 0.8 | 0.74; 0.87 | < 0.001 |
| Unplanned cesarean birth, before the onset of labor | 0.6 | 0.54; 0.67 | < 0.001 |
| Unplanned cesarean birth, after the onset of labor | 0.52 | 0.48; 0.56 | < 0.001 |
| Age | |||
| 18–24 | 0.81 | 0.73; 0.91 | < 0.001 |
| 25–30 | 0.96 | 0.91; 1.01 | 0.124 |
| 31–35 | Ref | Ref | |
| 36–39 | 1.05 | 0.98; 1.12 | 0.178 |
| > 40 | 1.05 | 0.94; 1.16 | 0.41 |
| Parity | |||
| Primiparous | Ref | Ref | |
| Multiparous | 1.27 | 1.21; 1.34 | < 0.001 |
| Woman gave birth in the country she herself was born in | |||
| Yes | Ref | Ref | |
| No | 1.01 | 0.93; 1.1 | 0.813 |
| Level of education | |||
| Junior high school or lower | 0.97 | 0.88; 1.08 | 0.626 |
| High school | 0.94 | 0.89; 1 | 0.046 |
| University degree | Ref | Ref | |
| Postgraduate/master/doctorate | 0.93 | 0.88; 0.99 | 0.013 |
| Country | |||
| Other | 0.98 | 0.81; 1.18 | 0.809 |
| Austria | 1.05 | 0.83; 1.34 | 0.667 |
| Bosnia‐Herzegovina | 0.6 | 0.47; 0.78 | < 0.001 |
| Croatia | 0.6 | 0.54; 0.66 | < 0.001 |
| France | 1.15 | 1; 1.33 | 0.056 |
| Germany | 1 | 0.86; 1.15 | 0.949 |
| Greece | 0.68 | 0.59; 0.77 | < 0.001 |
| Latvia | 0.51 | 0.47; 0.57 | < 0.001 |
| Lithuania | 0.45 | 0.39; 0.52 | < 0.001 |
| Luxembourg | 1.03 | 0.83; 1.29 | 0.769 |
| Norway | 1.51 | 1.39; 1.65 | < 0.001 |
| Poland | 0.91 | 0.8; 1.03 | 0.131 |
| Portugal | 0.91 | 0.79; 1.05 | 0.188 |
| Romania | 1.08 | 0.93; 1.26 | 0.313 |
| Serbia | 0.45 | 0.37; 0.55 | < 0.001 |
| Slovenia | 0.9 | 0.8; 1 | 0.052 |
| Spain | 0.43 | 0.34; 0.55 | < 0.001 |
| Sweden | 1.38 | 1.28; 1.5 | < 0.001 |
| Switzerland | 1.15 | 1; 1.33 | 0.046 |
| Italy | Ref | Ref | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Perinatal Health Interventions · Global Maternal and Child Health · Maternal and fetal healthcare
Background
1
During the COVID‐19 pandemic, policymakers and health authorities in European countries imposed restrictions on access to maternity care facilities for birth companions and visitors, as a measure to slow the spread of the virus [1, 2]. These bans were implemented despite the evidence that shows the benefit of having a birth companion on health outcomes and a positive childbirth experience [3, 4]. The restrictions varied over time, among countries, and across facilities [5]. In some hospitals, birth companions were permitted under strict regulations, such as mandatory real‐time polymerase chain reaction (RT‐PCR) testing and mask‐wearing. Others allowed companions only during the second phase of labor. In certain countries, access to the maternity ward was restricted to patients, meaning that women (We include into our considerations all pregnant and childbearing individuals.) had to navigate labor, birth, and the postpartum period without a birth companion [2, 6]. International [7] and national (e.g., Germany [8], Italy [9], France [10]) obstetricians' and midwives' associations, and civil society initiatives voiced concerns and formally opposed bans on birth companions. These initiatives referenced the World Health Organization's (WHO) recommendation to ensure women have a companion of choice during birth, emphasizing it as a vital element of respectful and high‐quality maternity care and a fundamental right in childbirth [3, 4]. Restrictions on companionship can evoke concerns, psychological distress, and loneliness for women in labor [11], placing added strain on their partner or desired companion [12], the newborn [13], and health professionals providing care [14]. Having a birth companion of choice, whether the woman's partner, a relative, doula, or a friend, can positively influence the labor and birth process, as companions can support and empower the woman [15], offer emotional support, practical assistance during labor, serve as an informational and communicational bridge between health professionals and the woman, and advocate for the woman's wishes. The significance and advantages of having a birth companion of choice are well‐documented [16, 17].
An equally important aspect of respectful and high‐quality maternity care is the continuous support and care provided by a health professional (usually a midwife) during labor and birth [18, 19]. Health professionals can enhance outcomes through evidence‐based care and supportive actions, including comfort, emotional support, effective communication, and information sharing, thereby mirroring the benefits of a birth companion of choice [20, 21]. Inadequate ratios of health professionals to women can lead to stressful work environments and unnecessary medical interventions during labor and can negatively impact women's birth experiences [22]. It also compromises a woman's right to receive the highest attainable level of health care during childbirth [4]. During the pandemic, inadequate staffing in maternity wards intensified due to health professionals' own illness quarantine, reduced working hours due to stressful working conditions, parental and caregiving duties, or redistribution of maternity staff to COVID‐19 wards [23]. Inadequate ratios of staff to women also increases the chances that women will experience mistreatment, disrespect or abuse during labor and birth [24, 25].
We examined data from 20 countries to determine whether having a birth companion of choice and receiving timely and sufficient attendance by an adequate number of health professionals during labor and birth are associated with positive birth perception when controlling for potential confounders. Positive birth perception refers to a woman's assessment of how she is being valued and treated as an individual, including preserving her integrity and autonomy [26, 27].
Methods
2
Study Design, Participants, and Data Collection
2.1
This study is part of the ongoing IMAgiNE EURO (Improving MAternal Newborn CarE In the EURO Region) project, which is collecting cross‐sectional data women's perspectives of the quality of maternal and newborn care (QMNC) in health facilities. Eligible participants included women aged 18 or older who gave birth in a maternity facility in the WHO European Region during the COVID‐19 pandemic (data collection start: March 1, 2020, data download for this study: March 1, 2023). Participants had the option of reporting on multiple births if they occurred within the study period. A structured, validated online questionnaire [28] was disseminated by project partners from over 20 countries and in 25 languages. Questions were based on WHO Quality Measures for improving the QMNC in health facilities, [29] using the three WHO domains of care (provision of care, experience of care, and availability of human and physical resources). Other questions pertained to organizational changes related to the COVID‐19 pandemic and sociodemographic data. The questionnaire design and setting‐specific dissemination strategies were described in prior publications [28, 30, 31, 32, 33, 34]. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting on cross‐sectional studies were applied [35] (Supporting Information: File S1).
Study Variables
2.2
Outcome Variable: Positive Birth Perception
2.2.1
Positive birth perception is defined as a woman's assessment of how she is valued and treated as an individual, and includes the preservation of her integrity and autonomy [26, 27, 36]. This was assessed using five key variables, which women then assessed on a scale of always/sometimes/never. Women reported on these five variables were as follows: (i) feeling treated with dignity, (ii) feeling emotionally supported by health professionals, (iii) feeling fully involved in choices regarding care and feeling that autonomy was respected, (iv) perceiving health professionals' communication to be clear and effective, and (v) reporting any kind of mistreatment, disrespect, or abuse (verbal, emotional, and physical). Using these five variables, we calculated a composite discrete score of positive birth perception ranging from 0 to 10, with 10 being the most positive perception of birth and 0 being the least positive perception of birth (with the following scoring for variables i–iv: always = 2 points, sometimes = 1 point, never = 0 points, and the following scoring for variable v: never = 2 points, sometimes = 1 point, always = 0). We dichotomized the birth perception score (10/< 10). A score equal to 10 indicates fully positive perception of birth. Due to the distribution of the variables, it seemed reasonable to dichotomize between (10/< 10). While recognizing that scores of 9, 8, or 7 might still be considered positive perceptions of birth, our aim with this study is to better understand the factors that contribute to a fully positive perception of birth.
Independent Variables
2.2.2
Independent variables were measured using the same scale as outcome variables (always/sometimes/never). Having a birth companion of choice was measured through a variable that asked if participants were allowed to have their chosen companion present during and after birth. Health professionals' attention, assistance, and availability during labor and birth from the participants' perspective was measured through three variables: (i) whether the number of health professionals was adequate considering the workload; (ii) whether the health professionals were present in sufficient numbers to guarantee adequate assistance; and (iii) whether participants felt they received immediate attention from health professionals when they needed it.
Potential Confounders
2.2.3
Socioeconomic and health‐related variables considered potentially relevant to the birth process and the provision of maternity care include maternal age, education, country, whether the mother was born in the same country where she gave birth to the infant, mode of birth, and birth interventions [37, 38, 39].
Data Analysis
2.2.4
Responses missing ≥ 90% of key variables, suspected duplicates, and entries with missing values in independent or outcome variables were excluded from the dataset, as described elsewhere [28]. Descriptive statistics were used to explore the distribution of outcomes and independent variables. Considering the skewed score distribution, we displayed the positive birth perception score distribution from 0 to 10 overall and for all countries graphically. We performed chi‐squared tests to assess whether independent variables differed by the dichotomized positive birth perception score. Lastly, we conducted a multivariate logistic regression analysis to estimate the associations between the dichotomized outcome of positive birth perception (outcome variable), presence of a birth companion of choice, and health professionals' attention and assistance (three variables). We controlled for the following potential confounders: age, education, parity, country, whether the mother was born in the same country where she gave birth, birth mode, and presence of medical interventions (vaginal birth, vaginal birth with episiotomy, instrumental vaginal birth, instrumental vaginal birth with fundal pressure, planned cesarean birth, and unplanned cesarean birth before or after the onset of labor). The category with higher frequency was chosen as the reference. For the sensitivity analysis, we performed a linear regression model on a subset of women with a score < 10 to explore associations between not‐perfect scores and the variables of interest. The discrete score was used as an outcome variable, while we used the same independent variables used in the logistic model. Statistical analyses were performed using Stata/SE version 14.0 (Stata Corporation, College Station, TX, USA) and R version 4.2.2: A language and environment for statistical computing (R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R‐project.org/).
Ethics Aspects
2.3
This voluntary and anonymous study was approved by the Institutional Review Board of the IRCCS Burlo Garofolo Trieste (IRB‐ Burlo 05/2020 15.07.2020) (Coordination center). The study was conducted according to General Data Protection Regulation (GDPR) regulations. Before participation, participants were informed of the objectives and methods of the study, including their rights in declining participation. Consent was provided before responding to the questionnaire, and participants could stop responding at any time. The study was approved by the ethics committees in four partner countries: Portugal (Instituto de Saúde Pública da Universidade do Porto, CE20159); Norway (Norwegian Regional Committee for Medical Research Ethics, 2020/213047), Germany (Bielefeld University ethics committee, 2020‐176), and Latvia (Rīgas Stradiņa universitātes, 22‐2/140/2021‐16/03/2021). Ethics approval was not necessary in other partner countries, as anonymity in data collection during the survey phase was ensured and no data were collected that disclosed participants' identities. Data transmission and storage were secured by encryption.
Results
3
Sample Characteristics
3.1
A total of 70,721 participants accessed the online questionnaire, from which 48,039 matched the inclusion criteria for this study (Figure 1).
Flow diagram. 1We used 45 key variables (40 key quality measures and five key sociodemographic questions). 2Independent variables are as follows: dignity, emotional support, involvement, abuse, and communication. Dependent variables are as follows: companion of choice, adequate assistance by a health professional, adequate number of health professionals, and immediate attention by a health professional.
The study sample characteristics are summarized in Table 1. More than half of the participants were highly educated (over 70.0% (n = 34,416) having a university degree), between 25 and 35 years old (74.1%; n = 35,808), and reported on their first birth (60.9%; n = 29,275). Most births were attended by a midwife (88.9%; n = 42,700) and/or an obstetrician, medical doctor, or medical resident (62.6%, n = 30,073). Over 90% (n = 44,445) of women gave birth in the same country where they were born.
As displayed in Table 2, 74.0% (n = 35,491) of all women gave birth vaginally, 49.7% (23,863) had no medical interventions (as defined in this study) during their vaginal birth, whereas 16.2% (n = 7781) gave birth vaginally with an episiotomy. Another 4.5% (n = 2141) of all women experienced an instrumental vaginal birth, and a further 3.6% (n = 1706) experienced instrumental vaginal birth with fundal pressure. In all, 26% (n = 12,548) of women had a cesarean birth. Of the total sample, planned cesarean births were reported by 10.8% (n = 5192), 5.2% (n = 2475) reported an unplanned cesarean birth before the onset of labor, and 10.2% (n = 4881) reported an unplanned cesarean birth after the onset of labor.
Overall, Table 2 shows that 41.6% (n = 19,988) of respondents reported that having a birth companion was always possible, 15.3% (n = 7341) reported sometimes, and 43.1% (n = 20,710) reported never. Over two‐thirds of the women felt that they always received immediate attention when needed (67.2%; n = 32,295) and that health professionals were available in adequate numbers all the time (always: 66.2%; n = 31,808). Overall, 41.3% (n = 19,861) respondents reported that they always experienced adequate assistance by health professionals.
Descriptive statistics for indicators of positive birth perception reveal that 48.7% (n = 16,072) of women who were always accompanied by a companion always felt emotionally supported, 50.1% (n = 14,364) always felt involved in decision‐making, 48.9% (n = 15,688) always experienced clear and effective communication from health professionals, 49.4% (n = 17,338) always felt treated with dignity, and 44.5% (n = 18,188) never experienced abuse. Conversely, among women who reported never receiving immediate attention from their health professional, 53.1% (n = 1240) reported never being treated with dignity, 27.9% (n = 1438), never feeling supported, 27.7% (n = 1802) reported never being involved in decision‐making, and 53.2% (n = 1579) reported never having effective communication. Of this same group, 43.3% (n = 540) reported always experiencing abuse. Generally, the measures for immediate attention, adequate assistance, and an adequate number of health professionals show similar distributions in the positive perception of birth indicators, as shown in Table 2.
Positive Perception of Birth
3.2
Around 43% (n = 20,918) of all women reported a positive birth perception score of 10, with the remaining scores ranging from 9 to 0, with decreasing frequency as the score decreases. There was a variation in score distribution across countries. Distribution for individual countries and overall can be found in Supporting Information: File S2.
Multivariate Analyses
3.3
As displayed in Table 3, the logistic regression model shows that reporting being always (aOR: 2.11; CI: 2.00; 2.23) or at least sometimes (aOR: 1.45; CI: 1.35; 1.55) having a birth companion of choice was associated with increased odds of a positive birth experience compared to women who did not have a birth companion of choice. All variables on health professionals' availability, assistance, and attention also showed a significant association with a positive birth perception. Reporting being always adequately assisted throughout labor and birth (aOR: 2.12; CI: 1.86; 2.43), always receiving immediate attention (aOR: 36.64; CI: 27.77; 49.55), and reporting that there was always an adequate number of health professionals available (aOR: 2.12; CI: 1.95; 2.31) were all associated with higher odds of a positive perception of birth. Having health professionals available sometimes (aOR: 1.10; CI: 1.02; 1.19) and receiving their assistance (aOR: 1.24; CI: 1.09; 1.41) and attention sometimes (aOR: 4.91; CI: 3.71; 6.66) were also associated with a higher probability of a positive perception of birth compared with women who reported never receiving assistance or attention by health professionals or who reported that health professionals were not available in adequate numbers.
TABLE 3: Logistic model result, positive birth perception is dichotomized 10 versus < 10 (n = 48,039).
Concerning the different birth modes and medical interventions, compared with women who reported a vaginal birth, those who had an instrumental vaginal birth were less likely to have a positive birth experience (aOR: 0.76; CI: 0.68; 0.86). Medical interventions such as episiotomies in women with vaginal birth (aOR: 0.74; CI: 0.69; 0.79) and fundal pressure in women with instrumental vaginal birth (aOR: 0.52; CI: 0.46; 0.59) were associated with decreased odds of a positive perception of birth. All types of cesarean births were negatively associated with positive birth perception, from women with planned cesarean births (aOR: 0.80; CI: 0.74; 0.87) to those with unplanned cesarean births before (aOR: 0.60; CI: 0.54; 0.67) and after the onset of labor (aOR: 0.52; CI: 0.48; 0.56). Women younger than 25 years (aOR: 0.81; CI: 0.73; 0.91) showed significantly lower odds of a positive perception of birth compared to women aged 25 or older. No further age effect was observed.
No significant difference was found between women giving birth in their own country of birth and those who gave birth in a foreign country. Women from Norway (aOR: 1.51; CI: 1.39; 1.65), Sweden (aOR: 1.38; CI: 1.28; 1.5), and Switzerland (aOR: 1.55; CI: 1.; 1.33) had significantly higher odds of experiencing their birth positively compared with women from Italy, whereas women from Spain (aOR: 0.43; CI: 0.34; 0.55), Lithuania (aOR: 0.45; CI: 0.39; 0.52), Latvia (aOR: 0.51; CI: 0.47; 0.57), Serbia (aOR: 0.45; CI: 0.37; 0.55), Greece (aOR: 0.68; CI: 0.59; 0.77), Croatia (aOR: 0.60; CI: 0.54; 0.66), and Bosnia‐Herzegovina (aOR: 0.60; CI: 0.47; 0.78) were more likely to have less positive birth perceptions than women from Italy. No significant differences for positive perception of birth were observed for Austria, France, Germany, Luxembourg, Poland, Portugal, Romania, and Slovenia, compared with women from Italy.
Sensitivity Analysis
3.4
The sensitivity analysis presented similar results to the primary logistic regression model and supported the association between the health professionals' attention, assistance, and availability; the presence of a birth companion of choice; and the effect of mode of birth and medical interventions on perception (Supporting Information: File S3).
Discussion
4
Given the significant changes health systems underwent during the COVID‐19 pandemic, this study's findings are particularly relevant. With data from more than 48,000 women in 20 WHO European Region countries, we underscore the importance of ensuring QMNC standards even during extraordinary situations such as the pandemic, as a way of ensuring maternal health and well‐being. We found that 40% of the women in our sample did not have a birth companion of choice, and this limitation was associated with a lower likelihood of positive birth perception. Increased experiences of disrespect and abuse were more frequent among women who did not have a birth companion of choice. Our findings are in line with existing research, indicating that the presence of a birth companion of choice can be a protective factor against disrespect and abuse during childbirth [25]. Our findings also align with previous research highlighting the manyfold benefits of birth companions [40].
Our study also aligns with research showing that respectful maternity care is crucial and linked to positive birth experiences [41, 42]. Research shows that staff shortages and COVID‐19 containment measures negatively impacted the delivery of respectful maternity care, as reported by health professionals [43] and women [44]. In anticipation of future crises, it is imperative to develop guidelines that assess the best‐available evidence to protect the health and well‐being of both healthcare providers and birthing women, while maintaining quality, respectful maternity care, including ensuring a birth companion of choice whenever possible.
Our study indicates that women who consistently receive attention, assistance, and have access to an adequate number of health professionals are most likely to have a positive perception of their birth. The importance of a labor companion and attentive care is vital in crises and during normal times, improving maternal care quality and postpartum health outcomes by fostering positive birth experiences and preventing traumatic birth experiences [45, 46, 47].
Our research also adds to the existing literature [48, 49] by showing an association between the mode of birth and women's perceptions. Women with vaginal births tended to report more positive birth perceptions, whereas births involving higher degrees of medical intervention, such as instrumental vaginal birth, the use of fundal pressure, or unplanned cesarean birth initiated after the onset of labor, were often associated with less positive perceptions of birth. This is likely a reflection of the potentially stress‐inducing conditions surrounding (unplanned) interventions and a birth mode not aligned with the birthing woman's expectations.
Strengths and Limitations of This Study
4.1
The development, validation, implementation, and translation of the survey, as well as the data collection and analysis processes, have been thoroughly detailed in previous publications by the IMAgiNE study group [28, 30]. A notable strength of this study is the sample size, which provides a comprehensive dataset of birthing experiences from women across Europe.
Our online study may have a selection bias, attracting participants with higher levels of education, better internet access, and a willingness to share their birth experiences, both positive and negative [50]. Methodological choices might have led to underreporting of medical interventions (e.g., fundal pressure and episiotomies were queried only in specific birth contexts). The questionnaire has recently been revised for clearer differentiation of interventions and birth modes to overcome this issue. Another limitation is related to the analytical framework of this study. The composite outcome for positive birth perception was not directly measured with specifically designed questions. Instead, it was deduced from a combination of variables selected by the authors, based on relevant literature, which are believed to adequately represent aspects of a positive birth perception.
Conclusion
4.2
Our study offers important new evidence by presenting associations between the positive perception of birth, the level of professional support provided to women, and the presence of a chosen companion during labor and birth in 20 countries. It suggests that it is crucial to ensure an adequate number of health professionals available to deliver high‐quality and respectful maternity care and ensure that women have a companion of choice throughout labor and birth. This new evidence will hopefully contribute to increased investments in maternity care that place a high value on the perception that women have of their labor and birth.
Disclaimer
5
The authors alone are responsible for the views expressed in this article, and they do not necessarily represent the views, decisions, or policies of the institutions with which they are affiliated.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
File S1.
File S2.
File S3.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1K. Coxon , C. F. Turienzo , L. Kweekel , et al., “The Impact of the Coronavirus (COVID‐19) Pandemic on Maternity Care in Europe,” Midwifery 88 (2020): 102779.32600862 10.1016/j.midw.2020.102779 PMC 7286236 · doi ↗ · pubmed ↗
- 2T. S. Eri , E. Blix , S. Downe , C. Vedeler , and A. B. V. Nilsen , “Giving Birth and Becoming a Parent During the COVID‐19 Pandemic: A Qualitative Analysis of 806 Women's Responses to Three Open‐Ended Questions in an Online Survey,” Midwifery 109 (2022): 103321.35349790 10.1016/j.midw.2022.103321 PMC 8935971 · doi ↗ · pubmed ↗
- 3World Health Organization , Companion of Choice During Labour and Childbirth for Improved Quality of Care (World Health Organization, 2020).
- 4White Ribbon Alliance , Respectful Maternity Care (Universal Rights of Childbearing women, 2011).
- 5D. Drandić , K. Hartmann , C. Barata , and R. Torguet , “Parent Organizations' Experiences of the Pandemic Response in Maternity Care in Thirteen European Countries,” European Journal of Midwifery 6, no. December (2022): 1–10.10.18332/ejm/156902 PMC 977326736591331 · doi ↗ · pubmed ↗
- 6K. S. Arora , J. T. Mauch , and K. S. Gibson , “Labor and Delivery Visitor Policies During the COVID‐19 Pandemic: Balancing Risks and Benefits,” Journal of the American Medical Association 323, no. 24 (2020): 2468–2469.32442264 10.1001/jama.2020.7563 PMC 7736929 · doi ↗ · pubmed ↗
- 7“Women's Rights in Childbirth Must be Upheld During the Coronavirus Pandemic [press release].” 29.03.2020 2020.
- 8“DGGG Empfiehlt: Begleitung bei der Geburt zulassen – Auch in Zeiten der Corona‐Pandemie [press release].” 26.03.2020 2020.