Case Report: Necrotizing granulomas in the central nervous system: sarcoidosis masquerading as neurotuberculosis
Clothilde Gros, Karolina Hankiewicz, Adrien Carle, Dominique Cazals-Hatem, Mickael Bonnan

TL;DR
This case report describes two patients with central nervous system granulomas that initially resembled tuberculosis but were later diagnosed as sarcoidosis.
Contribution
The paper highlights the diagnostic challenge of necrotizing sarcoid granulomatosis in the central nervous system mimicking tuberculosis.
Findings
Necrotizing granulomas in the brain were initially treated as tuberculosis but showed no improvement.
Immunosuppressive treatment led to sustained remission, supporting a sarcoidosis diagnosis.
NSG in the central nervous system should not exclude the possibility of sarcoidosis.
Abstract
Neurosarcoidosis (NS) can affect patients with or without any systemic involvement. Diagnosis of NS without lung involvement requires (i) a biopsy showing typical non-necrotizing granulomas and (ii) exclusion of tuberculosis by negative culture for M. tuberculosis and PCR amplification techniques. In the absence of microbiological infection, the diagnosis is challenging when granulomas are necrotizing mimicking tuberculosis on histology. We report two cases presenting neurological symptoms and radiological lesions that were concordant with the diagnosis of NS. Nevertheless, brain biopsy showed necrotizing granulomas. Antineutrophil cytoplasmic antibodies (ANCA) showed a negative finding. Given the biopsy results, we started anti-tuberculosis treatment despite negative mycobacterial test results. Lack of improvement suggested the diagnosis of necrotizing sarcoid granulomatosis (NSG). NSG…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
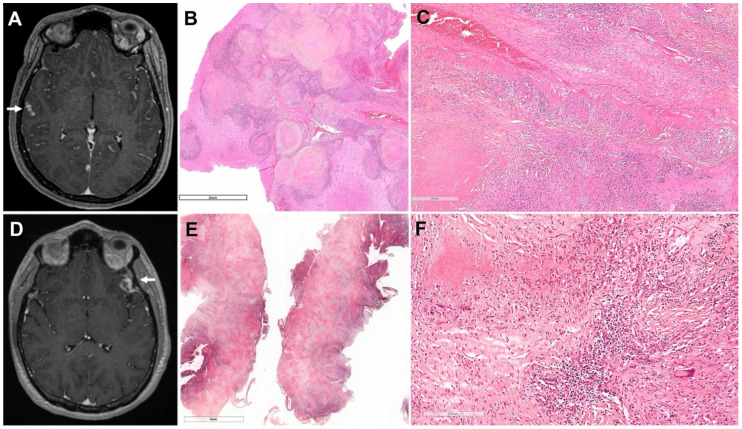 Figure 1
Figure 1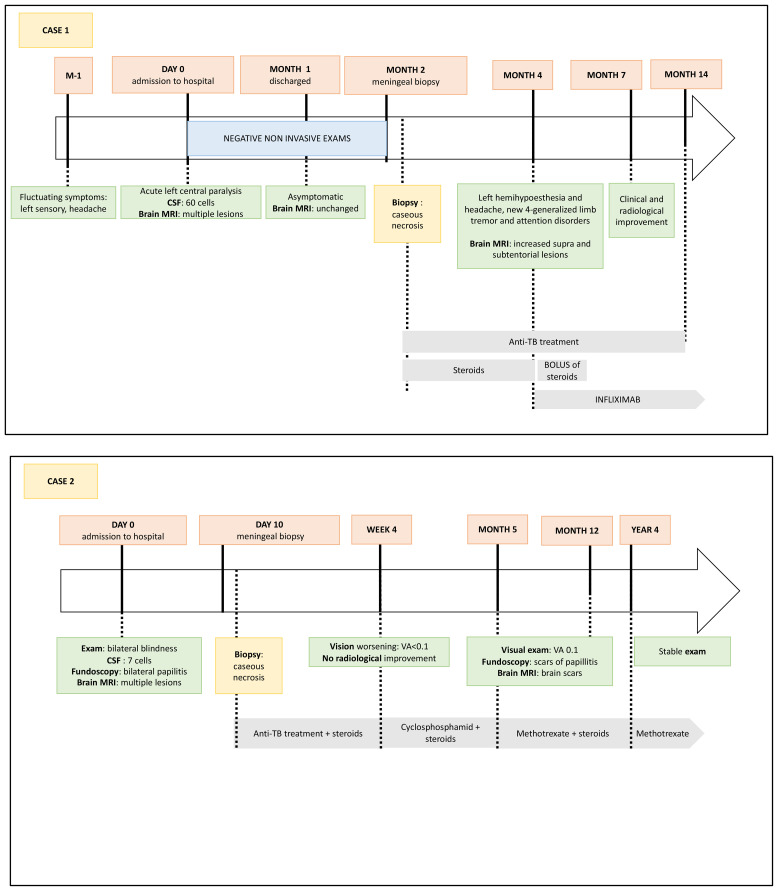 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Infectious Diseases and Tuberculosis · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
Sarcoidosis is a multisystem granulomatous disease of unknown origin that preferentially affects the lungs but can involve any organ. It affects the central nervous system (CNS) in 5% to 26% of patients with or without any systemic manifestations, and neurological symptoms are isolated in 10% to 28% of cases (1). The diagnosis of neurosarcoidosis (NS) is based on a range of clinical (i.e., meningitis, focal signs, cranial neuropathies, myelopathy), biological (i.e., hypercalcemia, hypergammaglobulinemia, increased angiotensin-converting enzyme [ACE]), and radiological signs with proven histology, while eliminating other differential granulomatous diagnoses such as infections, neoplasia, and vasculitis. Even if a neurological biopsy may be difficult to obtain, the presence of non-necrotizing granulomas remains a diagnostic pillar after ruling out infectious diseases, which can lead to the initiation of steroids or antitumor necrosis factor drugs (2). On the other hand, necrotizing granulomas are highly uncommon in sarcoidosis but provide strong evidence in favor of infection. We report two cases in which necrotizing granulomas on brain biopsy initially obscured the diagnosis.
Case description
Case 1
A woman in her 30s without any medical or familial history presented fluctuating left-side numbness and moderate headache. One month later, she was admitted to the emergency unit for acute left central facial paralysis. Brain magnetic resonance imaging (MRI) showed multiple contrast-enhancing T1 hyperintensities of tentorial and infra-tentorial white matter and leptomeningeal contrast-enhancement but no signs of recent ischemic stroke (Figure 1; Supplementary Figure S1). Her cerebral spinal fluid (CSF) level was 60 cells/µL, mainly lymphocytes with increased proteins (64 mg/dL) and normal glucose. Oligoclonal bands were present and ACE was normal. Interleukin-6 and interleukin-10 levels were not suggestive of lymphoma, and immunophenotyping showed a normal result. Results of bacterial and mycobacterial cultures, M. tuberculosis PCR, and test for cryptococcal antigen remained negative. Ocular examination revealed a unilateral posterior uveitis scar. Fluorodeoxyglucose-positron emission tomography revealed intense diffuse hypermetabolism of the tissues of the oral sphere, abnormally pronounced hypermetabolism of the spinal cord, and diffuse unspecific bone marrow hypermetabolism. Spinal MRI demonstrated leptomeningeal contrast enhancement at the level of the terminal cone and lower dorsal medulla. Nasal cavity biopsy revealed one granuloma without necrosis, and a salivary gland biopsy was normal. Blood count, ionogram, liver tests, and calcium had normal results. Other wide-spectrum non-invasive investigations showed normal findings including ACE in blood and CSF, negative antinuclear anti-phospholipids and anti-neuronal antibodies, positive antineutrophil cytoplasmic antibodies (ANCA) without any PR3 or MPO, no hypergammaglobulinemia, negative HCV and HIV serology, protective HBV serology, negative BD-glucans, and normal body CT scan.
Imaging and histopathological findings at onset. Patient 1 (A–C) – (A) T1-weighted brain MRI showing multiple leptomeningeal enhancements (right temporal lesion analyzed on histology, arrow). (B) Cortical lesion shows an accumulation of necrotic nodules surrounded by fibrosis and lymphocytes. (C) Many epithelioid granulomas are observed along an occluded artery at a distance from the nodules. Grocott’s methenamine silver and Ziehl’s colorations were negative (not shown). Patient 2 (D–F) – (D) T1-weighted brain MRI at onset showing a contrast-enhanced left temporal lesion (left frontal lesion analyzed on histology, arrow). (E) Cortical lesion shows diffuse central necrosis surrounded by fibrosis and a rim of chronic lymphoid inflammation. (F) Epithelioid and giant cell granulomas form the inflammation around the fibrinoid necrosis. Giemsa, PAS, and Ziehl’s colorations were negative (not shown).
Facial palsy and headache abated spontaneously, but control brain MRI showed the persistence of contrast-enhancing intraparenchymal hyperintense FLAIR signals. Right temporal neuromeningeal biopsy revealed a conglomerate of granuloma characterized by epithelioid and Langhans giant cells surrounding eosinophilic acellular necrosis (Figure 1), suggesting an active tuberculosis (TB). Ziehl Neelsen’s stain and mycobacterial cultures on CSF and biopsy, QuantiFERON-TB test, and PCR for M. tuberculosis on CSF showed negative findings; chest CT scan also presented normal results. Quadritherapy against TB and steroids were started in January 2022.
After 2 months of treatment, steroids were tapered. Left hemihypoesthesia and headache soon reappeared followed by limb tremor and the development of an attention disorder. Brain MRI showed a larger nodular leptomeningeal contrast enhancement. Findings of further immunological tests remained negative. The patient was diagnosed with immune reconstitution inflammatory syndrome, so the steroid dose was increased again, leading to transient incomplete improvement of headache and general status. Reassessment after 12 months of anti-TB showed the persistence of lymphocytic meningitis and progression of lesions radiologically. The diagnosis was reconsidered, and high-dose steroids and infliximab perfusions (5 mg/kg/month) were administered. Infliximab was chosen given its greater efficacy in severe NS (3). Reassessment during the next 2 years showed major MRI and clinical improvement (Figure 2).
Historical timeline of cases.
Case 2
A 39-year-old man without any medical or familial history was admitted to the neurology department for neuropapillitis manifested by subacute bilateral blindness. He initially complained of a monolateral decrease in visual acuity that affected the contralateral eye a few weeks later with bilateral blindness. At admission, brain MRI showed left temporal and peri-ventricular neuromeningeal lesions with contrast enhancement (Figure 1; Supplementary Figure S2). Clinical examination presented normal findings except for the blindness. His CSF level was 7 cells/µL with a discrete increase in protein level (50 mg/dL), normal glucose level, and the presence of oligoclonal bands. Tests for M. tuberculosis PCR, RNA 16S PCR, and cryptococcal antigen all showed negative results.
As non-invasive investigations were not informative (normal blood count, ionogram, liver test, and CRP; negative Bartonella, syphilis, Lyme, and HIV serologies with negative QuantiFERON-TB; negative ANCA and anti-neuronal antibodies; and normal ACE), a left temporal neuromeningeal biopsy was performed. Histology revealed granulomatous inflammation with acellular necrosis suggestive of TB (Figure 1) despite negative bacterial and mycobacterial cultures and M. tuberculosis PCR. Despite the initiation of anti-TB treatment and steroids, there was no clinical or radiologic improvement so the diagnosis of sarcoidosis was evoked. After 1 month, the anti-TB treatment was stopped and replaced by high-dose steroids and short-course IV cyclophosphamide (with trimethoprim and sulfamethoxazole as prophylaxis for Pneumocystis jirovecii pneumonia), with a subsequent switch to methotrexate (0.3 mg/kg/week). The size of the brain lesions began to decrease on MRI. After 2 years of methotrexate, the patient’s visual acuity had slightly improved. Fundoscopy showed optic atrophy and no inflammation, and brain MRI only highlighted parenchymal scars, including the frontal one, with no disease activity. Steroids were tapered and discontinued after 4 years of treatment, but methotrexate was continued (Figure 2).
Discussion
These patients illustrate the difficulty in the diagnosis of NS: Both presented with a suggestion of NS, whereas the biopsy led to a diagnosis of tuberculosis due to an unexpected necrotizing granuloma. Given the negative infectious context and immunological tests (especially ANCA), the diagnosis of NS was likely on histology. Additional necrosis confused with infection, mainly tuberculosis and chronic fungal infections (such as histoplasmosis, aspergillosis, and cryptococcosis) and with necrotizing vasculitis such as Wegener’s granulomatosis (4–6). Excluding these latter diagnoses, the lack of improvement with anti-TB treatment was decisive for the diagnosis of NS, characterized by well-circumscribed perivascular epithelioid and giant-cell granulomas generally located at the surface of the brain or meninges. Necrosis is rarely described in sarcoidosis and, when present, is limited, focal, and non-caseous on gross description. Fibrosis replaces the necrosis in chronic cases (2, 7). Necrotizing sarcoid granulomatosis (NSG) has previously been described in the brain, interpreted as a late stage of nodular sarcoidosis in which granulomas distributed along vessels cause fibrosis and secondary ischemic lesions (8). Some authors proposed the term “sarcoidosis with a necrotizing sarcoid granulomatosis pattern” (9).
NSG is very rare and mainly involves the lungs, whereas CNS is usually spared. A review found that in at least 6% of cases of pulmonary NSG, the CNS was also affected, although rarely biopsied (10). Neuromeningeal biopsy was considered too invasive a procedure, so it remains unclear how often necrotizing lesions observed in the lung may also occur in CNS lesions. We reviewed NSG with CNS involvement and found 25 cases including ours (see Supplementary Table S1). No systemic sarcoidosis was observed in 21/25. CNS lesions encompassed the range of usual NS lesions without an apparent specific pattern. The biopsy location was in the CNS in 17/24, in the orbit in 2/24, and otherwise in the lung. Pathology showed granuloma in all cases, necrotizing lesions in 21/25 and vasculitis in 6/23. All cases of vasculitis were observed in lung or orbit biopsies.
The present observations of NS are particularly interesting because both patients had no history of known sarcoidosis prior to CNS onset, and both benefited from full histological analysis showing granulomas with necrosis, which was atypical for a sarcoidosis. These patients are still in remission a few years after the diagnosis, and CNS lesions disappeared. As about 30% to 50% of patients with NS relapse, albeit with lower rates under immunosuppressive therapy (11, 12), the diagnosis remains robust even without any relapse. Moreover, the spontaneous remission of an unproven infectious disease, especially TB, can be ruled out.
Conclusion
Histology of neurosarcoidosis is usually informative when showing non-necrotizing granulomas. The diagnosis is challenging when granulomas are necrotizing in the absence of microbiological infection. Clinicians should be made aware that the diagnosis of NS should not be completely ruled out by the presence of CNS necrotizing lesions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barreras P Stern BJ . Clinical features and diagnosis of neurosarcoidosis – review article. J Neuroimmunol. (2022) 368:577871. doi: 10.1016/j.jneuroim.2022.577871, PMID: 35523055 · doi ↗ · pubmed ↗
- 2Stern BJ Royal W Gelfand JM Clifford DB Tavee J Pawate S . Definition and consensus diagnostic criteria for neurosarcoidosis: from the neurosarcoidosis consortium consensus group. JAMA Neurol. (2018) 75:1546. doi: 10.1001/jamaneurol.2018.2295, PMID: 30167654 · doi ↗ · pubmed ↗
- 3Chaiyanarm S Satiraphan P Apiraksattaykul N Jitprapaikulsan J Owattanapanich W Rungjirajittranon T . Infliximab in neurosarcoidosis: a systematic review and meta-analysis. Ann Clin Transl Neurol. (2024) 11:466–76. doi: 10.1002/acn 3.51968, PMID: 38087813 PMC 10863903 · doi ↗ · pubmed ↗
- 4Tana C Donatiello I Caputo A Tana M Naccarelli T Mantini C . Clinical features, histopathology and differential diagnosis of sarcoidosis. Cells. (2021) 11:59. doi: 10.3390/cells 11010059, PMID: 35011621 PMC 8750978 · doi ↗ · pubmed ↗
- 5Rammeh S Romdhane E Riahi H Chebbi Y Bouaziz MC Achour W . Granulomatous spondylodiscitis: A case series with focus on histopathological features. J Spinal Cord Med. (2021) 44:282–7. doi: 10.1080/10790268.2019.1607054, PMID: 31012811 PMC 7952049 · doi ↗ · pubmed ↗
- 6Kitajima S Sakai N Furuichi K Tomokage M Hara A Kitagawa K . A case of neurosarcoidosis with necrotizing granuloma expressing angiotensin-converting enzyme. Mod Rheumatol. (2010) 20:506–10. doi: 10.3109/s 10165-010-0301-y, PMID: 20499262 · doi ↗ · pubmed ↗
- 7Statement on sarcoidosis. Am J Respir Crit Care Med. (1999) 160:736–55. doi: 10.1164/ajrccm.160.2.ats 4-99, PMID: 10430755 · doi ↗ · pubmed ↗
- 8Churg A Carrington CB Gupta R . Necrotizing sarcoid granulomatosis. Chest. (1979) 76:406–13. doi: 10.1378/chest.76.4.406, PMID: 477427 · doi ↗ · pubmed ↗