Comparison of patient outcomes between video and non-video laryngeal mask airway insertion performed by novices: a prospective randomized controlled study
Ye Jiang, Fang Xing, Qian Wu, Yanan Gao, Guozhong Chen, Cheng Li

TL;DR
This study finds that video laryngeal mask airways are easier for novices to use and cause less patient discomfort than non-video versions.
Contribution
The study provides empirical evidence that video laryngeal mask airways improve novice performance and reduce patient injury.
Findings
Both groups achieved 100% first-attempt success in LMA insertion.
The V-LMA group showed better bronchoscope alignment and lower postoperative throat pain.
V-LMA insertion resulted in better intraoperative hemodynamic stability.
Abstract
This study compares the patient outcomes of video laryngeal mask airway (V-LMA) and non-video laryngeal mask airway (NV-LMA) to assess which is easier for novices to master, achieves faster placement success, and causes least injury to the patients. Twenty novice practitioners (resident doctors/anesthesia nurses) from the Department of Anesthesia and Perioperative Medicine, Shanghai Fourth Peoples' Hospital, were randomized 1:1 to the V-LMA or NV-LMA group. After standardized training, the participants performed supervised LMA insertions on 60 patients. The learning outcomes and patient injury rates during LMA placement were compared between the groups. Both groups achieved 100% first-attempt success. The V-LMA group demonstrated superior bronchoscope alignment (90% vs. 50%, P = 0.001). Postoperative throat pain was experienced by patients in both groups, but the V-LMA group…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
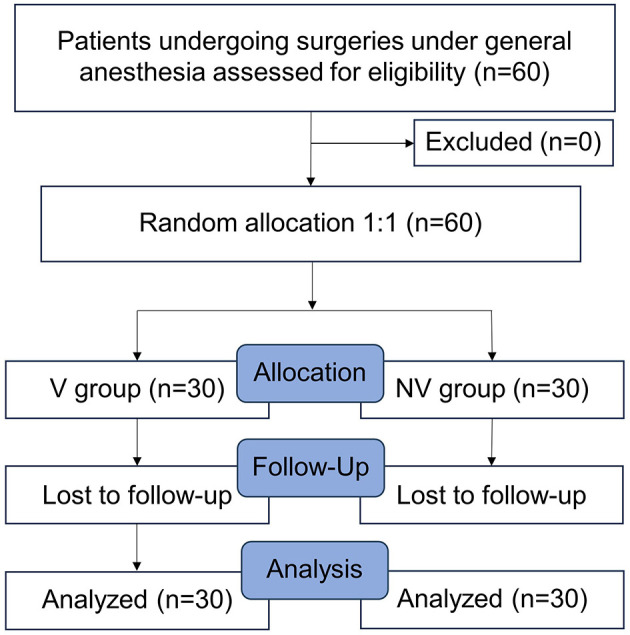 Figure 1
Figure 1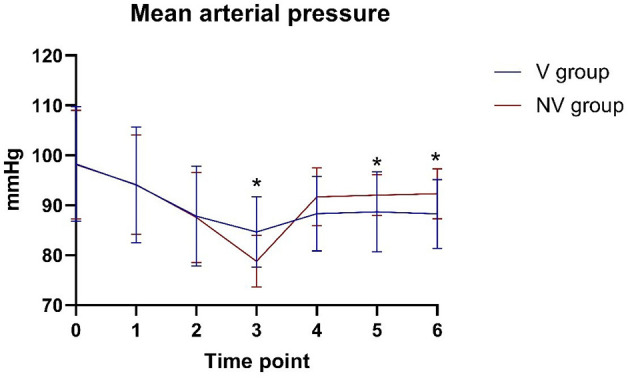 Figure 2
Figure 2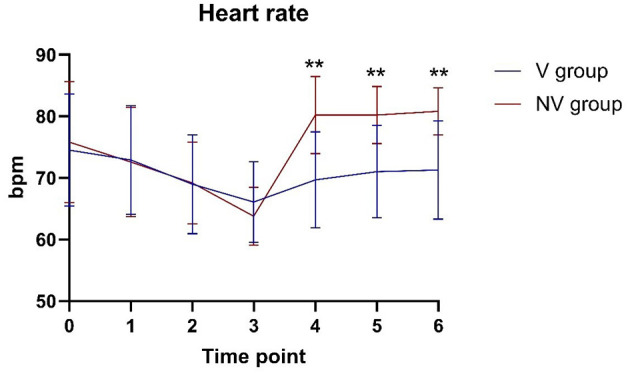 Figure 3
Figure 3|
|
|
|
|
|---|---|---|---|
| Age(years) | 49.63 ± 16.368 | 53.93 ± 15.163 | 0.296 |
| Male/Female | 19/11 | 18/12 | 0.071 |
| BMI(kg/m2) | 23.373 ± 1.7815 | 22.777 ±1.9310 | 0.219 |
|
|
|
|
|
|---|---|---|---|
| Time required for successful insertion (seconds) | 17.77 ± 7.29 | 14.57 ± 6.79 | 0.084 |
| Bronchoscope grade of I ( | 27 (90%)* | 15 (50%) | 0.001 |
| 3 (10%)* | 15 (50%) | 0.003 |
|
|
|
|
|
|---|---|---|---|
| Blood stains ( | 6 (20%) | 8 (26.75%) | 0.542 |
| Postoperative throat pain after 1 h ( | 6 (20%)* | 14 (46.7%) | 0.028 |
| Postoperative throat pain after 24 h ( | 17 (56.7%) | 19 (63.3%) | 0.598 |
|
|
|
|
|
|---|---|---|---|
| Patient | Very satisfactory ( | 22 (73.3%) | 24 (80%) |
| Satisfactory ( | 8 (26.7%) | 6 (20%) | |
| Common ( | 0 (0%) | 0 (0%) | |
| Unsatisfactory ( | 0 (0%) | 0 (0%) | |
| Instructor | Very satisfactory ( | 20 (66.7%) | 23 (76.7%) |
| Satisfactory ( | 10 (33.3%) | 7 (23.3%) | |
| Common ( | 0 (0%) | 0 (0%) | |
| Unsatisfactory ( | 0 (0%) | 0 (0%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Tracheal and airway disorders · Anesthesia and Sedative Agents
1 Introduction
Since its invention in 1983, the laryngeal mask airway (LMA) has become a cornerstone in anesthesia practice (1, 2). As a supraglottic airway device, the LMA enables ventilation without tracheal intubation (3), and it is now recommended in standard practice guidelines for routine airway management (4). The LMA is widely used in clinical anesthesia, emergency care, and intensive care unit settings (5).
Compared with tracheal intubation, LMA insertion is simpler, faster to learn, and associated with fewer complications (6–8). According to the American Society of Anesthesiologists (ASA) guidelines, LMA insertion has become an important tool for managing difficult ventilation (9). Studies have indicated that when laryngoscope intubation fails, LMA insertion can be performed to restore ventilation and maintain oxygenation (10, 11).
However, traditional LMAs are unreliable. For instance, challenges like mispositioning due to body movement, as well as air leakage (usually indicated by indirect evidence, such as changes in tidal volume or an audible gas leak) and other complications, have been reported (12). Severe displacement increases the risk of gastric reflux, aspiration, and trauma (13–15); therefore, displacement should be avoided.
Recently, video LMAs (V-LMAs) have been introduced, which provide real-time feedback during LMA insertion, allowing immediate positional adjustments (16). However, it remains to be clarified whether there is a difference in the placement success rate between traditional non-video LMAs (NV-LMAs) and V-LMAs. Broader adoption of V-LMAs could expand their use beyond anesthesiologists, improving timely ventilation in critical scenarios.
This study was designed to compare V-LMAs and NV-LMAs to determine which enables faster mastery by novices, has higher placement success, and causes least patient injury.
2 Methods and materials
2.1 Study design and participants
Twenty novice practitioners (resident doctors/anesthesia nurses) from the Department of Anesthesia and Perioperative Medicine, Shanghai Fourth People's Hospital, were recruited for this study. The study was approved by the institutional ethics committee (approval number 2022165-001) and has been registered in the Chinese Clinical Trial Registry (ChiCTR2300069399; 15 March 2023). Informed consent was obtained from all patients.
All practitioners had no prior LMA insertion experience. The practitioners were randomized 1:1 to two groups: (1) the V-LMA group and (2) the NV-LMA group, using a random number table. Sixty patients were also randomized 1:1 to the V-LMA group and the NV-LMA group using a random number table through the allocation manager, who stored the randomization table. The patients were informed preoperatively that they would be randomly assigned to either group, but they were blinded to the group allocation. The independent statisticians were also blinded, solely analyzing LMA efficacy without knowing any allocation information. The randomization numbers were only provided to a specific nurse who was not involved in the data analysis. Therefore, the grouping information was known only by the allocation manager, the specific nurse, anesthesiologists, surgeons, and data collectors.
2.2 Inclusion and exclusion criteria
The patient inclusion criteria were (1) ASA physical status classification I–II; (2) aged 18–70 years; (3) cardiac function class I–II; (4) body mass index (BMI) 18–25 kg/m^2^; (5) surgical duration < 3 h; and (6) voluntary provision of informed consent. The patient exclusion criteria were (1) abnormal airway anatomy (mouth opening < 3.0 cm, thyromental distance < 6.5 cm, micrognathia, Mallampati classification ≥3); (2) maxillofacial surgery, prone/beach chair position, or one-lung ventilation; (3) high reflux and aspiration risk; (4) throat pain or discomfort; (5) obstructive lung disease (asthma, chronic obstructive pulmonary disease, etc.); and (6) significant dental abnormalities (loose teeth, severe misalignment).
2.3 Research procedures
Under the supervision of the senior anesthesiologist, the practitioners in the V-LMA group received training on visual insertion techniques, while the practitioners in the NV-LMA group learned regular intubation laryngeal mask insertion techniques.
After the training, the practitioners performed supervised insertions on elective surgery patients under general anesthesia. The learning outcomes and patient injuries during insertion were analyzed. The study flow diagram is summarized in Figure 1.
Flow diagram.
2.3.1 Preparation before clinical practice
Novice practitioners (anesthesia doctors/nurses with no prior LMA insertion experience) underwent structured preparation by studying glottic anatomy and insertion protocols; reviewing instructional videos; observing mentors perform three supervised insertions; and practicing on simulation mannequins until achieving three consecutive successful insertions. The mentors were senior anesthesiologists with ≥5 years of LMA insertion expertise.
2.3.2 Clinical practice implementation
Each practitioner performed laryngeal mask insertion on three patients randomly in each group. Prior to the induction of anesthesia, all patients underwent standard monitoring (electrocardiogram, pulse oximetry, and non-invasive blood pressure monitoring every 3 min [every 1 min during anesthetic induction]). Pre-oxygenation with 100% oxygen (5 L/min) was performed for 5 min. The induction agents included intravenous propofol (1.50 mg/kg), sufentanil (0.40 μg/kg), and rocuronium (0.6 mg/kg). The LMA was inserted 5 min after the induction of anesthesia using a single-person technique and inflated to 50 cmH_2_O using a pressure gauge. Ventilation was initiated after confirming bilateral breath symmetry, two consecutive partial pressure of end-tidal carbon dioxide (PETCO_2_) waveforms, and the absence of oropharyngeal leakage. The mechanical ventilation parameters included oxygen flow at 2.0 L/min, tidal volume of 7 mL/kg, and respiratory rate of 12 breaths/min. Successful insertion required bilateral chest excursion, clear lung sounds, PETCO_2_ waveform, and no leakage. Failed insertion after three attempts prompted endotracheal intubation. Maintenance of anesthesia was achieved using propofol (4–12 mg/kg/h) and remifentanil (0.05–2.00 μg/kg/min) until completion of surgery. Fiberoptic bronchoscopy grade was defined as follows (17, 18): Grade 1: visualization of the glottis; Grade 2: visualization of the glottis and the lingual surface of the epiglottis; Grade 3: visualization of the glottis and the laryngeal surface of the epiglottis; Grade 4: no glottis visible. Data collection commenced from this point.
2.3.3 Laryngeal mask size selection
The SaCo VLM (Zhejiang U-Yue Medical Equipment Co. Ltd.) was used for V-LMA, while the Proseal Laryngeal Mask (Henan Tuoren Medical Equipment Co. Ltd.) was used for NV-LMA. The mask size was determined based on the patient's weight, as follows: Size 3: 30–50 kg; Size 4: 50–70 kg; Size 5: ≥70 kg.
2.4 Outcomes
2.4.1 Primary outcome
The primary outcome was the first-attempt insertion success rate.
2.4.2 Secondary outcomes
The secondary outcomes were the (1) time to successful insertion; (2) fiberoptic bronchoscopy grade (19); (3) frequency of in situ adjustments and reinsertions; (4) rate of conversion to endotracheal intubation; (5) patient's blood pressure and heart rate at specified time points (before anesthesia induction [T0], 1 min [T1] and 2 min [T2] after induction, immediately after LMA insertion [T3], 1 min after LMA insertion [T4], 2 min after LMA insertion [T5], and 3 min after LMA insertion [T6]); (6) incidence of postoperative throat complications within 24 h; (7) visible bleeding during LMA removal; and (8) patient and instructor satisfaction.
2.5 Statistical analysis
As this is a pilot study and represents the first attempt of its kind in this field, there were no previously published studies or pilot data available to inform a precise effect size estimate (such as a difference in proportions or hazard ratio). Therefore, our sample size was not determined by a traditional statistical power calculation but was primarily based on clinical practicality and the study's exploratory goals. The study specifically recruited novice LMA operators. A total of 20 eligible beginners were enrolled, and all were included in the analysis. Finally, 30 patients were included in each group. The statistical analysis was performed using SPSS 25.0 software. Continuous variables are expressed as the mean ± standard deviation and were analyzed using the independent-samples t-test. Categorical variables are presented as percentages and were compared using the chi-square test. P < 0.05 was considered statistically significant.
3 Results
3.1 Baseline characteristics
Overall, 60 patients were analyzed; there were no dropouts (Figure 1). The learner–instructor ratio was 2:8 in the V-LMA group and 1:9 in the NV-LMA group, with no statistically significant difference between the two groups. Baseline demographics, including age, BMI, and sex distribution, also showed no significant differences between the two groups (Table 1).
3.2 Primary outcome
Both groups achieved 100% first-attempt insertion success with no cases of conversion to endotracheal intubation.
3.3 Secondary outcomes
3.3.1 Time to successful insertion and bronchoscope grade
The average time to successful insertion was 17.77 ± 7.29 s in the V-LMA group and 14.57 ± 6.79 s in the NV-LMA group, showing no statistically significant difference (P = 0.084; Table 2). In the V-LMA group, 90% of patients achieved bronchoscope grade 1 compared with only 50% in the NV-LMA group (P = 0.001). Correspondingly, fewer in situ adjustments were required in the V-LMA group (10% vs. 50%, P = 0.003).
3.3.2 Mean arterial pressure and heart rate
The mean arterial pressure was higher in the V-LMA group than in the NV-LMA group at T3 (84.63 ± 7.05 mmHg vs. 78.77 ± 5.17 mmHg, P = 0.001) (Figure 2). At T5 and T6, the mean arterial pressure was significantly lower in the V-LMA group than in the NV-LMA group (88.67 ± 8.05 mmHg vs. 92.00 ± 4.09 mmHg, P = 0.049, and 88.27 ± 6.88 mmHg vs. 92.33 ± 5.00 mmHg, P = 0.011, respectively). The V-LMA group had smaller fluctuations in mean arterial pressure than the NV-LMA group. Figure 3 shows significant differences in heart rate at different time points. At T4, T5, and T6, heart rate in the V-LMA group was significantly lower than in the NV-LMA group (T4: 69.67 ± 7.82 bpm vs. 80.20 ± 6.29 bpm, P < 0.001; T5: 71.03 ± 7.53 bpm vs. 80.20 ± 4.66 bpm, P < 0.001; T6: 71.3 ± 7.97 bpm vs. 80.83 ± 3.83 bpm, P < 0.001).
*Mean arterial pressure at different time points in the V-LMA and NV-LMA groups. P < 0.05 compared with the NV-LMA group. NV-LMA, non-video laryngeal mask airway; V-LMA, video laryngeal mask airway.
*Heart rate at different time points in the V-LMA and NV-LMA groups. *P < 0.001 compared with the NV-LMA group. NV-LMA, non-video laryngeal mask airway; V-LMA, video laryngeal mask airway.
3.3.3 Postoperative throat complications within 24 h
No severe complications (nausea, vomiting, or hoarseness) occurred within 24 h postoperatively. Blood stains on the LMA surface were observed in 20% of the patients in the V-LMA group and in 26.7% of the patients in the NV-LMA group (P = 0.542; Table 3). The incidence of postoperative throat pain at 1 h was significantly lower in the V-LMA group (20% vs. 46.7%, P = 0.028), although there was no significant difference at 24 h (56.7% vs. 63.3%, P = 0.598). The Visual Analog Scale (VAS) scores of patients with throat pain at 1 h postoperatively were all < 3. At 24 h postoperatively, there were three patients with VAS scores ≥3 in the V-LMA group compared with six in the NV-LMA group (P = 0.278).
3.3.4 Patient and instructor satisfaction
There were no cases of general dissatisfaction or dissatisfaction among the patients or the instructors in either group (Table 4). In terms of patient satisfaction, the “very satisfied” rate was 73.3% in the V-LMA group and 80% in the NV-LMA group, while the “satisfied” rate was 26.7% and 20%, respectively (P = 0.542). Among the instructors, the “very satisfied” rate was 66.7% in the V-LMA group and 76.7% in the NV-LMA group, while the “satisfied” rate was 33.3% and 23.3%, respectively (P = 0.390).
4 Discussion
In recent years, the widespread application of LMAs in clinical practice, particularly in cases of difficult airway management (20–22), underscores the need to expand training beyond anesthesiologists. This study highlights the benefits of V-LMAs over traditional NV-LMAs in novice training, demonstrating higher placement accuracy, reduced complications, and enhanced hemodynamic stability among patients.
Second-generation LMAs provide numerous advantageous features; however, their optimal placement depends on accurate estimation of both LMA size and insertion depth. Anesthesiologists usually depend on a series of subjective indirect assessments and tests (23–25). According to one study, even when there are no clinical signs of air leakage, only 33% of patients have ideally positioned LMAs during blind insertion (26). Other scholars have compared blind insertion with LMA insertion under laryngoscope guidance. While the success rate of LMA insertion was close to 100% with both methods, the probability of achieving an ideal position was only 42% in the blind insertion group (27). In contrast, V-LMA insertion enables real-time visualization, allowing operators to dynamically adjust the positioning, achieving a glottic alignment rate of 94% (28). Additionally, operators can monitor the glottis and its surrounding area during the entire surgical procedure. Therefore, V-LMAs offer significant advantages in airway management.
In previous studies, the first-attempt success rate of SaCo VLM insertion was 91.4%−95%, higher than the rate of 77%−88% reported for traditional LMAs (18, 19, 29–33). In the present study, both groups achieved a first-attempt success rate of 100%. The first-attempt success rate in the V-LMA group was approximate to previous studies because the anesthesiologists were experienced in the use of SaCo VLM. In previous studies, no muscle relaxants were used before LMA insertion, which may have led to the lower first-attempt success rate than observed in our study.
The V-LMA group demonstrated significantly better bronchoscope alignment than the NV-LMA group (Grade 1: 90% vs. 50%, P = 0.001), consistent with a previous trial showing 91.4% accuracy for SaCo VLM vs. LMA Supreme (29). In previous studies, 40%−60% of the blindly intubated laryngeal masks did not achieve perfect positioning with a broncho-fiberscope, requiring realignment to improve ventilation (26, 34).
The reported incidence of postoperative throat pain can be as high as 70.6% (35–39). In the present study, the incidence of throat pain 1 h after the procedure was 20%, while it was 56.7% at 24 h after the procedure, markedly lower than reported previously. Potential causes of throat pain include deep LMA placement, epiglottis folding, violent blind insertion owing to poor visualization of the oral cavity, LMA material, and LMA oversizing. In the present study, patients in both groups experienced varying degrees of throat pain postoperatively, but the incidence was lower than reported in the literature, and the NV-LMA group had a higher rate than the V-LMA group. This may be related to the use of non-steroidal anti-inflammatory drugs during surgery, instructor guidance during LMA placement, controlled LMA pressure during surgery, and timely improvements in cases of misalignment or deep placement.
Two studies on NV-LMAs have reported blood stains on the LMA after removal in 7%−10% of patients (40, 41). In the present study, the incidence of blood stains on the LMA surface after removal was 26.75% in the NV-LMA group and 20% in the V-LMA group, higher than in previous studies. This may be related to the inexperience of the novice operators, insufficiently gentle LMA removal, or the LMA material. The lower incidence in the V-LMA group may be due to the operators having a better sense of direction during insertion under direct visualization.
Although the insertion time tended to be longer in the V-LMA group, there was no statistically significant difference when compared with the NV-LMA group. This is logical as novices in the V-LMA group took more time to assess the oral cavity structure and insertion path during the learning phase than those in the NV-LMA group who relied on blind insertion based on experience.
Hemodynamic analysis during LMA insertion showed that changes in patient hemodynamics after LMA insertion were within 20% of baseline values in both groups, indicating that the LMA is a safe and reliable method for airway management in terms of maintaining hemodynamic stability. Additionally, despite the longer insertion time in the V-LMA group, mean arterial pressure and heart rate were more stable before and after insertion. Direct visualization likely mitigated excessive tissue manipulation, reducing sympathetic stimulation.
The high rates of satisfaction among patients and instructors in both groups aligns with the low complication rates in this study, and there were no statistically significant differences in satisfaction between the two groups.
4.1 Limitations
This study had several limitations that should be considered when interpreting the findings. First, this was a single-center study with a small sample size. Therefore, large multicenter studies will be needed in the future to validate the findings. Second, LMA size was determined according to the patient's weight, without accounting for sex-specific anatomical variations (42). Third, the absence of initial learning-phase metrics (e.g., early failure rates) on manikins during learning phase limited a comprehensive evaluation of skill acquisition. Forth, this study was designed as a pilot and not powered to detect statistically significant differences between groups. Finally, as the novices were not blinded, potential assessment bias may exist. In the future, large multicenter studies are needed to validate the learning outcomes of V-LMA.
5 Conclusion
In summary, the V-LMA enhanced placement accuracy through real-time visualization, enabling immediate adjustments and reducing complications, such as postoperative throat pain and hemodynamic instability. These advantages make the V-LMA particularly suitable for novice practitioners and improve patient safety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jannu A Shekar A Balakrishna R Sudarshan H Veena GC Bhuvaneshwari S. Advantages, disadvantages, indications, contraindications and surgical technique of laryngeal airway mask. Arch Craniofac Surg. (2017) 18:223–9. 10.7181/acfs.2017.18.4.22329349045 PMC 5759658 · doi ↗ · pubmed ↗
- 2Brain AI. The laryngeal mask–a new concept in airway management. Br J Anaesth. (1983) 55:801–5. 10.1093/bja/55.8.8016349667 · doi ↗ · pubmed ↗
- 3Ramesh S Jayanthi R. Supraglottic airway devices in children. Indian J Anaesth. (2011) 55:476–82. 10.4103/0019-5049.8987422174464 PMC 3237147 · doi ↗ · pubmed ↗
- 4Bein B Scholz J. Supraglottic airway devices. Best Pract Res Clin Anaesthesiol. (2005) 19:581–93. 10.1016/j.bpa.2005.08.00516408535 · doi ↗ · pubmed ↗
- 5Van Zundert AAJ Kumar CM Van Zundert T Gatt SP Pandit JJ. The case for a 3rd generation supraglottic airway device facilitating direct vision placement. J Clin Monit Comput. (2021) 35:217–24. 10.1007/s 10877-020-00537-432537697 PMC 7293959 · doi ↗ · pubmed ↗
- 6Heidegger T Gerig HJ. Algorithms for management of the difficult airway. Curr Opin Anaesthesiol. (2004) 17:483–4. 10.1097/00001503-200412000-0000417031079 · doi ↗ · pubmed ↗
- 7Schäuble JC Heidegger T. Management of the difficult airway: overview of the current guidelines. Anaesthesist. (2018) 67:725–37. 10.1007/s 00101-018-0492-830291405 · doi ↗ · pubmed ↗
- 8Furman WR. Hagberg and Benumof's Airway Management. 4th ed, New York: Elsevier Health Sciences. (2018). 10.1213/ANE.0000000000003475 · doi ↗