Urgent Need to Focus on Gender‐Diverse Adolescents in Mental Health Prevention Research: A Cross‐Sectional Comparative Study
Sabrina Mittermeier, Sarah Franke, Linda M. Bonnekoh, Georg Romer, Marcel Romanos, Nikolaus Kleindienst, Arne Buerger

TL;DR
Gender-diverse adolescents face higher mental health risks like depression and self-harm compared to their cisgender peers, highlighting the need for targeted prevention strategies.
Contribution
This study provides direct comparative evidence of mental health disparities in gender-diverse adolescents using school-based data.
Findings
Gender-diverse adolescents showed significantly higher emotional dysregulation and depressive symptoms than both female- and male-identifying peers.
Recent suicidality and non-suicidal self-injury were more severe in gender-diverse youth compared to both comparison groups.
Lifetime suicidality did not differ significantly, but NSSI behaviors were more frequent and varied in gender-diverse adolescents.
Abstract
Gender‐diverse adolescents—those whose gender identity differs from their assigned sex at birth or who do not conform to traditional binary gender norms—are at significantly higher risk for mental health issues, including suicidality and non‐suicidal self‐injury (NSSI). However, most prevention efforts remain focused on cisgender youth. This study aims to directly compare levels of emotional dysregulation, depressive symptoms, suicidality, and NSSI between gender‐diverse adolescents and their cisgender peers to inform gender‐sensitive prevention strategies. This cross‐sectional analysis was conducted in a school‐based sample with participants aged 8–15 years. Gender identity was self‐reported through self‐categorization using a single item with three response options (female, male, diverse). Emotional dysregulation (DERS‐SF), depressive symptoms (PHQ‐9), suicidality (PSS), and NSSI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
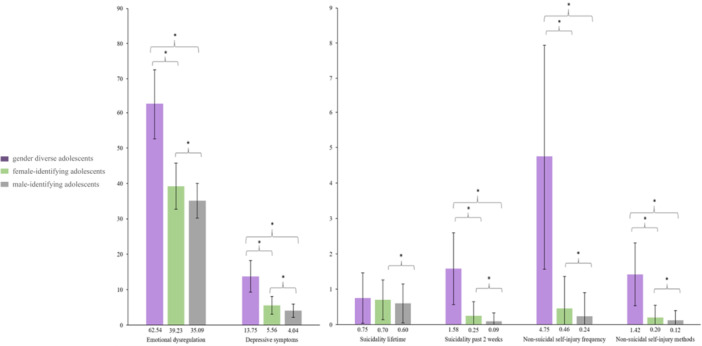 Figure 1
Figure 1- —This study von funded by Kaufmaennische Krankenkasse (KKH), Prevention and self‐help department, Tobias Bansen, Karl‐Wiechert‐Allee 61, 30625 Hannover, Germany.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent Sexual and Reproductive Health · Gender Roles and Identity Studies · Sex and Gender in Healthcare
Introduction
1
Gender diversity encompasses a spectrum of individual experiences of one's gender that may not necessarily partially or fully align with sex assigned at birth, representing an umbrella term for various subjective gender experiences that extend beyond conformity to traditional societal gender norms [1]. Gender adolescents show alarmingly high levels of suicidality [2, 3, 4]. But most suicide prevention measures are targeted at female‐identifying and male‐identifying adolescents. In a previous study on emotional dysregulation (EmD), non‐suicidal self‐injury (NSSI), and suicidality in a representative sample of n = 2350 high school students (aged 11–14 years), we emphasized the importance of gender‐dependent foci for future prevention measures [5]. However, due to the limited number of gender‐diverse adolescents in our sample (n = 13), we had to exclude them from our suicide risk model, as we could not meaningfully include them in our statistical model without potentially causing bias through forced binary gender categorization.
It is important to gather data from adolescents who identify as gender‐diverse, as these adolescents are known to be a high‐risk group not only for suicidality but also for mental health problems and poorer quality of life in general [6, 7, 8]. Moreover, adolescence is a highly sensitive phase in the development of gender identity [2]. Such data should shed light on the urgent need for targeted prevention measures for gender‐diverse adolescents and foster awareness both among clinicians and the public. This short communication aims to expand the current evidence on psychopathological distress—particularly regarding depression, suicidality, and non‐suicidal self‐injury—in gender‐diverse adolescents. In doing so, we seek to promote gender‐sensitive prevention research and to support the development and implementation of preventive interventions that meet the specific needs of gender‐diverse youth.
Methods
2
The present cross‐sectional data were collected as part of a school‐based universal prevention study on emotion regulation in adolescents, called DUDE (“DUDE—Du und deine Emotionen/You and your emotions”); for details, see [5]. The adolescents were aged between 8 and 15 years (gender diverse: M = 12.34, SD = 1.19; female‐identifying: M = 12.31, SD = 0.69; male‐identifying: M = 12.43, SD = 0.72; see Table S1 in the supporting information). Informed consent was obtained from all participants and from their legal guardians. Participants' gender identity was recorded based on self‐disclosure (response options: male, female, gender diverse). EmD was assessed using the 18‐item Difficulties in Emotion Regulation Scale–Short Form (DERS‐SF), with higher sum scores reflecting higher EmD. To assess depressive symptoms, we employed the nine‐item Patient Health Questionnaire (PHQ‐9); items refer to the past 2 weeks, and higher scores reflect greater depressive symptom severity. We further assessed suicidality using the five‐item Paykel Suicide Scale (PSS), which measures the severity of suicidality, encompassing thoughts of death, suicidal ideation, and suicide attempts, referring to the past 2 weeks and lifetime; higher scores reflect more severe suicidality. Finally, we assessed possible NSSI using the nine‐item Deliberate Self Harm Inventory (DSHI‐9), which measures lifetime prevalence, frequency, and methods of NSSI. All questionnaires employed in this study have been validated and are frequently used in mainly female‐/male‐identifying adolescents worldwide [5].
Sum scores were calculated for all questionnaires, and incomplete questionnaires were excluded from the analyzes. Due to different group sizes and a lack of normal distribution of the data, we performed two‐sided Mann‐Whitney U tests, Fisher's exact tests, and χ² tests for group comparisons and report Bonferroni‐adjusted p‐values with the a priori significance level of α < 0.05. We performed direct pairwise Mann‐Whitney U tests rather than a Kruskal‐Wallis omnibus test due to the extreme group size imbalance (gender‐diverse n = 13 vs. comparison groups n > 1000), which would severely reduce test power for detecting differences involving the small group and compromise the chi‐square approximation reliability. This analytical approach extends our previously published framework [5], where we established separate models for emotional dysregulation and suicide risk in female‐identifying and male‐identifying adolescents. The pairwise comparisons allow us to specifically examine how gender‐diverse adolescents compare to each comparison group, informing whether they align with existing models or require separate theoretical consideration. Bonferroni correction was applied to control for multiple testing. All descriptive analyzes were conducted using R Studio (version R 4.1.2).
The DUDE study was ethically approved by both the ethics committee in Wuerzburg (127/19‐me) and the Ministry of Education and Cultural Affairs (IV.7‐BO5106/200/12).
Results
3
Group comparisons between gender‐diverse (d) and female‐identifying (f) and male‐identifying (m) adolescents showed significant differences in EmD (d vs. f: U = 2488.0, p < 0.001; d vs. m: U = 1556.6, p < 0.001), depressive symptoms (d vs. f: U = 3064.0, p < 0.001; d vs. m: U = 2267.5, p < 0.001), suicidality in the past 2 weeks (d vs. f: U = 3931.0, p < 0.001; d vs. m: U = 3333.0, p < 0.001), NSSI frequency (d vs. f: U = 3748.0, p < 0.001; d vs. m: U = 3366.5, p < 0.001), NSSI methods (d vs. f: U = 3823.0, p < 0.001; d vs. m: U = 3424.0, p < 0.001), and NSSI lifetime prevalence (d vs. f: p < 0.001; d vs. m: p < 0.001).
Only with regard to lifetime suicidality did no significant differences emerge between gender‐diverse and female‐identifying and male‐identifying adolescents. All comparisons are displayed in Figure 1. For details, see also Table S1 in the supporting information.
*Means of emotional dysregulation, depressive symptoms, suicidality lifetime, suicidality past 2 weeks, non‐suicidal self‐injury frequency, and non‐suicidal self‐injury methods for gender‐diverse, cisgender female and cisgender male adolescents. indicates significant group comparisons with p < 0.05. Error bars represent standard deviation of the mean (SD). The colors of the bar plots reflect the group affiliation of the participants: gender‐diverse adolescents (purple), female‐identifying adolescents (green), male‐identifying adolescents (gray).
Discussion
4
Our analyzes revealed significantly higher levels of EmD, depressive symptoms, NSSI lifetime prevalence and frequency, and significantly more NSSI methods in gender‐diverse adolescents compared to their female‐identifying and male‐identifying peers. Although lifetime suicidality did not differ between the groups, gender‐diverse adolescents reported significantly higher levels of suicidality in the past 2 weeks compared to female‐identifying and male‐identifying adolescents.
Our data are consistent with previous research suggesting that gender‐diverse adolescents are a high‐risk group for mental health problems compared to their cisgender peers [9]. Despite this vulnerability, gender‐diverse youth remain underrepresented in prevention research and have received limited attention in early detection and intervention efforts [10]. While some promising approaches exist—such as digital interventions that provide safe spaces for identity exploration [11] and programs emphasizing intersectional youth rights approaches [12]—evidence‐based prevention measures specifically tailored to gender‐diverse adolescents remain scarce.
Implications for Prevention
4.1
The elevated symptom burden observed in gender‐diverse adolescents necessitates both universal and targeted prevention approaches. Universal strategies should incorporate comprehensive mental health literacy programs and school‐based anti‐bullying interventions, given the higher victimization rates among sexual and gender minority youth [13]. Targeted interventions require gender‐specific modules addressing minority stress processes, including coping with discrimination and internalized stigma [8].
However, implementation faces substantial barriers. Structural challenges include healthcare access limitations, provider discrimination, and inadequate training for school personnel [14]. Additionally, while isolated progress has been made in validating some screening instruments across gender identities [15], screening measures validated for gender‐diverse adolescent populations are still scarce. These barriers are compounded by data security concerns, particularly regarding involuntary disclosure risks in electronic health records when collecting sensitive gender identity information [16].
Strengths and Limitations
4.2
The limitations include the small number of gender‐diverse adolescents and the cross‐sectional design, which precludes causal conclusions. Further, the questionnaires were predominantly developed and normed using female‐identifying and male‐identifying samples, which is why only isolated data points are available for gender‐diverse adolescents (DSHI [17]; PSS [18]; DERS [19]. Although the PHQ‐9 has been administered to gender‐diverse adolescents, no validation studies or normative values exist for this population either [20], limiting comparability with other studies. Moreover, gender identity was assessed using a single questionnaire item with three response options (male, female, diverse), which presents several important limitations. This approach does not provide insight into specific gender identities such as transgender or nonbinary. More critically, some binary transgender adolescents may have selected “male” or “female” in alignment with their gender identity and were consequently misclassified as cisgender, potentially leading to underrepresentation of gender‐diverse participants and measurement bias. To account for this limitation, we use the terms “male‐identifying” and “female‐identifying” adolescents throughout this study rather than assuming cisgender identity. Additionally, this limited assessment approach restricts our understanding of minority stressors related to gender diversity (e.g. stigmatization, rejection [21]. The generalizability of our findings is inherently limited to school‐enrolled adolescents and does not extend to out‐of‐school youth or clinical populations, who may differ systematically in mental health outcomes. Nevertheless, the questionnaire approach also represents an advantage, as adolescents may be more likely to disclose their gender identity via questionnaire than during an interview. Taken together, however, we do not believe that these limitations question the essence of our findings, that is, strongly increased symptom severity in several clearly defined areas of psychopathology, including emotional dysregulation, suicidality, depressiveness, and NSSI.
Future Perspectives
4.3
Moving forward, three critical research priorities emerge. First, developing and validating gender‐sensitive assessment instruments specifically normed for gender‐diverse adolescents is essential for accurate identification of mental health needs and treatment outcomes. Second, longitudinal studies examining protective and risk factors unique to gender‐diverse youth trajectories will inform more effective prevention and intervention timing and targets. Finally, adapting established prevention measures through participatory approaches that actively involve gender‐diverse youth in program development will ensure interventions are culturally relevant and acceptable to this population. Such inclusive research will provide the foundation for prevention programs that consider the full spectrum of gender experiences, ultimately ensuring all young people have equitable opportunities for improved mental health outcomes.
Conclusion
5
The inclusion of adolescents identifying as gender diverse in research will lay the foundation for determining suitable approaches for prevention measures and developing future prevention programs that consider the variety of gender non‐conforming and gender‐diverse youth, thus giving all young people the same opportunities for improved mental health.
Author Contributions
Sabrina Mittermeier: conceptualization, writing – original draft, writing – review and editing, data curation, formal analysis, visualization. Sarah Franke: conceptualization. Linda M. Bonnekoh: validation, writing – review and editing. Georg Romer: validation. Marcel Romanos: funding acquisition. Nikolaus Kleindienst: conceptualization, methodology, validation. Arne Buerger: conceptualization, supervision, funding acquisition, project administration, writing – review and editing.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author Sabrina Mittermeier affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Supporting information
Supporting Tables 1: Sample characteristics and group comparisons of gender‐diverse and female‐/male identifying adolescents.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. Hines and M. Taylor , Is Gender Fluid?: A Primer for the 21st Century. Thames and Hudson. 2018.
- 2S. Mezzalira , C. Scandurra , F. Mezza , M. Miscioscia , M. Innamorati , and V. Bochicchio , “Gender Felt Pressure, Affective Domains, and Mental Health Outcomes Among Transgender and Gender Diverse (TGD) Children and Adolescents: A Systematic Review With Developmental and Clinical Implications,” International Journal of Environmental Research and Public Health 20, no. 1 (2022): 785, 10.3390/ijerph 20010785.36613106 PMC 9819455 · doi ↗ · pubmed ↗
- 3L. Bochicchio , K. Reeder , L. Aronson , C. Mc Tavish , and A. Stefancic , “Understanding Factors Associated With Suicidality Among Transgender and Gender‐Diverse Identified Youth,” LGBT Health 8, no. 4 (2021): 245–253, 10.1089/lgbt.2019.0338.33904768 · doi ↗ · pubmed ↗
- 4J. L. Hughes , L. M. Horowitz , J. P. Ackerman , M. C. Adrian , J. V. Campo , and J. A. Bridge , “Suicide in Young People: Screening, Risk Assessment, and Intervention,” BMJ 381 (2023): e 070630, 10.1136/bmj-2022-070630.37094838 PMC 11741005 · doi ↗ · pubmed ↗
- 5S. Mittermeier , A. Seidel , C. Scheiner , N. Kleindienst , M. Romanos , and A. Buerger , “Emotional Dysregulation and Its Pathways to Suicidality in a Community‐Based Sample of Adolescents,” Child and Adolescent Psychiatry and Mental Health 18, no. 1 (2024): 15, 10.1186/s 13034-023-00699-4.38245793 PMC 10800042 · doi ↗ · pubmed ↗
- 6M. Röder , C. Barkmann , H. Richter‐Appelt , M. Schulte‐Markwort , U. Ravens‐Sieberer , and I. Becker , “Health‐Related Quality of Life in Transgender Adolescents: Associations With Body Image and Emotional and Behavioral Problems,” International Journal of Transgenderism 19, no. 1 (2018): 78–91, 10.1080/15532739.2018.1425649. · doi ↗
- 7L. Sares‐Jäske , M. Czimbalmos , S. Majlander , et al., “Gendered Differences in Experiences of Bullying and Mental Health Among Transgender and Cisgender Youth,” Journal of Youth and Adolescence 52, no. 8 (2023): 1531–1548, 10.1007/s 10964-023-01786-7.37199852 PMC 10276116 · doi ↗ · pubmed ↗
- 8N. M. Wittlin , L. E. Kuper , and K. R. Olson , “Mental Health of Transgender and Gender Diverse Youth,” Annual Review of Clinical Psychology 19, no. 1 p. annurev‐clinpsy (2023): 207–232, 10.1146/annurev-clinpsy-072220-020326.PMC 993695236608332 · doi ↗ · pubmed ↗