Testicular lymphoma of 63 patients: a Chinese retrospective, real-world study
Honghan Qiao, Sijun Zhang, Yukai Duan, Renjie Hua, Feiyang Zong, Mingzhi Zhang, Xudong Zhang

TL;DR
This study compares primary and secondary testicular lymphoma in 63 patients, highlighting treatment outcomes and survival differences.
Contribution
The study provides real-world clinical data on treatment strategies and survival outcomes for primary and secondary testicular lymphoma in China.
Findings
Primary testicular lymphoma (PTL) had significantly better progression-free and overall survival than secondary testicular lymphoma (STL).
Radiotherapy improved progression-free survival, while the double-expressor phenotype was linked to worse outcomes.
Combined treatment involving orchiectomy, chemotherapy, and radiotherapy is recommended for PT-DLBCL.
Abstract
To suggest the difference between primary and secondary testicular lymphoma, and to manifest the clinical characteristics, treatment modalities and prognostic factors of primary testicular lymphoma. This study included all lymphoma patients with testicular involvement treated at our institution between October 2012 and May 2024. We retrospectively collected data on their clinical characteristics, treatment approaches, and outcomes for further analysis. A total of 50 primary testicular lymphoma (PTL) patients and 13 secondary testicular lymphoma (STL) patients were enrolled, with diffuse large B-cell lymphoma (DLBCL) being the most common subtype. After a median follow-up of 36.0 months (range: 1.1–117.5), the median progression-free survival (PFS) was 105.9 months for PTL patients and 16.8 months for STL patients. The median overall survival (OS) was 106 months for PTL and 23.8 months…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
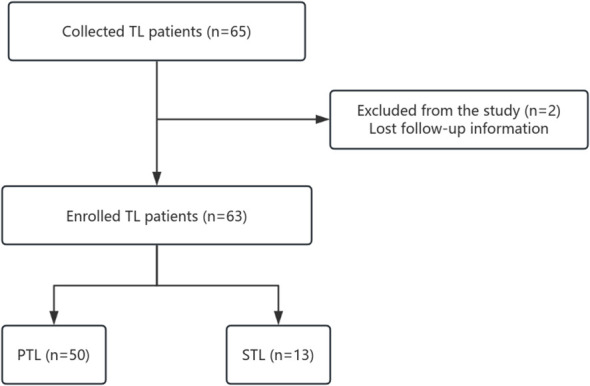 Figure 1
Figure 1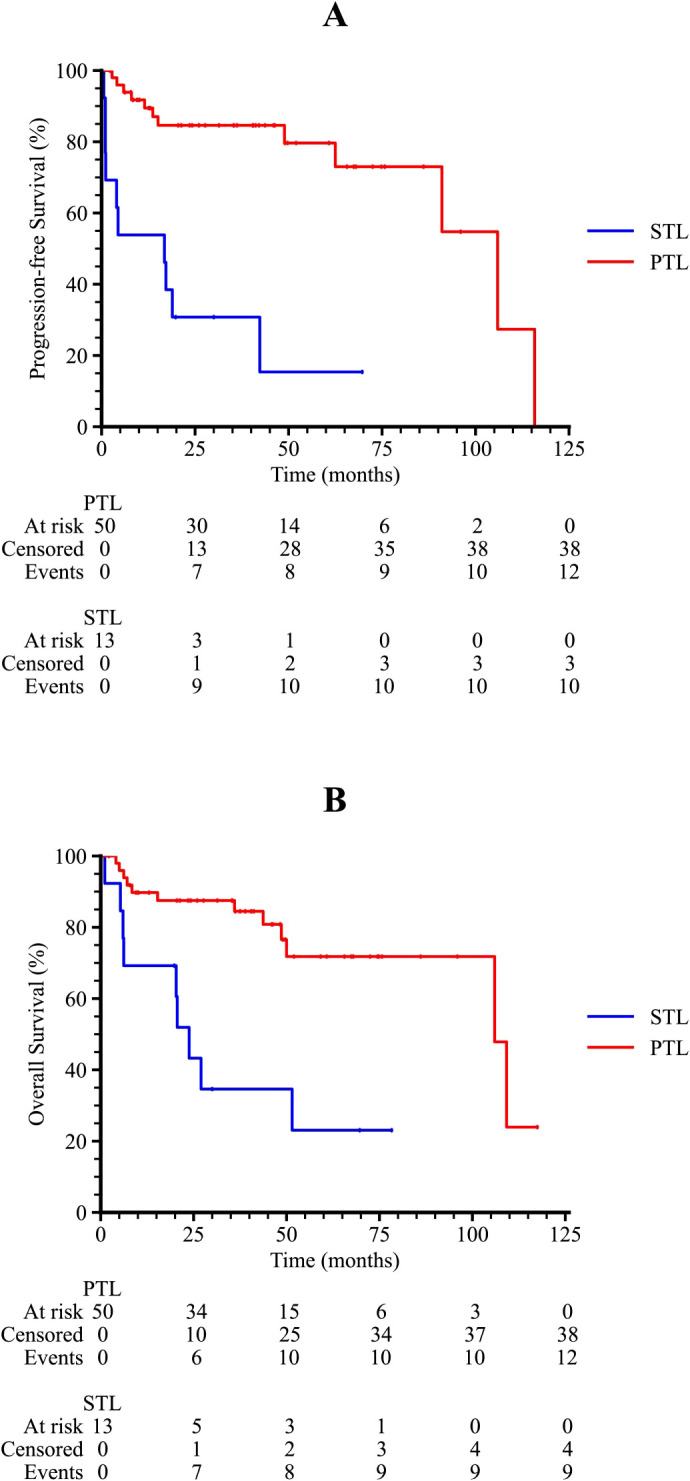 Figure 2
Figure 2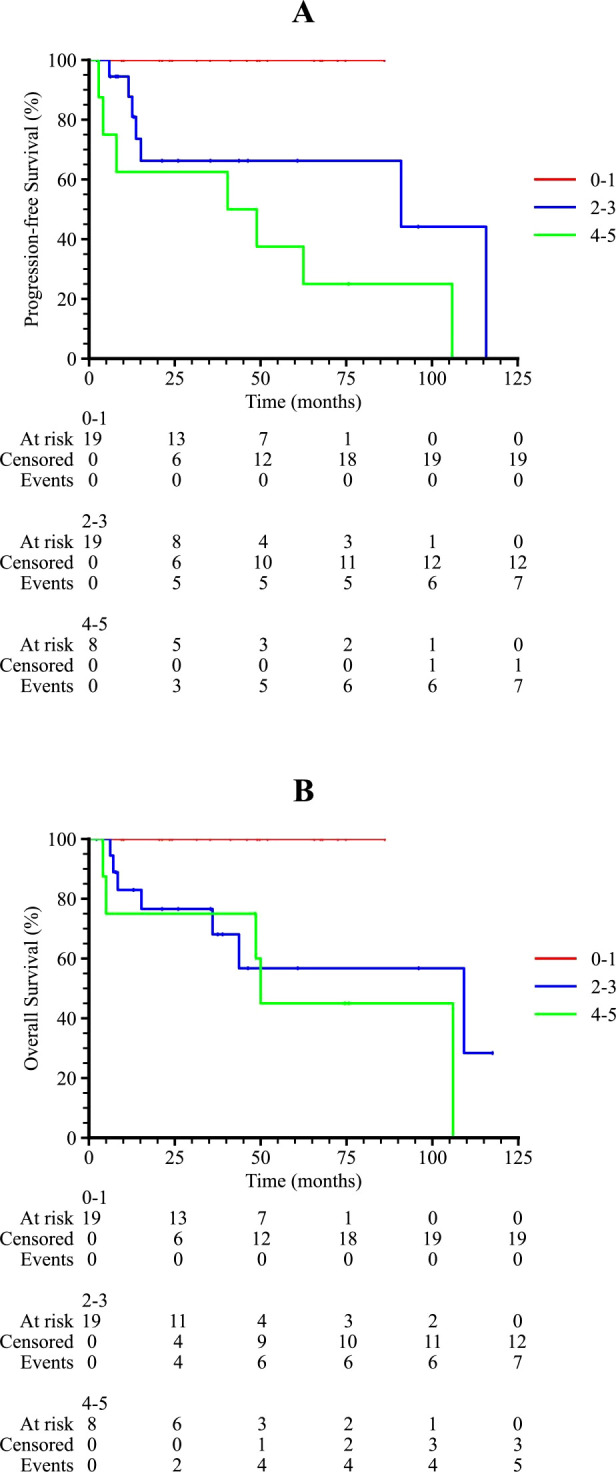 Figure 3
Figure 3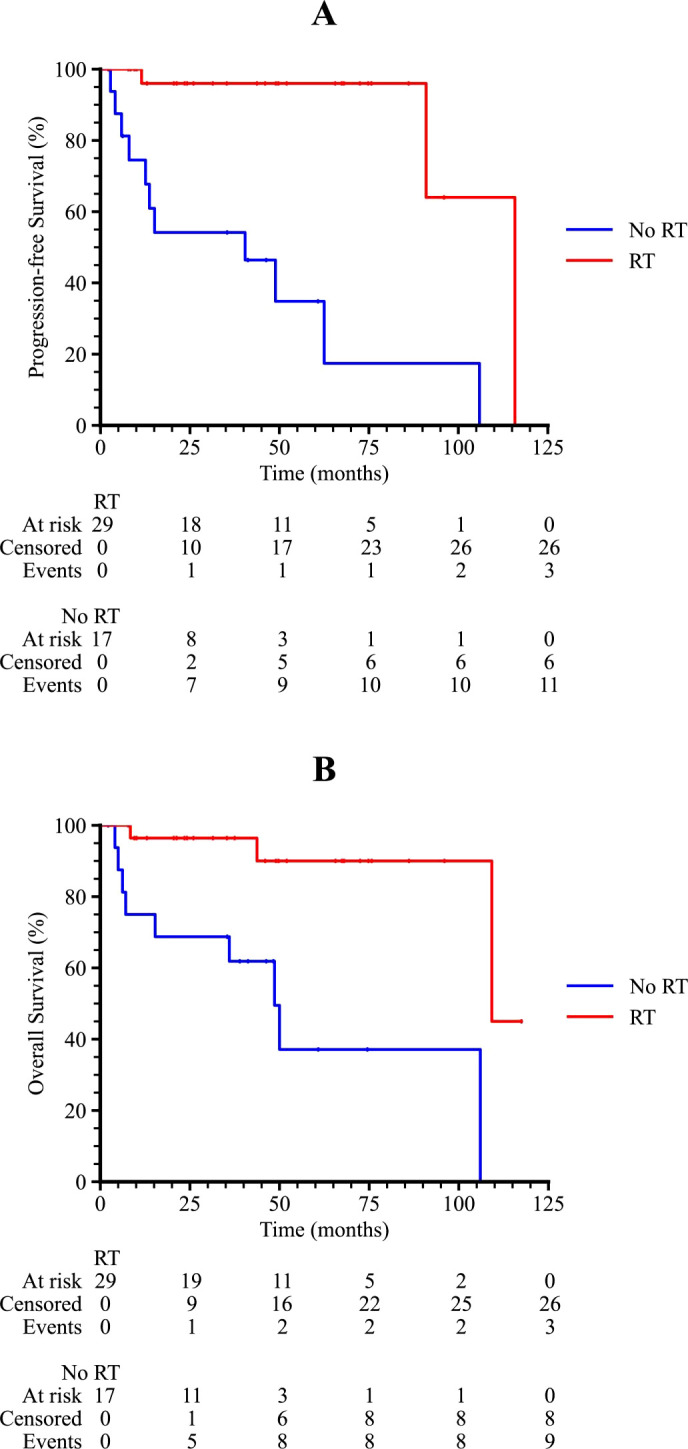 Figure 4
Figure 4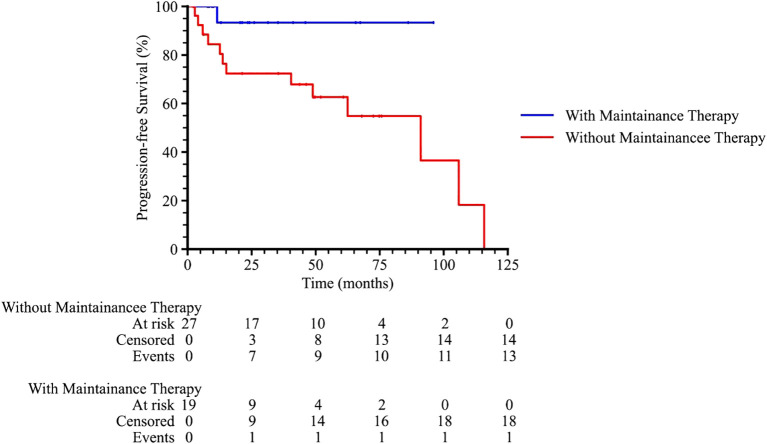 Figure 5
Figure 5| Characteristics, n (%) | PTL (n=50) | STL (n=13) |
|---|---|---|
| Age | ||
| Median (range) age, years | 64 (39-88) | 53 (29-77) |
| Disease diagnosis | ||
| DLBCL | 46 (92.0%) | 7 (53.8%) |
| Ann Arbor stage | ||
| IE | 13 (26.0%) | 0 (0.0%) |
| Location | ||
| Left | 19 (38.0%) | 3 (23.1%) |
| Extranodal involvement | ||
| Bone marrow involvement | 4 (8.0%) | 3 (23.1%) |
| Survival | ||
| Alive | 37 (74.0%) | 4 (30.8%) |
| Orchiectomy | ||
| Yes | 48 (96.0%) | 6 (46.2%) |
| First-line therapy | ||
| R-CHOP-like regimens*
| 33 (66.0%) | 7 (53.9%) |
| Radiotherapy | ||
| Yes | 29 (58.0%) | 6 (46.2%) |
| CNS prophylaxis | ||
| Yes | 31 (62.0%) | 6 (46.2%) |
| HSCT | ||
| Yes | 1 (2.0%) | 1 (7.7%) |
| CAR-T | ||
| Yes | 0 (0.0%) | 2 (15.4%) |
| Effectiveness,n (%) | Total,63 | PTL,50 | STL,13 | P value |
|---|---|---|---|---|
| ORR | 39 (61.9%) | 35 (70.0%) | 4 (30.8%) | 0.023 |
| CR | 31 (49.2%) | 29 (58.0%) | 2 (15.4%) | |
| PR | 8 (12.7%) | 6 (12.0%) | 2 (15.4%) | |
| SD | 6 (9.5%) | 5 (10.0%) | 1 (7.7%) | |
| PD | 18 (28.6%) | 10 (20.0%) | 8 (61.5%) |
| Clinical features | N (%) |
|---|---|
| Primary symptoms | 46 (100%) |
| Unilateral painless swelling | 23 (50.0%) |
| Disease status | |
| Relapse | 2 (4.3%) |
| IPI score | |
| 0-1 | 19 (41.3%) |
| CNS-IPI score | |
| 0-1 | 19 (41.3%) |
| Cell of origin | |
| Non-GCB subtype | 36 (78.2%) |
| Immunophenotype | |
| Double-expressor phenotype | 10 (21.7%) |
| Double/triple-hit phenotype | 4 (8.7%) |
| Treatment category | Regimen or approach | N (%) |
|---|---|---|
| Orchiectomy | Yes | 44 (95.7%) |
| First-line therapy | R-CHOP-like regimens | 32 (69.6%) |
| Number of first-line treatment cycles | Median (range) | 6 (0-10) |
| R as consolidation therapy | Yes | 11 (23.9%) |
| Second-line therapy | R-Gemox*
| 3 (6.5%) |
| Maintenance therapy | Lenalidomide | 7 (15.2%) |
| CNS prophylaxis | Intrathecal (IT) | 27 (58.7%) |
| Radiotherapy | Yes | 28 (60.9%) |
| IPI score, n(%) | CNS recurrence, 7 | No CNS recurrence, 39 | Total, 46 | P value |
|---|---|---|---|---|
| 0-1 | 0 (0%) | 19 (41.3%) | 19 (41.3%) | |
| 2-3 | 5 (10.7%) | 12 (26.1%) | 17 (37.0%) | |
| 4-6 | 2 (4.3%) | 8 (17.4%) | 10 (21.7%) | 0.028 |
| Variables | Univariate analysis (PFS) | Multivariate analysis (PFS) | ||
|---|---|---|---|---|
| HR | P value | HR | P value | |
| Age | ||||
| 1.09(1.02-1.15) |
| 0.96(0.86-1.07) | 0.469 | |
| Ann Arbor stage | ||||
| I-II | Ref |
| 3.45(0.17-70.08) | 0.420 |
| COO | ||||
| Non-GCB subtype | Ref | 0.916 | ||
| Laterality | ||||
| Unilateral | Ref | 0.848 | ||
| IPI score | ||||
| 2.26(1.43-3.58) |
| 1.15(0.43-3.08) | 0.782 | |
| Immunophenotype | ||||
| Double-expressor phenotype | 2.63(0.69-10.13) | 0.159 | ||
| Double-hit phenotype | 2.05(0.43-9.66) | 0.365 | ||
| First-line therapy | ||||
| No | Ref | 0.058 | 0.05(0.00-1.56) 0.45 | 0.089 |
| Maintenance therapy | ||||
| Yes | 0.15(0.02-1.17) | |||
| Radiotherapy | ||||
| Yes | 0.08(0.02-0.35) | 0.07(0.01-0.64) |
| |
| Intrathecal CNS prophylaxis | ||||
| Yes | 0.40(0.12-1.32) | |||
| Variables | Univariate analysis (OS) | Multivariate analysis (OS) | ||
|---|---|---|---|---|
| HR | P value | HR | P value | |
| Age | ||||
| 1.09(1.03-1.15) |
| 1.02(0.92-1.13) | 0.750 | |
| Ann Arbor stage | ||||
| I-II | Ref | 0.077 | ||
| COO | ||||
| Non-GCB subtype | Ref | 0.669 | ||
| Laterality | ||||
| Unilateral | Ref | 0.456 | ||
| IPI score | ||||
| 1.78(1.16-2.73) |
| 0.75(0.40-1.42) | 0.378 | |
| Immunophenotype | ||||
| Double-expressor phenotype | 6.93(1.95-24.64) |
| 10.99(2.06-58.75) |
|
| Double-hit phenotype | 3.43(0.72-16.29) | 0.121 | ||
| First-line therapy | ||||
| No | Ref | 0.104 | 0.13(0.00-4.02) | 0.241 |
| Maintenance therapy | ||||
| Yes | 0.19(0.02-1.54) | 0.120 | ||
| Radiotherapy | ||||
| Yes | 0.10(0.02-0.49) |
| 0.10(0.01-1.16) | 0.065 |
| Intrathecal CNS prophylaxis | ||||
| Yes | 0.30(0.08-1.13) | 0.075 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Multiple Myeloma Research and Treatments · Lymphoma Diagnosis and Treatment
Introduction
1
The testes are regarded as immune-privileged sites, protected by the blood-testicular barrier and immunomodulatory mechanisms. Lymphomas arising in these immune sanctuaries represent a rare subtype of non-Hodgkin lymphoma (NHL), typically associated with aggressive clinical behavior and poor prognosis. These lymphomas can be broadly categorized as either primary testicular lymphoma (PTL) or secondary testicular lymphoma (STL).
PTL is defined by the presence of testicular masses as the initial or predominant manifestation, without obvious involvement of other extranodal organs. In contrast, STL is caused by the spread of extara-testicular lymphoma. Clinically, differentiating PTL from STL can be challenging, particularly when testicular involvement is the presenting symptom. Accurate clinical staging is also crucial for determining the appropriate treatment. PTL accounts for 1% to 2% of all NHL cases and 3% to 9% of testicular malignancies. It is the most common testicular tumor in men over 60 and is associated with a high risk of contralateral testicular and central nervous system (CNS) relapse (1). The majority of PTL cases are diffuse large B-cell lymphoma (DLBCL), while STL displays more varied histopathological types.
Although the incidence of PTL is gradually increasing in China, the overall occurrence of testicular lymphoma remains significantly lower in Asian populations compared to Western cohorts. This discrepancy has resulted in a scarcity of real-world clinical data from Chinese populations. Furthermore, despite the consensus on standard PTL treatment, optimal therapeutic approaches following orchiectomy remain a subject of debate. Novel agents, such as PD-1 and Bruton’s tyrosine kinase inhibitors (BTK-i), have shown promise. In light of these issues, we conducted this retrospective study, collecting real-world data from PTL and STL patients at our center. Our aim was to compare clinical and pathological characteristics, assess the effectiveness of various treatment regimens, and evaluate survival outcomes.
Materials and methods
2
Study design and patient selection
2.1
We retrospectively collected data from 63 lymphoma patients with testicular involvement treated at the First Affiliated Hospital of Zhengzhou University between October 2012 and May 2024. Patients were categorized into two groups: primary testicular lymphoma (PTL) and secondary testicular lymphoma (STL). Procedures of patient selection are displayed in Figure 1. The classification was based on whether the testicular mass was the primary or predominant symptom and whether there was significant involvement of other extranodal organs. PTL was confirmed through testicular pathology, while testicular involvement in STL cases was evaluated using either pathology or positron emission computed tomography (PET/CT). Disease staging was conducted according to the Ann Arbor staging system. Immunohistochemistry was performed for Bcl-2 and c-Myc expression, while fluorescence in situ hybridization (FISH) was used to identify double-expressor types as well as double-hit/triple-hit DLBCL. The cell of origin (COO) of DLBCL was determined using the HANS algorithm, based on the expression of CD10, Bcl-6, and MUM-1. Clinical characteristics such as age, Ann Arbor stage, extranodal involvement, treatment regimens, and disease response were collected for further analysis. This study was approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University (2022-KY-0869-001). All the processes conformed to the Declaration of Helsinki. All patients have signed written informed consents before treatment.
Procedures of patients selection.
Treatment modalities and assessment of effectiveness
2.2
For PTL patients, orchiectomy was followed by 4 to 6 cycles of chemotherapy, CNS prophylaxis, and radiotherapy (RT). Prophylactic contralateral testicular RT or nodal RT after first-line treatment was administered with a total dose ranging from 20 to 45 grays. CNS prophylaxis was primarily carried out through intrathecal injections of methotrexate (MTX, 12–15 mg), cytarabine (AraC, 50 mg), and dexamethasone (DXM, 5 mg). Treatment response was evaluated using computed tomography (CT) or positron emission tomography/computed tomography (PET/CT). Short-term effectiveness was classified as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). The overall response rate (ORR) was defined as the percentage of patients achieving CR or PR. Overall survival (OS) was measured from the date of diagnosis to death or last observation from any cause, while progression-free survival (PFS) was defined as the time from diagnosis to the first relapse, progression, death, or last follow-up.
Statistical analysis
2.3
Descriptive statistics were expressed as percentages and medians. Treatment effectiveness was compared using the chi-squared test. Survival outcomes, including overall survival (OS) and progression-free survival (PFS), were estimated using the Kaplan–Meier method. Differences between survival curves were compared using the log-rank test. Univariate Cox proportional hazards regression models were applied to identify potential prognostic factors. Variables assessed included age at diagnosis, Ann Arbor stage, COO, laterality, IPI score, immunophenotype, first-line therapy, radiotherapy, maintenance therapy and intrathecal CNS prophylaxis. Variables with a p-value <0.05 in univariate analysis were further included in the multivariate Cox model. All statistical analyses were conducted with SPSS software version 26.0 and GraphPad Prism version 8. A p-value of <0.05 was considered statistically significant.
Results
3
Baseline characteristics, clinical response, and survival outcomes between PTL and STL patients
3.1
A total of 63 patients with testicular involvement were included in the study, consisting of 50 PTL and 13 STL patients. Comparisons between their clinical characteristics and their treatment options are depicted in Table 1. The median age (range) for PTL patients was 64 years (39–88), and for STL patients, it was 53 years (29–77). Among them, 56.0% of PTL patients and 30.8% of STL patients were over 60 years of age. All PTL cases and 6 STL cases were confirmed via testicular pathology, while the remaining 7 STL patients were assessed using FDG-PET/CT, with a mean testicular maximum standardized uptake value (SUVmax) of 12.3 (range: 5.0–21.1). The majority of patients were diagnosed with DLBCL, accounting for 92% of PTL and 53.8% of STL cases, with a statistically significant difference in pathology between the two groups (p < 0.001). Of the PTL patients, 52% (n = 26) presented with limited-stage lymphoma (stage I E and II E), while all STL patients were diagnosed at an advanced stage. Two PTL and one STL patient had a history of testicular injury, and four PTL and two STL patients had undergone testicular surgery, potentially linked to the development of testicular lymphoma. Most patients had unilateral disease, observed in 86% of PTL and 76.9% of STL patients. Bone marrow involvement was noted in four PTL (8%) and three STL (23.1%) patients, while CNS involvement occurred in seven PTL (14%) and four STL (30.8%) patients. During follow-up, 22 patients died, including four PTL and nine STL patients, with a significant difference in mortality between the groups (p = 0.01).
At a median follow-up of 36.0 months (range: 1.1–117.5), treatment response and survival outcomes were evaluated for all patients. The overall response rate (ORR) was 61.9%, with 31 patients achieving a complete response (CR) and eight patients achieving a partial response (PR). The total CR rate was 49.2% (Table 2). Among PTL patients, the ORR was 70.0%, with 58.0% achieving a CR, while in STL patients, the ORR was 30.8%, with 15.4% achieving a CR, representing a significant difference between the two groups (p = 0.023).
Kaplan-Meier survival curves of TL patients. (A) The progression-free survival curve among PTL and STL patients. (B) The overall survival curve among PTL and STL patients.
Primary testicular DLBCL
3.2
Clinical features and treatment regimens of primary testicular DLBCL
3.2.1
A total of 46 primary testicular DLBCL (PT-DLBCL) patients were enrolled in the study, representing the majority of PTL cases. The clinical characteristics and treatment modalities of these patients are summarized in Table 3. The most commonly reported primary symptom was unilateral painless swelling (50.0%), followed by testicular pain (26.1%), a combination of swelling with pain (17.4%), and the presence of a testicular mass (17.4%). Fourteen out of 46 patients (30.4%) had relapsed or refractory (R/R) disease, and 78.2% of cases were of the non-GCB subtype. MYD88 gene testing was performed on five patients, with four testing positive for the MYD88 mutation. All patients were diagnosed with DLBCL through pathological examination, with 44 out of 46 (95.7%) undergoing orchiectomy, while two patients were confirmed through testicular puncture biopsy without receiving any orchiectomy.
Detailed information on treatment regimens is summarized in Table 4. Among all patients, the majority received R-CHOP-like regimens as first-line treatment. These included R-CHOP, Rituximab with cyclophosphamide, pegylated liposomal doxorubicin, vincristine, and prednisone (R-CDOP); zanubrutinib with R-CHOP (ZR-CHOP); and lenalidomide with R-CHOP (R2-CHOP). Two patients did not receive chemotherapy after orchiectomy. After a median of four cycles of frontline treatment, 11 patients received Rituximab (R) monotherapy as consolidation therapy. Several second-line and maintenance regimens were used in relapsed or high-risk cases, including lenalidomide, thalidomide, and R-Gemox. Additionally, 28 out of 46 patients underwent radiotherapy following chemotherapy, and CNS prophylaxis was given to 28 patients (60.9%), including 27 patients with intrathecal methotrexate and 1 with intravenous methotrexate.
Contralateral testis and CNS recurrence in primary testicular DLBCL
3.2.2
Among the 46 PT-DLBCL patients, 3 (6.5%) experienced relapse in the contralateral testis, and 7 (15.2%) had central nervous system (CNS) recurrences. There was a trend toward lower contralateral testis relapse rates in patients who received prophylactic contralateral testicular radiotherapy (RT) compared to those who did not, although this difference did not reach statistical significance (p = 0.054). Similarly, the rate of CNS recurrence did not differ significantly between patients who received CNS prophylaxis (27 with intrathecal methotrexate and 1 with intravenous methotrexate) and those who did not (p = 0.900), nor did the cumulative incidence of CNS relapse (p = 0.54). The 6-month cumulative CNS relapse rates in the prophylaxis and non-prophylaxis groups were 9.5% and 8.5%, respectively, with the median time to CNS relapse among all PT-DLBCL patients being 47.3 months (range: 0.2–106.0).
Among the 7 patients with CNS recurrence, 6 had parenchymal involvement, and 1 had leptomeningeal involvement. The most commonly affected sites were the corpus callosum, basal ganglia, frontal lobe, and parietal lobe. There was no significant difference in CNS relapse rates between patients who received Rituximab and those who did not (p = 1.000). However, patients classified as low-, intermediate-, and high-risk based on CNS-IPI scores (0–1, 2–3, and 4–6, respectively) showed a statistically significant difference in CNS recurrence rates (p = 0.028 Table 5).
Survival analysis by subgroup and prognostic factors for primary testicular DLBCL
3.2.3
Subgroup analysis revealed that patients with an International Prognostic Index (IPI) score of 2–3 or 4–5 had significantly poorer survival outcomes compared to those with an IPI score of 0–1 (p = 0.001 and 0.011 for PFS and OS, respectively), as shown in Figure 3. Patients who received radiotherapy demonstrated improved progression-free survival (PFS) and overall survival (OS) (p = 0.009 and 0.001, respectively, Figure 4). The 3-year PFS rate was 93.3% for patients who received maintenance therapy after first-line treatment, compared to 72.4% for those who did not receive maintenance therapy (p = 0.037, Figure 5).
Kaplan-Meier survival curves of PTL patients in different IPI scores. (A) The progression-free survival curve among PTL patients in 0-1, 2–3 and 4–5 IPI score. (B) The overall survival curve among PTL patients in 0-1, 2–3 and 4–5 IPI score.
Kaplan-Meier survival curves of PTL patients with or without RT. (A) The progression-free survival curve among PTL patients with or without RT. (B) The overall survival curve among PTL patients with or without RT.
The progression-free survival curve among PTL patients with or without maintenance therapy.
Univariate and multivariate Cox regression analyses were performed to evaluate potential prognostic factors in PT-DLBCL patients. In the univariate analysis, age, Ann Arbor stage, IPI score, first-line therapy, and radiotherapy were identified as potential prognostic factors for PFS. For OS, age, IPI score, immunophenotype, first-line therapy, and radiotherapy were identified as possible prognostic factors. Further multivariate analysis confirmed that radiotherapy was an independent prognostic factor for PFS, while the double-expressor phenotype was an independent prognostic factor for OS in PT-DLBCL patients (Tables 6, 7).
Discussion
4
Differentiating between PTL and STL remains a significant challenge in clinical practice, impacting clinical staging, treatment planning, and prognostic evaluation. Matthew et al. proposed a stricter definition of PTL, limiting it to testicular lymphomas without lymph node or bone marrow involvement (2). Moreover, Rebecca et al. suggested that phenotypic, genetic, and biological characteristics could further assist in distinguishing these two types (3). PTL, for example, is often associated with the non-GCB subtype and the common mutations of MYD88 L265P and CD79B, although this requires further clinical validation. In our study, we differentiated PTL from systemic lymphoma disease based on clinical symptoms and extranodal involvement. Our findings demonstrate that the two groups exhibited distinct pathological features, treatment responses, and survival outcomes. However, the distinction might be correlated to diverse biological features and treatment strategies, including non-GCB phenotype, MYD88/CD79B mutations, and immune-privileged site involvement between these two groups. Current guidelines recommend that PTL diagnosis be confirmed via biopsy and pathology. Combined treatment strategies, including orchiectomy followed by chemotherapy and radiotherapy, are essential. Orchiectomy not only facilitates an accurate pathological diagnosis but also disrupts the blood-testicular barrier, enhancing the efficacy of chemotherapy. In contrast, for STL patients, diagnosis primarily depends on the intensity of FDG uptake on PET/CT (4, 5). Given the difficulty in interpreting physiologic and pathologic uptake on FDG-PET/CT, we adopted a standardized uptake value (SUVmax) threshold of 5.0 to determine testicular involvement by lymphoma, referencing a previous American study (5). 14 PTLs displayed unfavorable survival outcomes in general, however, one with NKTCL received 6 cycles of DDGP regimen as front-line and then discovered testicular involvement, after 4 cycles of etoposide, PD-1 blockade and chidamide, he received chimeric antigen receptor T-cell (CAR-T) therapy and reached a PFS of 70 months. As systemic chemotherapy has shown limited efficacy in such case, novel therapies such as stem cell transplantation and CAR-T cell therapy should be considered.
Primary testicular diffuse large B-cell lymphoma (PT-DLBCL) is the most common histological subtype of PTL, accounting for 80–90% of cases. It is characterized by a high propensity for relapse in the central nervous system (CNS), contralateral testis, and other extranodal sites (3, 6). However, Chinese real-world data on this rare and aggressive disease remain limited. In our study, we analyzed a cohort of 46 patients with PT-DLBCL, focusing on their clinical features, treatments strategies, and prognosis outcomes. This analysis reflects real-world clinical practice and provides valuable insights into the management of this uncommon lymphoma subtype. The primary symptoms of PT-DLBCL were predominantly unilateral painless swelling, and the most commonly observed phenotype was the non-GCB subtype, which aligns with previous studies (7, 8). Notably, western cohorts have shown greater molecular heterogeneity. Interestingly, half of our patients were at an advanced stage at diagnosis, a higher proportion than previously reported. This may be attributed to frequent misdiagnoses as orchitis, leading to delayed treatment.
Although MYD88 gene mutation testing is not routinely conducted in Chinese clinical practice, our study found an 80% mutation rate, consistent with the 68–82% reported in other Chinese and Asian studies (9). This mutation, frequently co-occurring with CD79B mutations, is a hallmark of the activated B-cell (ABC) or non-GCB subtype, contributing to constitutive NF-κB pathway activation and poorer outcomes. BCL2 and BCL6 mutations, which have also been implicated in extranodal DLBCL prognosis in previous studies, were not assessed in our cohort due to limited access to molecular profiling (10–12). The double- or triple-hit phenotype, commonly involving rearrangements of MYC and BCL-6, was less frequent in PT-DLBCL compared to nodal DLBCL. Similarly, the double-expressor phenotype was also less prevalent in PT-DLBCL (13), while BCL6 rearrangements, double-expressor phenotype, and even double-hit lymphomas involving MYC and BCL6 or BCL2 are reported more frequently in western countries (14).
For PT-DLBCL patients, orchiectomy alone is insufficient; combined treatment modalities are essential for improving outcomes. In the Rituximab era, R-CHOP and R-CHOP-like regimens have been the most commonly used first-line therapies, demonstrating significantly better survival compared to orchiectomy alone. Additionally, Polatuzumab vedotin—a CD79b-targeted antibody–drug conjugate—has shown enhanced efficacy when combined with R-CHP in DLBCL patients, particularly in those with the ABC (non-GCB) subtype. However, its use remains limited in real-world clinical practice in China during the study period. Furthermore, the addition of radiotherapy following chemotherapy has been shown to prolong both progression-free survival (PFS) and overall survival (OS), aligning with the results from IELSG clinical trials (14). Several small molecules and targeted agents, including immunomodulatory drugs (IMiDs) such as lenalidomide and pomalidomide, BTK-i like ibrutinib, zanubrutinib, and orelabrutinib, have been confirmed to exert antitumor effects in B-cell lymphomas by inhibiting BCR signaling and reducing NF-κB pathway activation. These agents have also demonstrated efficacy in crossing the blood-testicular and blood-brain barriers (15–18). In our study, patients who received maintenance therapy with these agents showed a trend toward improved PFS. However, no statistically significant differences in survival were observed based on the specific maintenance regimens used. Interestingly, BTK inhibitors did not display a clear benefit for long-term survival in PT-DLBCL patients, which may be due to their use primarily in the relapsed/refractory (R/R) setting rather than as part of frontline therapy. Only a small number of patients received R-CHOP in combination with agents such as lenalidomide or BTK inhibitors as frontline treatment. In light of recent preclinical and clinical studies highlighting the crucial role of the PD-1/PD-L1 pathway in immune evasion in PT-DLBCL (19, 20), PD-1 blockade was explored in our cohort. One patient achieved a partial response (PR) after receiving a combination of Rituximab and a BTK inhibitor, suggesting that immunotherapy may offer additional therapeutic benefit in select cases.
PT-DLBCL is particularly characterized by a high risk of CNS relapse, occurring in 10%–25% of patients. Although the exact mechanisms underlying CNS recurrence remain unclear, they are thought to involve latent molecular features specific to these immune-privileged sites (21). The CNS-IPI score has been validated as an effective risk stratification model for predicting CNS involvement, consistent with our findings (22, 23). For high-risk patients, implementing appropriate CNS prophylaxis is critical. A phase II study demonstrated that intravenous (IV) high-dose methotrexate (HD-MTX) combined with intrathecal (IT) liposomal cytarabine and R-CHOP was effective in preventing CNS relapse (24). In comparative analyses, IV-directed CNS prophylaxis showed superior survival outcomes over IT methotrexate in high-risk patients (25).However, a real-world study similar to ours found no significant difference in CNS relapse rates between IV and IT regimens (26). In our cohort, due to concerns about the toxicity of IV HD-MTX—especially in elderly patients—only one patient received this regimen. Approximately half of the patients underwent IT MTX prophylaxis, the clinical benefit of which remains controversial. Given that CNS relapses in our patients primarily involved the parenchyma rather than the leptomeninges (6 vs. 1), the limited benefit of IT chemotherapy seems reasonable. Altogether, beyond CNS-IPI scoring, genomic biomarkers could also be explored in identifying high-risk patients for CNS recurrence, and CNS-directed chemotherapy should be considered under close health monitoring. However, considering those who are unsuitable for HD-MTX, novel treatment approaches like rational combined therapy with targeted agents such as BTK-i, PD-1 inhibitors and CAR-T cells could be the future direction (27).
Several studies, including retrospective analyses and investigations using large datasets, have explored potential prognostic factors for PT-DLBCL, leading to the development of predictive nomograms (28, 29). However, no unified conclusion has been established thus far. Factors such as age, Ann Arbor stage, laterality, IPI score, and treatment modality have been reported as significant prognostic factors for PT-DLBCL. Interestingly, no obvious difference was observed in intermediate-risk and high-risk PT-DLBCLs when classified by IPI score, perhaps owing to the small number of patients cohort and the insufficient prognostic value of IPI score in PT-DLBCL patients without considering its unique biological characteristics. In our univariate analysis, older patients with advanced-stage disease, high IPI scores, double-expressor phenotypes, orchiectomy alone, and the absence of radiotherapy were associated with poor survival outcomes, consistent with previous reports (30). In multivariate analysis, radiotherapy emerged as an independent prognostic factor for progression-free survival (PFS), while the double-expressor phenotype was an independent factor for overall survival (OS). Given the rarity of this disease and the limited number of cases, our findings warrant further validation in larger, prospective, multi-center studies, and to further optimize prognostic scoring models.
In summary, this retrospective, real-world study included a relatively large cohort of testicular lymphoma patients in China, providing valuable insights into their diagnosis and treatment. Compared with STL, PTL cases tended to demonstrate different pathological subtypes, more favorable clinical responses and survival outcomes, which may reflect earlier disease stage at diagnosis, more localized involvement, and more standardized treatment strategies, based on primary symptoms and extranodal involvement. For PT-DLBCL patients, chemotherapy following orchiectomy, combined with consolidation therapy and radiotherapy, emerged as the recommended therapeutic approach in our study. Future research should focus on optimizing CNS prophylaxis strategies, identifying genomic predictors, and exploring the potential of immunotherapy and targeted therapies for high-risk patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Twa D Lee DG Tan KL Slack GW Ben-Neriah S Villa D. Genomic predictors of central nervous system relapse in primary testicular diffuse large B-cell lymphoma. Blood. (2021) 137:1256–9. doi: 10.1182/blood.2020006338, PMID: 32967007 · doi ↗ · pubmed ↗
- 2Cheah CY Wirth A Seymour JF. Primary testicular lymphoma. Blood. (2014) 123:486–93. doi: 10.1182/blood-2013-10-530659, PMID: 24282217 · doi ↗ · pubmed ↗
- 3Horne MJ Adeniran AJ. Primary diffuse large B-cell lymphoma of the testis. Arch Pathol Lab Med. (2011) 135:1363–7. doi: 10.5858/arpa.2010-0158-RS, PMID: 21970494 · doi ↗ · pubmed ↗
- 4King RL Goodlad JR Calaminici M Dotlic S Montes-Moreno S Oschlies I. Lymphomas arising in immune-privileged sites: insights into biology, diagnosis, and pathogenesis. Virchows Arch. (2020) 476:647–65. doi: 10.1007/s 00428-019-02698-3, PMID: 31863183 · doi ↗ · pubmed ↗
- 5Khessib T Itani M Hippe D Akaike G Bermo M Zare M. Testicular FDG uptake on PET/CT in patients with lymphoma: correlation with age. Curr Probl Diagn Radiol. (2022) 51:474–7. doi: 10.1067/j.cpradiol.2021.07.003, PMID: 34756775 · doi ↗ · pubmed ↗
- 6Higgins A Kim H Harper L Habermann TM Nowakowski GS Thompson CA. Testicular FDG-PET/CT uptake threshold in aggressive lymphomas. Am J Hematol. (2021) 96:E 81–81E 83. doi: 10.1002/ajh.26073, PMID: 33338288 PMC 7902412 · doi ↗ · pubmed ↗
- 7Ollila TA Olszewski AJ. Extranodal diffuse large B cell lymphoma: molecular features, prognosis, and risk of central nervous system recurrence. Curr Treat Options Oncol. (2018) 19:38. doi: 10.1007/s 11864-018-0555-8, PMID: 29931605 PMC 6294323 · doi ↗ · pubmed ↗
- 8Lee YP Yoon SE Cho J Ko YH Oh D Ahn YC. Real-world data analysis of survival outcomes and central nervous system relapses in testicular diffuse large B cell lymphoma. Cancer Manag Res. (2023) 15:463–74. doi: 10.2147/CMAR.S 407837, PMID: 37304895 PMC 10252944 · doi ↗ · pubmed ↗