Bilateral Choanal Atresia in a 65-Year-Old Female: A Case Report and Literature Review
Maraam Al Qout, Abdullah Alkarni, Abdulaziz Alaraifi, Mohammad Almahdi

TL;DR
A 65-year-old woman was diagnosed with a rare condition called bilateral choanal atresia, which is typically found in newborns and causes nasal blockage.
Contribution
This case report presents the oldest documented case of bilateral choanal atresia diagnosed in late adulthood.
Findings
The patient had lifelong nasal obstruction due to undiagnosed bilateral choanal atresia.
Endoscopic transseptal repair successfully treated the condition with no postoperative complications.
The case emphasizes the possibility of delayed diagnosis and variable clinical presentation of choanal atresia.
Abstract
Choanal atresia (CA) is a congenital condition characterized by occlusion of the nasal airway due to failure of recanalization during embryological development. It is more commonly unilateral and typically presents during infancy. In contrast, bilateral CA is a neonatal emergency that often manifests as respiratory distress at birth. The presentation of bilateral CA in late adulthood is extremely rare. This case presents an unusual case of an elderly patient diagnosed with bilateral CA at 65 years. She presented with a primary complaint of lifelong bilateral nasal obstruction and denied any symptoms suggestive of chronic rhinosinusitis. Examination revealed bilateral choanal obstruction with no visible openings in the nasal cavity. The patient underwent endoscopic transseptal repair of bilateral CA, which included perforation of the atretic plate, posterior septectomy, and flap…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
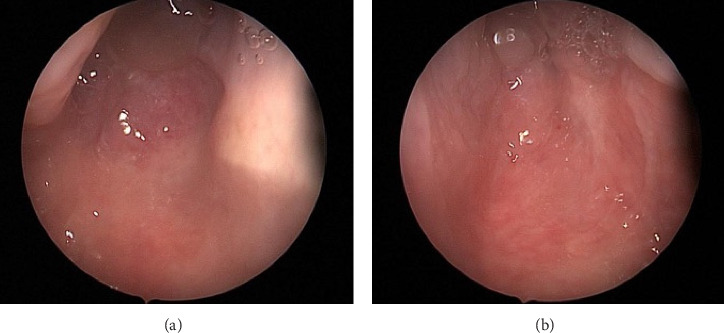 Figure 1
Figure 1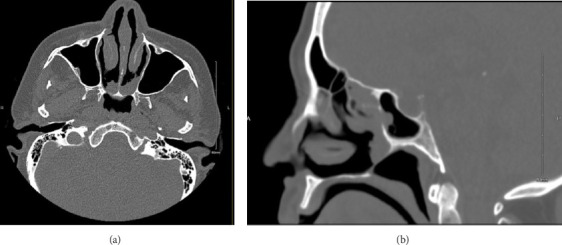 Figure 2
Figure 2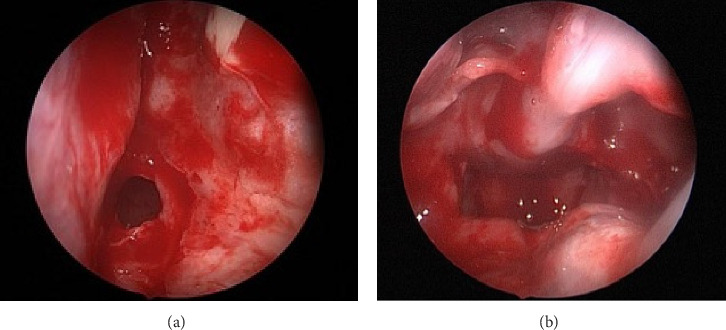 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Ear and Nasal Anomalies · Ear Surgery and Otitis Media · Pediatric Hepatobiliary Diseases and Treatments
1. Introduction
Choanal atresia (CA) is a congenital malformation of the nasal airway characterized by an occlusion between the nasal cavity and nasopharynx. This results from the failure of recanalization of the nasobuccal membrane during the seventh week of embryonic development [1]. It occurs more frequently in females than in males, with a ratio of 2:1, and has an estimated incidence of 1 in 8000 live births [2]. Unilateral CA is more common, accounting for approximately 60% of the cases. It often remains asymptomatic in neonates and rarely causes severe respiratory distress, sometimes presenting later in adulthood [1]. In contrast, bilateral CA is a neonatal emergency, typically manifesting as episodes of cyanosis and apnea shortly after birth [3]. Herein, we present a case of a 65-year-old woman diagnosed with bilateral CA, a condition typically detected at birth.
2. Case Presentation
A 65-year-old Saudi woman with a history of hypertension, diabetes mellitus, and bronchial asthma presented to the clinic with a complaint of lifelong bilateral nasal obstruction. She described the obstruction as persistent and associated with anosmia and intermittent mucoid nasal discharge. She denied any history suggestive of chronic rhinosinusitis, including postnasal drip, facial pain or pressure, and frontal headaches. She never sought medical management or intervention for her condition. Transnasal 0-degree endoscopic evaluation revealed bilateral complete absence of the choanal openings, which were surrounded by polypoidal tissue in proximity to the choanae (Figure 1). No other significant anatomical abnormalities were observed in the nasal cavities. A computerized tomography (CT) scan of the paranasal sinuses revealed bilateral CA with minimal mucosal thickening of the maxillary sinuses and mild opacification of the ethmoid air cells and sphenoid sinuses (Figure 2). These findings further confirmed the diagnosis and provided additional details on the sinonasal anatomy prior to potential surgical intervention. Regarding her comorbidities, the patient was managed by a family physician for hypertension, diabetes mellitus, and asthma, all of which were well controlled with medications. Prior to the operation, she was evaluated in the anesthesiology clinic for preoperative clearance and was classified as ASA class III.
The patient underwent endoscopic transnasal surgical repair of bilateral CA under general anesthesia. A 4-mm, 0-degree Hopkins telescope was used to examine the bilateral nasal cavities, revealing mixed bony and membranous CA with a thick vomer bone. Lidocaine (1%) with epinephrine (1:100,000) was injected into the posterior nasal septum, followed by a right-sided Killian incision and elevation of right mucoperiosteal flap. The atretic portion of the right nasal cavity was perforated transseptally using a suction freer, creating an initial passage to the postnasal space. The opening was then enlarged using a microdebrider, followed by posterior septectomy and removal of the bony junction between the atretic plate and vomer while preserving the mucoperiosteal flap bilaterally. The redundant mucosa was excised, and a common postnasal cavity was created, fully exposing the nasopharynx and the bilateral torus tubarius. Subsequently, the right and left mucoperiosteal flaps were predesigned to cover the postnasal common cavity along the roof and floor, respectively. A reassessment confirmed that the flaps were well positioned and a wide postnasal cavity had been achieved (Figure 3). Hemostasis was achieved using neuropatties soaked in xylometazoline and suction electrocautery. Finally, bilateral silastic breathable sheets were applied and secured in place using 2-0 Prolene sutures. The patient tolerated the procedure well, and no complications were observed. During postoperative follow-up visits at 2 weeks and 3 months, endoscopic examination of the nasal cavities revealed bilateral patent choanae with no stenosis (Figure 4).
3. Discussion
While unilateral CA is often asymptomatic and may go undiagnosed until later in life, bilateral CA typically presents as a neonatal emergency due to severe respiratory distress [1]. However, rare cases of bilateral CA diagnosed in adulthood have been reported [4, 5].
In 1755, Roederer reported the first instance of bilateral CA [6]. Several theories have been proposed to explain its embryological development, including the persistence of the buccopharyngeal membrane, Hochstetter's nasobuccal membrane, abnormal mesodermal tissue within the nasal choana, and misdirection of mesodermal flow due to local factors [7]. The condition is life-threatening in neonates, presenting with cyanosis, apnea, and respiratory distress, as newborns are obligate nasal breathers [1, 8, 9]. Therefore, the occurrence of undiagnosed bilateral CA persisting into adulthood is exceptionally rare. Carpenter and Neel (1977) studied 36 patients with unilateral or bilateral CA. Among them, twelve had bilateral CA, with eight diagnosed before 10 months of age, one at 16 months, one at 2 years, one at 15 years, and only one at 33 years [10]. These findings reinforce that bilateral CA is not typically considered a preliminary diagnosis for bilateral nasal obstruction in adults.
A review of the literature revealed 17 reported cases of bilateral CA in adults. As shown in Table 1, most patients were diagnosed in the second or third decade of life, whereas the present case involves a patient in her sixth decade. For instance, Aksoy et al. reported a 23-year-old patient with bilateral CA who presented with bilateral nasal obstruction and nasal discharge since birth [15]. The majority of the reported cases were females, including the current patient. Most cases had no associated abnormalities or disorders, while four cases were associated with telecanthus, hypogammaglobulinemia, pycnodysostosis, and Tessier number 3 facial cleft.
The current patient had hypertension, diabetes mellitus, and bronchial asthma; however, she had no associated congenital anomalies or syndromic disorders. Similar to this case, the most common presenting symptoms in the literature were nasal obstruction, rhinorrhea, and anosmia. Among the 17 reported cases, only two patients had a history of prior surgical intervention. The first underwent multiple procedures for cleft lip, palate, and nasal deformities, which may have contributed to the development of CA [9]. The second patient had surgical repair for bilateral CA as a newborn but later experienced recurrence [23]. Overall, only two patients were reported to have recurrence following surgical intervention. Importantly, all patients, including the present case, achieved favorable postoperative outcomes, with patent choanae documented during follow-up visits.
Our case represents the oldest documented instance in the literature to date. This patient experienced lifelong nasal obstruction without significant respiratory distress during infancy or childhood, suggesting possible partial obstruction or adaptation to oral breathing patterns. The latter is most likely because the examination showed no openings in the choana. This aligns with the theory proposed by Miller et al., who posited that infants are not strictly obligate nasal breathers and can adapt to oral breathing in the presence of nasal obstruction [10].
The management of bilateral CA in adults typically involves surgical intervention to establish nasal airway patency. The transnasal endoscopic approach is favored because of its effectiveness and minimally invasive nature. In this case, the patient underwent successful endoscopic transnasal repair, resulting in patent choanae and resolution of symptoms. This outcome is consistent with other reports advocating endoscopic techniques as a reliable treatment modality [13–16].
4. Conclusion
Bilateral CA is a rare congenital condition typically diagnosed in the neonatal period due to respiratory distress. However, in exceptional cases, it can remain undiagnosed until adulthood, as seen in this 65-year-old patient. This case adds to the growing evidence supporting the need to consider CA in adults presenting with lifelong nasal obstruction, even in the absence of significant respiratory symptoms. It also highlights the remarkable adaptability of some individuals to congenital nasal obstruction through compensatory mouth breathing. The successful surgical repair using an endoscopic transnasal approach further reinforces the efficacy of this technique in restoring nasal patency and improving quality of life.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andaloro C. Winters R. Ignazio La Mantia 2025 Stat Pearls [Internet]29939546 · pubmed ↗
- 2Verma R. K. Lokesh P. Panda N. K. Congenital Bilateral Adult Choanal Atresia Undiagnosed Until the Second Decade: How We Did It Allergy & Rhinology 201672 p. ar.2016.7.015510.2500/ar.2016.7.0155 PMC 501043727658184 · doi ↗ · pubmed ↗
- 3Tinoco P. Pereira J. C. O. Filho R. C. L. O. Bilateral Choanal Atresia in 34 Year-Old Patients Arquivos Internacionais de Otorrinolaringologia 2010 December 144481484
- 4Schwartz A. A. Isaacs H. J. Congenital Atresia of the Posterior Naresreport of Two Cases Archives of Otolaryngology-Head and Neck Surgery 1942 April 35460361210.1001/archotol.1942.00670010608008 · doi ↗
- 5James W. W. Hastings S. Discussion on Mouth-Breathing and Nasal Obstruction Proceedings of the Royal Society of Medicine 1932 June 2581343135510.1177/0035915732025008682-s 2.0-8491034775719988850 PMC 2184147 · doi ↗ · pubmed ↗
- 6Dunham M. E. Miller R. P. Bilateral Choanal Atresia Associated With Malformation of the Anterior Skull Base: Embryogenesis and Clinical Implications Annals of Otology, Rhinology & Laryngology 19921011191691910.1177/0003489492101011062-s 2.0-00264581721444099 · doi ↗ · pubmed ↗
- 7Pracy R. The Diagnosis of Respiratory Obstruction in Infants and Small Children Nursing Times 1972 July 68309309335044356 · pubmed ↗
- 8Carpenter R. J. Neel H. B.3rd Correction of Congenital Choanal Atresia in Children and Adults The Laryngoscope 1977 August 8781304131110.1288/00005537-197708000-000102-s 2.0-0017519428881923 · doi ↗ · pubmed ↗