A comparative study of diagnostic performance in shoulder pain: clinical tests versus ultrasonography and magnetic resonance imaging
Yasemin TOMBAK, Özgür Zeliha KARAAHMET, Ayşegül TOMBAK, Ömer ATA, Eda GÜRÇAY

TL;DR
This study compares the accuracy of clinical tests with imaging methods like ultrasound and MRI for diagnosing shoulder pain conditions.
Contribution
The study provides a direct comparison of clinical tests' diagnostic performance against US and MRI for specific shoulder pathologies.
Findings
Clinical tests showed higher sensitivity than US for subacromial impingement and biceps tendinitis.
Clinical tests had higher specificity than MRI for acromioclavicular arthritis and rotator cuff rupture.
MRI remains important for shoulder imaging despite the effectiveness of clinical tests.
Abstract
Shoulder pain is common and often evaluated with physical examination tests, yet their diagnostic accuracy remains controversial. The aim of this cross-sectional study was to determine the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) rates of clinical test results in patients with shoulder pain, based on ultrasonography (US) and magnetic resonance imaging (MRI) findings as reference diagnostic methods. The study included 78 patients who had complaints of shoulder pain. All patients underwent physical examinations and specific clinical tests (such as Neer and Jobe tests) to reveal shoulder pathologies, and US and MRI evaluations were performed. The sensitivity of clinical examination tests for subacromial impingement syndrome, biceps tendinitis and rupture, and infraspinatus tendinitis was higher than US. The specificity of tests for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
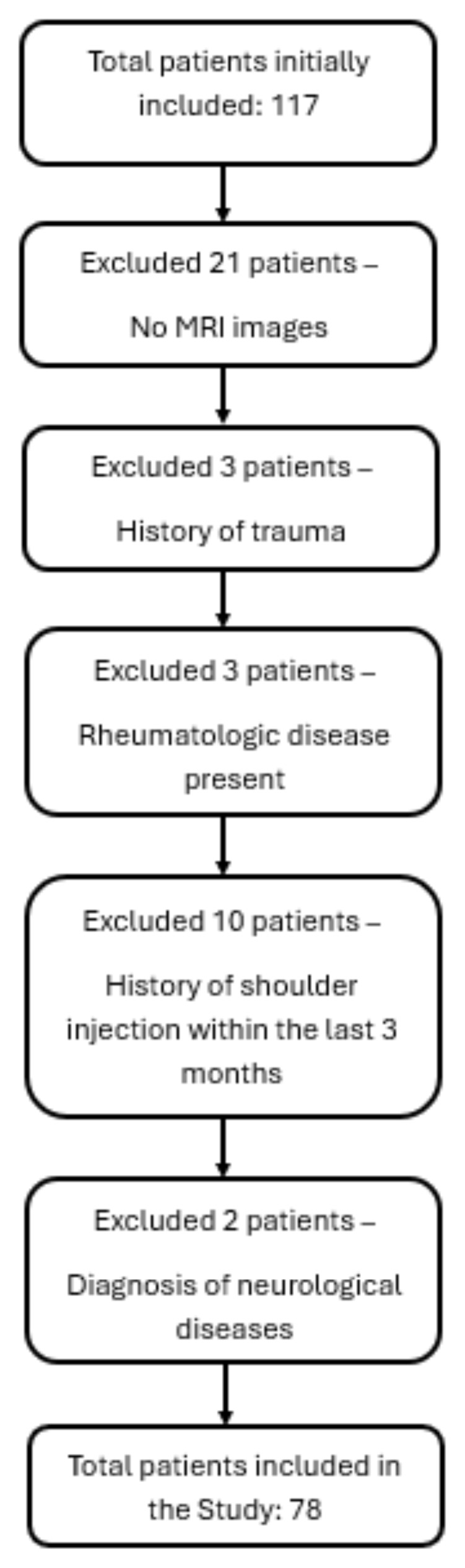 Figure 1
Figure 1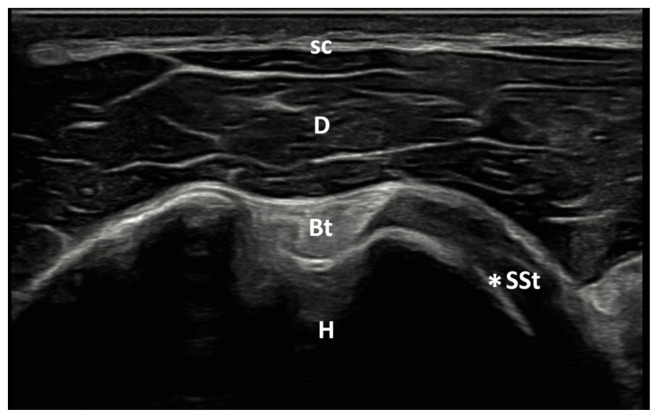 Figure 2
Figure 2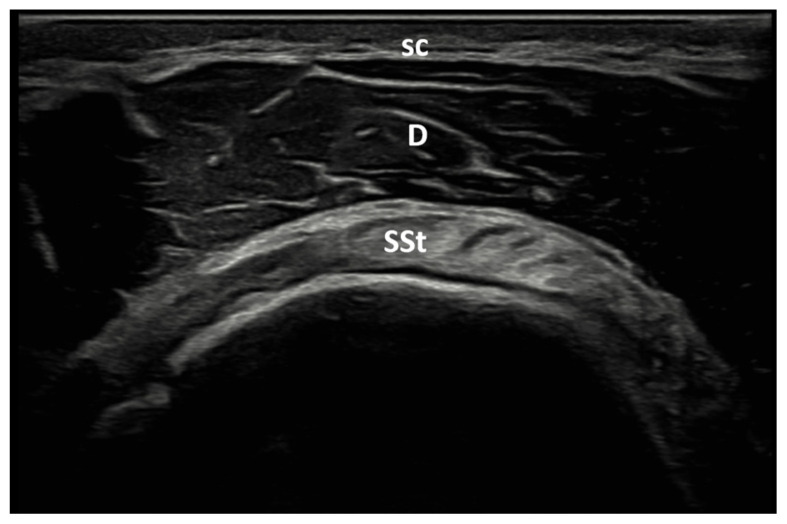 Figure 3
Figure 3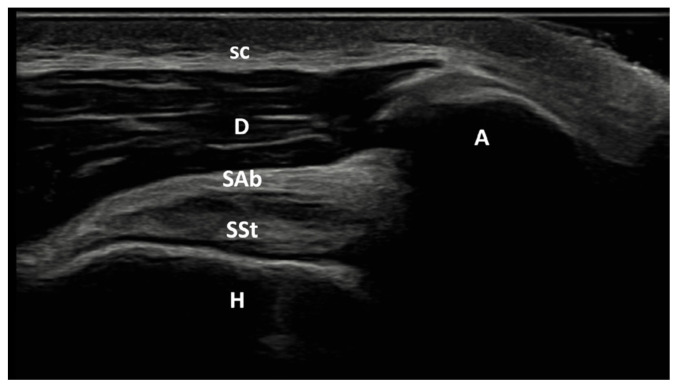 Figure 4
Figure 4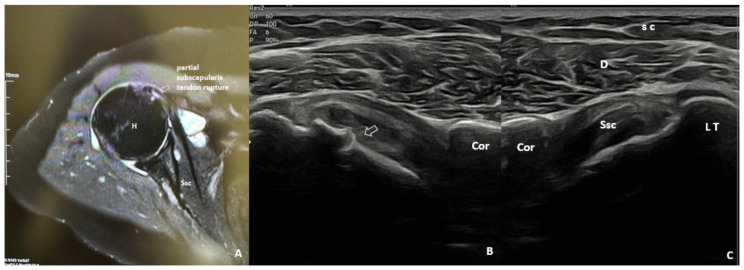 Figure 5
Figure 5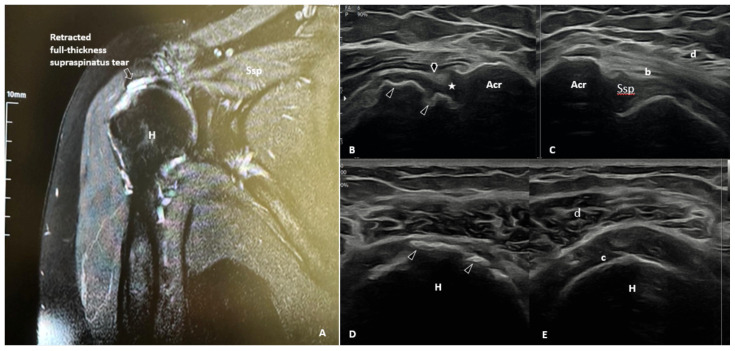 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Orthopedic Surgery and Rehabilitation
Introduction
Twenty percent of people worldwide suffer from shoulder pain [1]. Approximately two-thirds of individuals with non-specific shoulder pain have a rotator cuff lesion; however, tendinosis, adhesive capsulitis, osteoarthritis, labral tears, and transferred pain from the neck are all possible causes [2]. Physical examination tests are primarily preferred in diagnosis. These tests aim to simulate particular symptoms and indicators. The literature has described a wide variety of tests, so it can be challenging to decide which test to use [3]. The same test was conducted using various positivity criteria. For example, ‘weakness’ [4] and/or ‘pain’ [5] were used as positivity criteria for the supraspinatus test. Additionally, when the same test is called by different names (e.g., Supraspinatus test = Empty can test = Jobe test), confusion results [4–6]. The Yergason test [7], which measures biceps pathology, is also utilized to assess glenoid labral pathology [8].
The results of specific shoulder tests compared with imaging methods can give us an idea of which preliminary diagnoses will require imaging. There are studies in literature comparing US, MRI and clinical findings, but the issue of which clinical test has more diagnostic sensitivity is still controversial [9–11]. To date, no studies in the literature have been identified that combined specific shoulder tests, US, and MRI in the same patient. Therefore, we aimed to determine the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of clinical test results based on US and MRI in patients with shoulder pain.
Materials and methods
2.1. Study design and patient recruitment
The study was carried out in compliance with the Declaration of Helsinki’s principles and with authorization from the local ethics committee (Protocol No: 2023-695, dated 22.11.23). Every patient who took part in the study provided written consent.
This cross-sectional study included 78 consecutive patients aged 25–80 years who applied to the Physical Medicine and Rehabilitation (PMR) outpatient clinic with complaints of shoulder pain between January 2024 and April 2024.
The physician performing the clinical tests was blind to the US and MRI images. Physicians performing US and evaluating MRI images were blind to physical examination findings. US was performed within 3 days following the physical examination.
2.2. Exclusion and inclusion criteria
Patients over the age of 18 who had an MRI with shoulder pain in the last 2 weeks and agreed to participate in the study were included. Patients with a history of trauma or surgery, inflammatory rheumatic disease, another musculoskeletal problem in the upper extremity, and limited passive joint movements were excluded from the study.
The flow diagram illustrating patient enrollment and exclusion criteria is presented in Figure 1.
2.3. Clinical evaluation
The patients’ age, gender, education level, comorbidity, dominant side, symptomatic side, and symptom duration were recorded.
Specific shoulder tests and associated shoulder pathologies are shown in Table 1.
2.4. Ultrasonographic evaluation
Sonographic examinations were carried out in all patients with a single physician who had at least 5 years of US experience in musculoskeletal sonography blinded to the clinical test results of the patients, using a 7–15 MHz linear-array transducer (LOGIQ 9, GE HealthCare, Wauwatosa, WI, USA).
There have been many written accounts of the US examination method for the shoulder in the literature [30–32]. Scanning was performed while the subjects were in a sitting position, care was taken to ensure that the examined arm was not in abduction position, and the imaging included the humeral head’s circular structure.
The patient was positioned so that the elbow was flexed to 90° and the forearm was half pronated on the lap when the biceps tendon was examined. The long head of the biceps tendon is imaged as an oval-shaped echogenic structure on the anterior aspect of the shoulder. With a small external rotation of the GH joint, the hyperechoic subscapularis tendon was located anteromedial to the biceps tendon (Figure 2a). The patient’s shoulder was placed in hyperextension and full internal rotation while the dorsum of the hand was placed in the small of the back to examine the supraspinatus tendon. In a longitudinal view, supraspinatus tendon appears as a convex, tapered, hyperechoic fibrillar layer that inserts at the greater tuberosity (Figure 2b). The bursa subacromial-subdeltoid was detected on imaging as a hypoechoic line situated between the supraspinatus tendon and the deltoid muscle (Figure 2c). Patient’s hand was placed on the contralateral shoulder for examination of the Glenohumeral (GH) joint and infraspinatus tendon.
2.5. Magnetic resonance imaging evaluation
Axial Proton Density (PD), coronal PD-T2 fat suppressed (FS), coronal T1 Fast Spin Echo (FSE), and sagittal PD FS sequences were used in all patients. Rotator cuff tendons were examined for tendinitis, partial and full-thickness rupture. Increased signal intensity in PD-weighted sections was evaluated as tendinitis, increased fluid intensity in articular, bursal or intratendinous areas in T2 was evaluated as partial rupture, focal or diffuse loss of integrity and retraction in the tendon was evaluated as full-thickness rupture. Subacromial-subdeltoid bursa, glenohumeral joint, biceps tendon, acromioclavicular joint, humeral head changes were examined routinely.
Shoulder US and MRI images of the same patient are shown in Figure 3 and Figure 4.
2.6. Statistical analysis
All the statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) for Windows (Version 22.0, IBM Corp., Chicago, IL, U.S.A.). With regard to categorical variables, data are displayed as frequency (%). When calculating a p value for categorical variables, the chi-squared test was used. Statistics were deemed significant if the p-value was less than 0.05.
2.7. Sample size calculation
The sample size calculations were based on data from the earlier study by Naredo et al. [31]. The number of participants was calculated using an incidence of subacromial impingement syndrome population (44%) and study group (20%) respectively, with 95% power and 1% significance. We eventually determined that at least 65 people would be allocated.
Results
Demographic and clinical data of the patients are shown in Table 2. The average age was found to be 53.5 years and 74.4% were female.
Table 3 demonstrates the distribution of the patients’ clinical, sonographic, and MRI-detected shoulder lesions. Tables 4 and 5 show the diagnostic performance levels of clinical test results in distinguishing patients with and without shoulder lesions detected by US and MRI, respectively.
When clinical examination results of subacromial impingement syndrome, biceps tendinitis and rupture, and infraspinatus tendinitis were compared with US, their sensitivity was found to be high.
When clinical examination results for biceps rupture, rotator cuff rupture, infraspinatus and subscapularis tendinitis were compared with US, their specificity was found to be high.
Subacromial impingement syndrome was found to have higher sensitivity when clinical examination results were compared with MRI.
When clinical examination results for AC arthritis, biceps rupture, rotator cuff rupture, infraspinatus tendinitis were compared with MRI, their specificity was found to be high.
Discussion
In this study diagnostic performance levels of clinical tests were investigated with the sensitivity, specificity, PPV and NPV parameters based on US and MRI results in shoulder pain. The most clinically detected cases were subacromial impingement syndrome (51.3%) and supraspinatus tendinitis (51.3%). Supraspinatus tendinitis was mostly detected in MRI and US. The most common occurrence of supraspinatus tendinitis was consistent with the literature [33].
One of our remarkable results was that, contrary to the literature [34], subscapularis tendinitis was detected more frequently as examination, US and MRI findings than infraspinatus tendinitis.
According to our results, we found that the sensitivity of clinical tests compared to US in subacromial impingement syndrome was 91.7% and the negative predictive value was 97.4%. Again, the sensitivity and negative predictive value of the examination in subacromial impingement syndromes were as high when compared with MRI as they were when compared with US. In addition, the specificity of clinical tests compared to US in subacromial impingement syndrome was found to be 56.1% and PPV was 27.5%. The reason why we found the specificity to be low while the sensitivity was high may be that we applied the tests in combination. Calis et al. in their study examined combinations of clinical tests and found that as the number of tests found positive together increased, sensitivity rates increased, and specificity rates decreased [35].
When clinical tests were compared with US in AC arthritis, sensitivity was found to be 25%, specificity was 88%, positive predictive value was 100%, and negative predictive value was 88%. The fact that we performed a single test instead of a combined test in AC arthritis may have caused the specificity to be high. This situation in AC arthritis was also present in the clinical examination and MRI comparison. While physical examination tests were not sensitive compared to MRI in AC arthritis, a specificity of 95% was detected.
In a study comparing US and MRI findings, the sensitivity and specificity of US in full-thickness tears of the supraspinatus tendon were found to be 95%, in cases of partial tears the sensitivity was 91% and specificity was 98%, in cases of supraspinatus tendinosis the sensitivity and specificity were found to be 90% and specificity 93% [36]. Our sensitivity and specificity results of physical examination compared to MRI in supraspinatus partial tear and tendinitis were lower than the results of this study. The reason we over-detect supraspinatus tendinitis during examination may be that it is also positive in other shoulder pathologies. During clinical tests, pain occurs by stimulating nociceptors by compressing or stretching the subacromial bursa. Weakness in the arm occurs due to pain inhibition, and the clinician may misinterpret these findings. This may explain why the tests show false positivity [11].
In addition, although we did not detect any full-thickness tears of the supraspinatus tendon during the examination, it was detected in the MRI. We could not detect any subscapularis or infraspinatus tears on examination. With these results, we do not know whether physical examination is insufficient to detect tendon ruptures or whether the results vary from person to person. We can emphasize the importance of MRI in detecting full-thickness tendon tears. Clinical tests may suffice for the initial evaluation, particularly for subacromial impingement, but MRI should be prioritized when tendon ruptures are suspected. In a study where shoulder examination and US evaluations were performed in patients with spinal cord injury who had shoulder pain, Neer’s impingement test was the most common examination finding, while O’Brien’s test was the least common examination finding. Sensitivity-specificity evaluation was not performed in this study [37]. In our case, subacromial impingement syndrome was easily detected dynamically using US. However, superior labrum anterior and posterior (SLAP) lesions were detected less frequently. Subacromial impingement syndrome is a dynamic pathology. For this reason, MRI may not be preferred in detecting subacromial impingement syndrome. We can easily detect subacromial impingement with dynamic impingement findings on US [38].
In Günay’s study, the Speed test was found to be 100% sensitive in biceps tendinitis, and the specificity was found to be 13.6%. Our study differs in that we evaluated biceps tendinitis using both the Speed and Yergason tests [10]. While the sensitivity of clinical tests in biceps pathologies is higher in the literature, we found the specificity to be high [11,35,39].
Leroux et al. found the sensitivity of the Patte test in infraspinatus lesions to be 92% and the specificity to be 30% [40]. While the diagnostic performance level of the Patte test in infraspinatus lesions was found to be statistically significant, the resisted rotation test was not found to have sufficient diagnostic performance [11]. Our results in infraspinatus tendinitis did not have significant diagnostic performance.
In one study, the lift-off test was found to be 89.47% sensitive in subscapularis partial tear [10]. We did not evaluate partial tears of the subscapularis because they could not be detected on clinical examination; however, we found that clinical tests had lower sensitivity than MRI in diagnosing subscapularis tendinitis. Clinically, we determined that the tests we performed for subscapularis tendinitis had high sensitivity, specificity, PPV and NPV rates, and significant diagnostic performance when compared to US. The higher number of subscapularis tendinitis cases in our study may have been effective in reaching this conclusion.
The results of Naredo et al. show that clinical diagnosis of periarticular conditions in the painful shoulder is not very accurate compared to US diagnosis [31]. They said that this was an expected result. They explained this situation as the impingement syndrome in most patients with chronic shoulder pain and the presence of several periarticular lesions, usually involving different tendons and the subacromial-subdeltoid bursa. In clinical tests, significant diagnostic performance was detected in subacromial impingement syndrome, AC arthritis, biceps tendinitis, biceps rupture, rotator cuff rupture and subscapularis tendinitis according to US.
4.1. Limitations and advantages of the study
There may be false positives in the examination, or there may be shoulder lesions that we cannot detect. In our study, supraspinatus full-thickness tears, biceps subluxation, SLAP, infraspinatus and subscapularis tears were detected on imaging, although they were not detected on examination.
We have not found many studies evaluating the sensitivity and specificity of clinical examination tests compared to US. Generally, studies were conducted with MRI evaluation. We compared clinical tests with both US and MRI. To the best of our knowledge, this is the first study to investigate the diagnostic performance of clinical tests by comparing two different imaging methods.
The single-center nature of our study, the relatively small sample size, and the operator dependency of US can be considered as limitations.
Conclusion
Patients with shoulder pain may have more than one pathological lesion. Clinical tests have an important place in practice when examining shoulder lesions with their high specificity and sensitivity. Although US reveals many shoulder lesions that cannot be detected by clinical tests or support our examination, MRI maintains its importance in shoulder imaging.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vecchio P Kavanagh R Hazleman BL King RH Shoulder pain in a community-based rheumatology clinic British Journal of Rheumatology 1995 34 5 440 442 10.1093/rheumatology/34.5.440 7788173 · doi ↗ · pubmed ↗
- 2Mitchell C Adebajo A Hay E Carr A Shoulder pain: diagnosis and management in primary care The British Medical Journal 2005 331 7525 1124 1128 10.1136/bmj.331.7525.1124 16282408 PMC 1283277 · doi ↗ · pubmed ↗
- 3Mc Farland EG Examination of the Shoulder: The Complete Guide 1st ed New York (NY) Thieme Medical Publishers 2006
- 4Holtby R Razmjou H Validity of the supraspinatus test as a single clinical test in diagnosing patients with rotator cuff pathology Journal of Orthopaedic and Sports Physical Therapy 2004 34 4 194 200 10.2519/jospt.2004.34.4.194 15128189 · doi ↗ · pubmed ↗
- 5Chew K Pua YH Chin J Clarke M Wong YS Clinical predictors for the diagnosis of supraspinatus pathology Physiotherapy Singapore 2010 13 2 12 17
- 6Jobe FW Moynes DR Delineation of diagnostic criteria and a rehabilitation program for rotator cuff injuries The American Journal of Sports Medicine 1982 10 6 336 339 10.1177/036354658201000602 7180952 · doi ↗ · pubmed ↗
- 7Yergason RM Supination sign Journal of Bone and Joint Surgery 1931 13 160
- 8Holtby R Razmjou H Accuracy of the Speed’s and Yergason’s tests in detecting biceps pathology and SLAP lesions: comparison with arthroscopic findings Arthroscopy 2004 20 3 231 236 10.1016/j.arthro.2004.01.008 15007311 · doi ↗ · pubmed ↗