Impact of pulmonary metastasectomy timing and nodule characteristics on survival outcomes in patients with pediatric sarcoma
İlteriş TÜRK, Mehmet ÇETİN, Neriman SARI, Selma ÇAKMAKCI, Necati SOLAK, Fatma BABACAN, Nesrin GÜRÇAY, Pınar BIÇAKÇIOĞLU

TL;DR
Early surgery for lung metastases in pediatric sarcoma patients improves 5-year survival, with fewer nodules linked to better outcomes.
Contribution
Demonstrates that early pulmonary metastasectomy within 30 days of detection improves survival in pediatric sarcoma patients.
Findings
Patients who had PM within 30 days of metastasis detection had a 75.26% 5-year survival rate versus 35.88% if delayed.
Fewer metastatic nodules (<10) and fewer nodules per operation (<3) correlated with better 5-year survival outcomes.
Survival outcomes were similar across different sarcoma subtypes like osteosarcoma and Ewing sarcoma.
Abstract
Pulmonary metastasectomy (PM) is a crucial intervention for patients with metastatic sarcomas, particularly among pediatric populations. The timing of PM and its impact on survival outcomes remain a subject of debate in the literature. This study aims to evaluate the impact of PM on survival outcomes. This retrospective study included pediatric patients diagnosed with sarcomas who underwent pulmonary metastasectomy. Demographic and clinical characteristics, including age, sex, primary malignancy type, metastasis presence at diagnosis, chemotherapy response, and PM details (e.g., number and laterality of metastatic nodules, time from metastasis detection to surgery) were analyzed. Survival data were assessed using Kaplan–Meier curves and Cox regression analysis, and statistical significance was determined using log-rank tests. A total of 29 patients (51.7% male, 48.3% female) were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
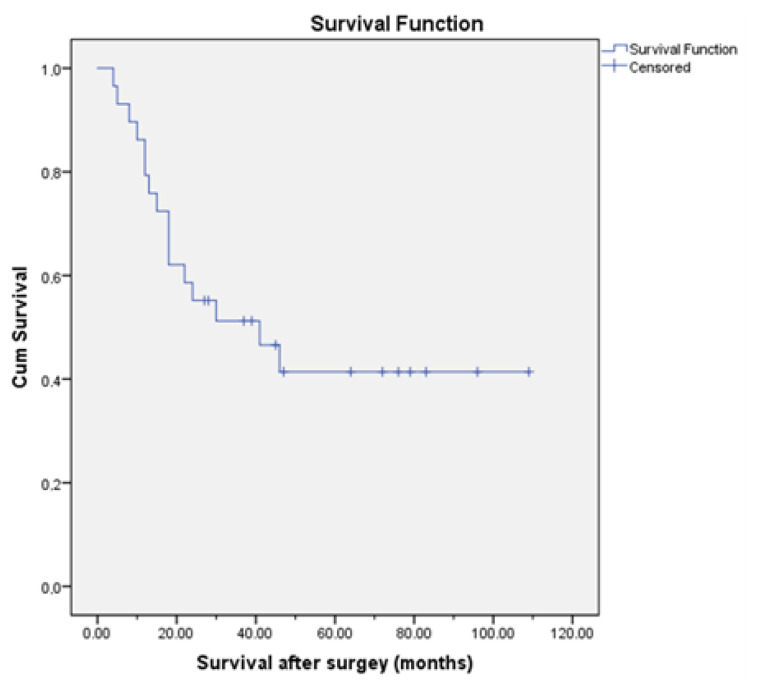 Figure 1
Figure 1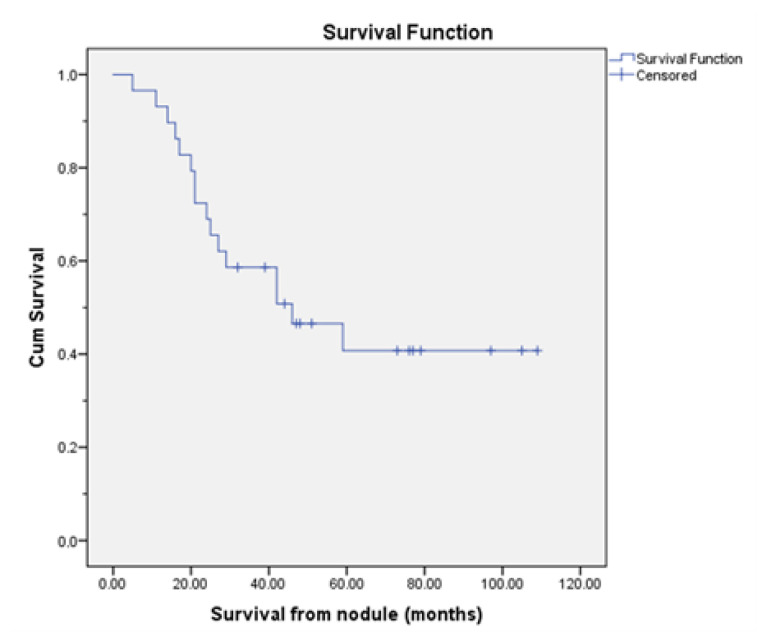 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroblastoma Research and Treatments · Sarcoma Diagnosis and Treatment · Lung Cancer Diagnosis and Treatment
Introduction
Pulmonary metastasectomy (PM) has long been employed in the management of lung metastases originating from various primary organ cancers. Over the years, several criteria for surgical candidacy have gained general acceptance. These include control of the primary tumor, absence of extrapulmonary metastases, complete resectability of pulmonary metastases, adequate pulmonary reserve to tolerate surgery, and the absence of a more effective alternative treatment option. Numerous studies have emphasized that PM performed in accordance with these patient selection criteria can significantly improve survival outcomes [1–3].
Malignancies in children represent a specific subgroup within this context. In pediatric patients with solid tumors, metastatic disease and complications of its treatment are the most common causes of mortality. Among children with bone and soft tissue malignancies, the incidence of pulmonary metastases at diagnosis or during follow-up is particularly high [4,5]. Since Richardson’s 1961 publication of outcomes following PM in 35 pediatric patients, the literature has consistently advocated that staged bilateral resections should not be avoided, that the number of metastases and the disease-free interval should not be considered absolute contraindications for PM, and that the primary histology is the most critical determinant of survival [6–8].
This study aims to evaluate the prognostic factors influencing survival following PM in pediatric patients with sarcomas and to assess the impact of timing of PM on clinical outcomes.
Materials and methods
A retrospective analysis was conducted on data from 29 pediatric patients who underwent pulmonary metastasectomy (PM) for lung metastases of bone and soft tissue sarcomas at our center between 2016 and 2022. Metastasectomies performed in adult patients and procedures targeting nonsarcoma tumor metastases in pediatric patients were excluded from the study. Local ethics committee approval was obtained prior to the study (Approval no: 2024-BÇEK/56), and the study was conducted in accordance with the Declaration of Helsinki. Patient data included age, sex, histologic subtype of the primary tumor, presence of pulmonary metastases at the time of initial diagnosis, time interval between detection of the pulmonary nodule and PM (categorized as surgery within the first month versus later), laterality of PM (unilateral or bilateral), number of PM procedures, total number of resected metastatic nodules per procedure (categorized as < 3, 3–10, or > 10), receipt of radiotherapy (RT) to the lungs, presence of complications, length of hospital stay, postmetastasectomy survival time, survival time from nodule detection, and 5-year survival rates. The impact of each variable on survival time and 5-year survival rate, both after PM and from the time of nodule detection, was evaluated.
2.1. Surgical technique and management
All patients included in the study were evaluated for pulmonary metastases via thoracic computed tomography (CT) during follow-up in the pediatric oncology clinic where they were being treated for their primary tumor. Positron emission tomography/computed tomography (PET/CT) was performed at diagnosis and at relapse to evaluate extrapulmonary metastases. Once the decision for PM was made by the oncology team, patients were referred to the thoracic surgery department, and the preoperative preparation process was initiated. The surgical team assessed whether the patients’ primary tumors were under control, whether all pulmonary nodules could be resected with PM, and whether the patients had sufficient respiratory capacity. Preoperative anesthesia evaluations were initiated for patients deemed suitable. All patients met the widely accepted criteria for PM eligibility.
All surgeries were performed under general anesthesia using double-lumen endotracheal intubation, with patients positioned in the lateral decubitus position, and a muscle-sparing thoracotomy approach was used. When necessary, staged bilateral thoracotomies or repeated thoracotomies on the same side were performed due to newly developed nodules during follow-up. In patients with numerous small nodules, excision was performed using the precision cautery excision technique as described by Perelman [9]. For fewer and larger nodules, wedge resections were performed. All resections were nonanatomical, and no patient required anatomical resection. At the end of each operation, a single chest drain was routinely placed. In the absence of complications, patients were monitored for 1 day in the intensive care unit and then transferred to the general ward. They were discharged following control chest radiography on the day the drain was removed.
2.2. Chemotherapy protocols
For osteosarcoma, first-line chemotherapy consisted of a combination of high-dose methotrexate, doxorubicin, and cisplatin (MAP regimen) [10]. In relapsed or refractory cases, second-line therapies included high-dose ifosfamide, oxaliplatin, irinotecan, and the multikinase inhibitor sorafenib [11].
Patients with Ewing sarcoma received alternating cycles of vincristine, doxorubicin, and cyclophosphamide (VDC) with ifosfamide and etoposide (IE) as standard first-line treatment [12]. In cases of relapse or refractory disease, salvage regimens containing irinotecan, temozolomide, carboplatin, and tyrosine kinase inhibitors were used [13].
In rhabdomyosarcoma, low- and intermediate-risk patients were treated with vincristine, dactinomycin, and cyclophosphamide (VAC). For high-risk patients, this regimen was intensified with vincristine, doxorubicin, and cyclophosphamide (VDC), alternating with ifosfamide and etoposide (IE), and supplemented with irinotecan [14]. Relapsed or refractory cases were managed with carboplatin-based chemotherapy and tyrosine kinase inhibitors [15]. For patients with synovial sarcoma and alveolar soft part sarcoma, first-line chemotherapy included ifosfamide and doxorubicin, while tyrosine kinase inhibitors were used in relapsed patients.
2.3. Statistical analysis
All statistical analyses were performed using SPSS software, version 24.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were presented as count (n), percentage (%), mean ± standard deviation (SD) for age, and median ± standard error (SE) for survival durations. Overall survival from the time of surgery, from the time of nodule detection, and from initial diagnosis was evaluated using the Kaplan–Meier method and compared using the log-rank test. Variables analyzed included age, sex, presence of metastasis at diagnosis, primary malignancy type, response to chemotherapy, primary relapse, pulmonary relapse, interval between metastasis detection and surgery, surgical approach, number of surgeries, total number of nodules, number of nodules per surgery, receipt of pulmonary radiotherapy, and presence of postoperative complications. The 2-year and 5-year survival rates after surgery and after nodule detection were also calculated using the Kaplan–Meier method and compared across groups. Survival time after PM and from nodule detection was compared with other parameters using Cox regression analysis. A p-value less than 0.05 was considered statistically significant.
Results
Of the 29 patients, 15 were female and 14 were male, with a mean age of 13.59 ± 3.96 years (range: 3–18 years). The most common primary malignancy leading to pulmonary metastasis was osteosarcoma, accounting for 41.4% of cases. The primary tumors were most frequently located in the lower extremities, predominantly in the femur. The mean interval from initial diagnosis of the primary tumor to the development of pulmonary metastases was 13.3 months (range: 0–64 months). A total of 47 PM procedures (range: 1–4 per patient) were performed. Among the 864 pulmonary nodules excised during these surgeries, 782 (90.5%) were histopathologically confirmed as metastatic. The median number of nodules resected per surgery was six (range: 1–72). The median time from detection of pulmonary nodules to PM was 90 days (range: 2–870 days). Postoperative complications occurred in four (8.5%) of the 47 operations. There was no surgical mortality. The median length of hospital stay following PM was 5 days (range: 3–9 days). Demographic and general perioperative data are summarized in Table 1.
Patients aged 12 years or younger, those who underwent PM within the first 30 days following nodule detection, those with fewer than 10 total metastatic nodules, and those with fewer than three nodules excised per procedure had significantly longer survival after PM compared to other groups. No statistically significant differences in survival were observed among other parameters (Table 2).
With a median follow-up duration of 42 months, 11 patients were alive, while 18 patients (62.1%) had died. At the time of analysis, the mean post-PM survival duration was 51.97 ± 7.98 months, while the mean survival from the time of nodule detection was 57.52 ± 7.50 months. The 5-year survival rate from the time of nodule detection was 40.7% ± 10%, and the 5-year survival rate following PM was 41.4% ± 9.8%. Kaplan–Meier survival curves for 5-year survival rates are presented in Figure 1 and Figure 2.
Analysis of prognostic factors revealed that patients with fewer than three nodules resected per PM procedure and those who underwent PM within 30 days of nodule detection had significantly higher 5-year survival rates both after PM and from the time of nodule detection (p = 0.006 and p = 0.039, respectively) (Table 3). In multivariate Cox regression analysis, post-PM survival was found to be significantly better in patients whose interval between metastasis and surgery was less than 30 days. However, no statistically significant difference was observed in survival time following nodule detection (p = 0.035 and p = 0.150, respectively) (Table 4).
Discussion
The optimal timing of pulmonary metastasectomy (PM) has long been debated in the literature, with varying findings reported. Tanaka et al., in a study including both adult and pediatric patients with diverse primary histologic types, suggested that a 3-month surveillance period following the detection of pulmonary nodules might help prevent early relapse and improve prognosis [16]. In contrast, another study focusing solely on pulmonary metastases from colorectal cancers recommended a considerably longer follow-up period of 9 months after nodule detection [17]. Yet another study on colorectal cancer metastases proposed immediate PM for solitary and peripheral lesions, while recommending two consecutive 3-month follow-up intervals before deciding on PM or deferring surgery in other cases [18]. On the other hand, Detterbeck et al., in a publication evaluating imaging requirements before PM, advocated for the earliest possible surgical intervention if the patient’s clinical condition allows, arguing that delaying resection offers no benefit [19]. Waiting for PM after diagnosis may be considered questionable due to the possibility of existing metastases growing and requiring more extensive resections or even seeding additional metastases.
In a comprehensive review, Krüger summarized the main arguments against early surgery in three categories: (1) deferring surgery to exclude rapidly progressive disease during the initial months, (2) allowing for chemotherapy administration before PM, and (3) avoiding reoperations in case of initially undetected small lesions [20]. However, numerous studies have emphasized that repeat surgeries do not adversely affect survival and should not be avoided when necessary [21–23]. An earlier study focusing on pediatric sarcomas also supported the survival benefit of repeat PM in appropriate cases [24]. In a study involving 81 sarcoma patients, adjuvant chemotherapy following R0 resection during PM did not demonstrate additional survival benefit [25]. A study examining the doubling time of pulmonary metastases reported 109 days for colorectal cancers, 42 days for sarcoma metastases, and only 37 days for very young patients regardless of histologic type [26]. In our study, univariate analysis showed that performing PM within the first 30 days after nodule detection significantly improved both 5-year survival from nodule detection and post-PM survival. In multivariate analyses, while the post-PM outcome remained statistically significant, the lack of statistical significance for survival after nodule detection may be attributed to the limited number of patients. Therefore, we advocate for prompt PM in pediatric patients with sarcoma who meet surgical criteria.
The timing of metastasis appearance may also provide prognostic insights. In a study evaluating 88 osteosarcoma patients who underwent PM, patients were grouped based on the timing of metastasis: present at initial diagnosis, emerging during chemotherapy, or appearing during follow-up after completion of treatment. The worst survival outcomes were observed in patients who developed metastases during chemotherapy [27]. Another study with a smaller osteosarcoma cohort suggested that the presence of pulmonary metastases at diagnosis was associated with worse survival [28]. A separate study identified pulmonary metastases progressing under neoadjuvant chemotherapy as an independent prognostic factor for poor survival [25]. In our study, patients were grouped based on whether they had pulmonary metastases at initial diagnosis. While the 5-year survival rate was 45.8% in those with metastases at diagnosis and 36.9% in those without, the difference was not statistically significant. This may be due to the heterogeneity of the second group, as also noted by Ahmed et al. [27].
The number of pulmonary metastases has long been a subject of debate in terms of its impact on survival, and PM is increasingly being performed in patients with multiple metastases. Nevertheless, a high number of nodules is often considered a marker of aggressive tumor biology [29]. In a study of 615 patients undergoing PM for colorectal cancer, those with three or fewer metastatic nodules had significantly better 5-year survival rates [30]. Similarly, a study on sarcoma metastases found that progression under chemotherapy and the presence of more than three metastases were independent risk factors for worse overall survival [31]. Consistent with the literature, we found that the presence of fewer than three metastatic nodules per operation, regardless of the total number of surgeries, was significantly associated with longer survival and higher survival rates in our patient cohort.
Smolle et al., in their study on lung metastases of bone sarcomas, reported that the majority of patients had osteosarcoma, followed by Ewing sarcoma, and found no significant survival differences between histologic types. They reported a 5-year survival rate of 44.8% after PM [32]. Lin et al., in another study, reported a median survival of 35.4 months and a 5-year survival rate of 34.8%. Conversely, they noted better survival after PM in osteosarcoma compared to synovial sarcoma [33]. Another study reporting a 5-year survival rate of 41% demonstrated the survival benefit of PM in relapsed osteosarcoma cases [34]. Osteosarcoma and Ewing sarcoma—the most common and second most common bone tumors in children, respectively [35]—constituted the majority of our cohort. However, we found no statistically significant difference in survival between different histologic subtypes. Our 5-year survival rate of 41.4% after PM is consistent with previously reported data.
A current topic of discussion is whether thoracotomy or video-assisted thoracoscopic surgery (VATS) yields better outcomes in PM. Many recent studies report that VATS does not confer a survival disadvantage compared to thoracotomy. A metaanalysis including 1541 patients from four studies found no survival difference between VATS and thoracotomy, while VATS was associated with shorter hospital stays [36]. Another study based on database analysis noted that although VATS use was associated with shorter hospitalizations, the rate of adoption demonstrated a peak in 2009 [37]. In a survey conducted by the American Pediatric Surgical Association, only 34% of surgeons preferred VATS for patients with three nodules on one side, and this dropped to 21% for five nodules [38]. A study comparing PM via thoracotomy and VATS in 202 osteosarcoma patients found similar survival outcomes but expressed concern over potential selection bias. Additionally, although not statistically significant, the VATS group had a higher number of R1 resections [39]. A study conducted in Türkiye including 226 PM procedures (including adults) found that thoracotomy allowed resection of 1.9 times more malignant nodules than were initially detected on CT scans [40]. There is a common concern that subcentimeter nodules may be missed using VATS due to the lack of bimanual palpation, potentially resulting in incomplete (non-R0) resections. Moreover, the inability of CT to detect some of these small nodules further emphasizes the importance of manual palpation. For all these reasons, we prefer and recommend a muscle-sparing thoracotomy approach for PM in accordance with oncologic principles.
Although our study included only pediatric sarcoma cases, its limitations include its single-center nature, a relatively small sample size, exclusion of patients with pulmonary metastases who did not undergo surgery, limited generalizability due to the inclusion of multiple histological subtypes in a single analysis, and the retrospective design, which may have introduced selection bias. Nevertheless, our findings contrast with some previous literature and demonstrate that, in pediatric sarcoma patients who meet surgical criteria, early PM contributes to improved survival.
In conclusion, early pulmonary metastasectomy, particularly when performed within 30 days of nodule detection, appears to improve survival in pediatric sarcoma patients. A lower number of metastatic nodules per surgery also correlates with better outcomes. These findings support expeditious surgical intervention in eligible cases to maximize long-term survival.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rusch VW Pulmonary metastasectomy: a moving target Journal of Thoracic Oncology 2010 5 6 Suppl 2 130 131 10.1097/JTO.0b 013e 3181 dca 268 20502246 · doi ↗ · pubmed ↗
- 2Nichols FC Pulmonary metastasectomy Thoracic Surgery Clinics 2012 22 1 91 99 10.1016/j.thorsurg.2011.08.017 22108693 · doi ↗ · pubmed ↗
- 3Zhao P Jiang Q Xue K Liu X Tian B The role of pulmonary metastasectomy in patients suffering pancreatic ductal adenocarcinoma with lung metastases: a systematic review and meta-analysis Frontiers in Surgery 2025 27 12 1535212 10.3389/fsurg.2025.1535212 40084343 PMC 11903735 · doi ↗ · pubmed ↗
- 4Corkum KS Craig BT Piche N Pio L Fernandez-Pineda I Current surgical approach to pulmonary metastasectomy Pediatr Blood and Cancer 2025 72 Suppl 2 e 31468 10.1002/pbc.31468 39654090 · doi ↗ · pubmed ↗
- 5Boam T Rogoyski BG Jawaid W Losty PD Do children with osteosarcoma benefit from pulmonary metastasectomy?: a systematic review of published studies and “real world” outcomes Annals of Surgery 2024 280 2 235 240 10.1097/SLA.0000000000006239 38375639 · doi ↗ · pubmed ↗
- 6Richardson WR Progress in pediatric cancer surgery. Recent advances in the surgical management of neoplasms in infants and children Archives of Surgery (Chicago, Ill :1960) 1961 82 641 655 10.1001/archsurg.1961.01300110003001 13741310 · doi ↗ · pubmed ↗
- 7Croteau NJ Heaton TE Pulmonary metastasectomy in pediatric solid tumors Children (Basel, Switzerland) 2019 6 1 6 10.3390/children 6010006 30626161 PMC 6352020 · doi ↗ · pubmed ↗
- 8Türkİ Çetin M Gürçay N SarıN ÖzkaraŞ Bıçakçıoğlu P Tuberculosis mimicking rhabdomyosarcoma metastasis in a pediatric patient Archives of Current Medical Research 2022 3 2 158 162 10.47482/acmr.2022.62 · doi ↗