Do the expressions of HLA-G and killer cell immunoglobulin-like receptors change in colorectal cancer?
Ezgi DİNÇER, Fatma KAYA DAĞISTANLI, Kıvanç Derya PEKER, Damlanur SAKIZ, Figen ABATAY SEL, Demet KIVANÇ, Hayriye ŞENTÜRK ÇİFTÇİ, Çiğdem KEKİK ÇINAR, Şule KARATAŞ, Fatma SAVRAN OĞUZ

TL;DR
This study explores how HLA-G and KIR molecules are expressed in colorectal cancer, suggesting they may help predict cancer outcomes and guide future immunotherapy.
Contribution
The study reveals increased HLA-G and KIR expression in CRC and their variability within tumors, suggesting potential as biomarkers and therapeutic targets.
Findings
HLA-G was positive in 16.7% of CRC patient samples, with no staining in controls.
KIR positivity was significantly higher in CRC tissues compared to controls.
KIR expression varied within the same tumor and was associated with patient age.
Abstract
The immune system functions as a well-coordinated defense mechanism, protecting the host from both external pathogens and internal threats. Cancer cells often display surface antigens that the immune system can recognize as foreign, potentially triggering an immune response. However, many cancer cells evade detection by downregulating or completely losing these surface antigens. The immune system relies on the expression of surface antigens and human leukocyte antigens (HLA) to identify and target tumor cells. One key method by which tumor cells evade natural killer (NK) cells involves alterations in HLA antigens. Colorectal cancer (CRC) is known to cause various changes in the immune system, including the increased expression of HLA antigens on cell surfaces, reduced functionality of NK cells, and mechanisms for immune evasion. The aim of this study was to investigate the possible…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
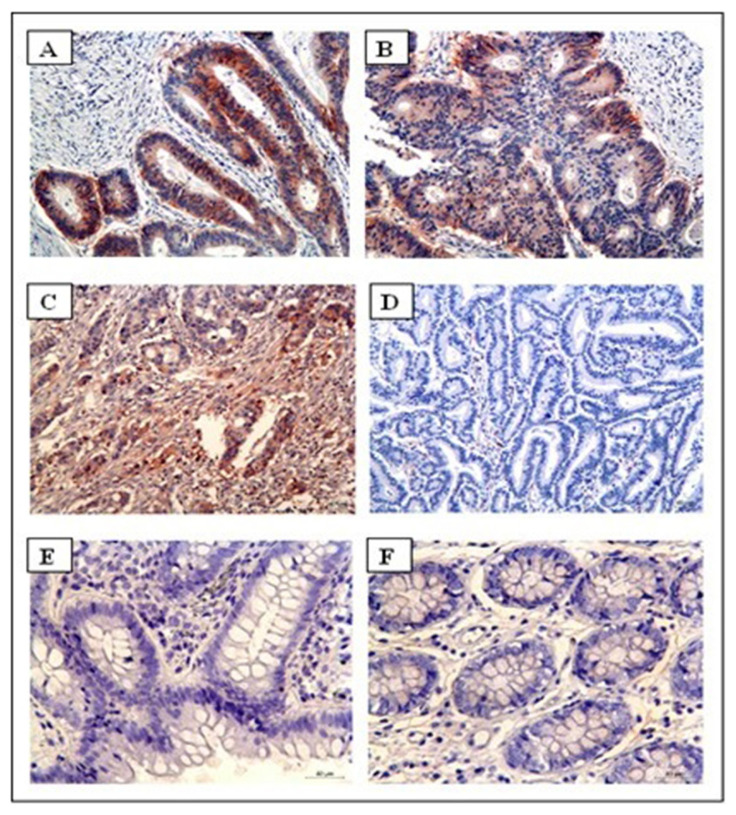 Figure 1
Figure 1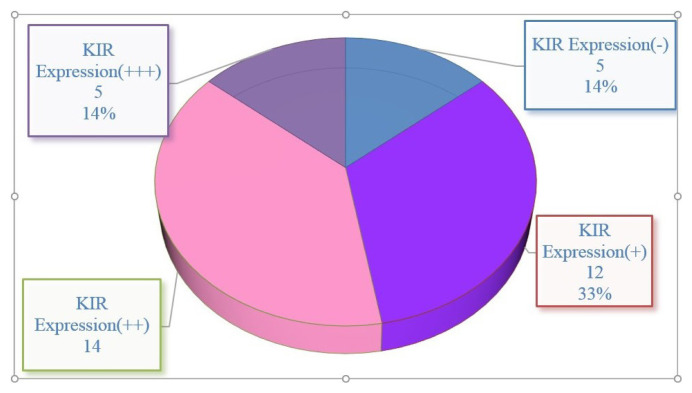 Figure 2
Figure 2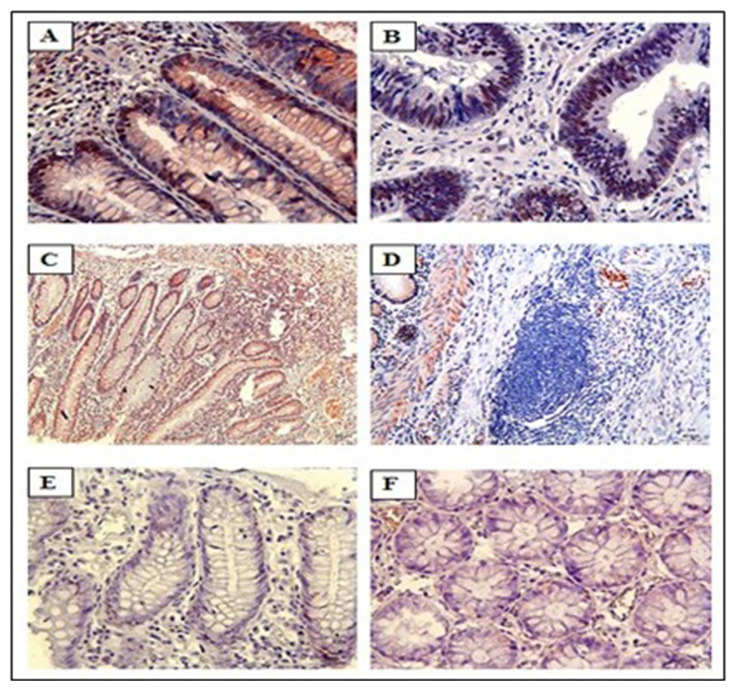 Figure 3
Figure 3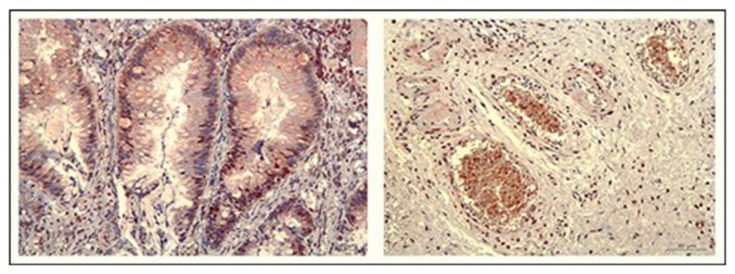 Figure 4
Figure 4- —İstanbul University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive System and Pregnancy · Immune Cell Function and Interaction · Urticaria and Related Conditions
Introduction
The immune system acts as a vital protective network, shielding the body from external threats as well as internal disruptions. In the context of cancer, tumor cells may express specific surface antigens that the immune system can recognize as foreign. This recognition has the potential to trigger an immune response. However, many cancer cells develop mechanisms to evade detection by reducing or entirely eliminating these surface antigens, making it challenging for the immune system to identify cancer cells as threats. For the immune system to function efficiently, the presence of both surface antigens and human leukocyte antigen (HLA) molecules is crucial, as they collaborate to help immune cells identify and attack cancerous cells.
A common strategy that tumor cells use to evade the immune system, particularly natural killer (NK) cells, involves modifications in HLA antigens [1–3]. These changes help the tumor cells avoid being identified and destroyed. Colorectal cancer (CRC), a prevalent and potentially fatal malignancy, disrupts various immune system processes [4, 5]. This includes altering HLA antigen expression on the cellular surface of tumors, impairing the function of NK cells, and facilitating immune evasion [6, 7]. These modifications can greatly impair the capability of the immune system to initiate a response against cancer cells [8, 9].
In the current study, the objective was to assess the soluble HLA-G (sHLA-G) in the blood serum of CRC patients using enzyme-linked immunosorbent assay (ELISA). Additionally, we examined the HLA-G expression loss in tumor tissues using immunohistochemistry (IHC), and we aimed to assess the infiltration of killer cell immunoglobulin-like receptors (KIRs) on NK cells within the tumor microenvironment. Through these analyses, our aim was to gain a deeper understanding of how CRC tumors avoid detection by the immune system and to identify potential therapeutic targets for future cancer therapies.
Materials and methods
2.1. Patient group
In this study, 36 individuals with a diagnosis of CRC were enrolled, including 24 males and 12 females. These patients underwent surgery at the General Surgery Clinic of İstanbul Bakırköy Dr Sadi Konuk Training and Research Hospital. The age range for the included patients was between 18 and 90 years. Blood samples were collected from each patient before surgery using serum-separating tubes. The collected samples were then preserved at −80 °C to be analyzed at a later stage. Tumor tissues were obtained during surgery and processed for IHC analysis.
The current study received approval from by the Clinical Research Ethics Committee of İstanbul University (approval date: 13 March 2017, protocol number: 2016/1350). Informed consent was obtained from all participants, and the research followed the ethical standards outlined in the Declaration of Helsinki.
2.2. Healthy control group
The control group consisted of 40 healthy volunteers, with 22 females and 18 males, all between the ages of 18 and 90 years. None of the individuals in this group had a history of acute or chronic illness, cancer, or previous treatments such as chemotherapy or radiotherapy. All healthy volunteers had undergone screening colonoscopies and provided informed consent for research purposes. Blood samples from the control participants were collected into tubes with EDTA, and the serum was preserved at −80 °C.
2.3. Immunohistochemistry
The colorectal tissue specimens were preserved using 10% neutral buffered formalin and were placed in paraffin blocks. Tissue slices were prepared from these blocks and transferred to glass slides. Samples were deparaffinized and rehydrated using a graded alcohol series. For IHC staining, the sections were exposed to primary antibodies targeting HLA-G (4H84, diluted 1:50, Santa Cruz Biotechnology, Dallas, TX, USA, catalog number: sc-21799) and KIR2DL4 Ab (rabbit polyclonal, diluted 1:7.5, Biorbyt, Cambridge, UK, catalog number: orb447529) according to the manufacturers’ guidelines. A negative control of PBS was applied instead of the primary antibody to check the immunolabelling, and all steps of the process were performed in the same manner. The slides were then treated using the hydrogen peroxide block/3-amino-9-ethyl-carbazole (HRP/AEC) antipolyvalent kit (Thermo Fisher Scientific, Waltham, MA, USA). A counterstain with hematoxylin was applied, and the stained slides were analyzed using a light microscope (Leica DM 2500, UK) coupled with a digital camera system (Leica DFC280, Germany). The staining intensity for each sample was categorized into 4 levels: no staining (−), weak staining (+), moderate staining (++), or strong staining (+++), following established criteria [10].
2.4. ELISA
Serum samples from CRC patients and healthy controls were analyzed for sHLA-G levels using ELISA. Prior to testing, the serum samples were centrifuged at 1000 rpm for 20 min. The Human HLA-G ELISA Kit (Abbkine Inc., China) was used following the manufacturer’s protocol [11], and absorbance was measured at 450 nm using an ELISA plate reader (Agilent, USA). The resulting data were used to determine sHLA-G concentrations in patient and control groups.
2.5. Statistical analysis
The data were processed using SPSS software version 21.0. For numerical variables, descriptive statistics (mean, standard deviation, minimum, and maximum values) were computed. Categorical variables were expressed as percentages. To check for normally distributed data, a Kolmogorov-Smirnov test was performed. For group comparisons, Student’s t-test was used when the data was normally distributed, whereas the Mann-Whitney U test was applied for nonnormally distributed data. Relationships between categorical variables were evaluated using Pearson’s chi-square test. A p-value below 0.05 was considered statistically significant.
Results
3.1. Demographic results
In this study, the CRC patient group was composed of 24 males (66.7%) and 12 females (33.3%), while the healthy control group included 18 males (45.0%) and 22 females (55.0%). The average age of the CRC patients was 62.33 ± 11.49 years, with an age range from 33 to 78. Conversely, the control group had a mean age of 50.03 ± 11.30, with ages ranging from 22 to 71.
3.2. HLA-G immunostaining results
IHC analysis was performed on tissue sections from 36 CRC patients, focusing on the expression of HLA-G. Cells displaying staining either on their membranes or within their cytoplasm were considered HLA-G positive. None of the 40 samples from the healthy control group were HLA-G positive. In the patient group, 16.7% (6 out of 36) of the tissue sections were HLA-G positive, while the remaining 83.3% (30 out of 36) were negative for HLA-G staining (Table 1). A statistically significant difference was observed between the CRC patients and healthy controls in terms of HLA-G expression (p = 0.009).
The staining intensity of HLA-G in the CRC samples was categorized as weak (+), moderate (++), or strong (+++). Of the 6 positive cases, 1 (2.8% of all cancer patients) had weak staining (p = 0.473), 3 cases (8.3%) had moderate staining (p = 0.101), and 2 cases (5.6%) had strong staining (p = 0.221). The comparison of staining intensity between patient and control groups did not show any statistically significant differences. The IHC staining of HLA-G for patient and control groups is shown in Figure 1. Figures 1A, 1B, and 1C show tumor samples. Figures 1D shows HLA-G immunostaining negativity for healthy tissue. Figure 1C shows the strongest HLA-G positivity for tumor samples. Figure 1D shows HLA-G immunostaining negativity for tumour samples, while Figures 1E and 1F show HLA-G immunostaining negativity for healthy control tissue.
HLA-G expression was primarily observed in the cell membrane in 11.1% of the samples, while faint cytoplasmic staining was noted in 2.7% of the cases. These results indicate that while a subset of CRC patients were HLA-G positive, the majority did not show significant HLA-G expression in their tissue samples.
3.3. Correlation between HLA-G and clinicopathological features
We examined how HLA-G expression correlated with various clinical and pathological features, such as patient age, sex, tumor invasion depth, lymph node status, and tissue grade. No significant correlations were found between HLA-G positivity and these factors, including cancer stage (p = 0.658) (Table 2). When cancers were grouped into early and advanced stages, HLA-G expression was observed in 5.6% (2 out of 18) of early-stage patients and 11.1% (4 out of 18) of advanced-stage patients.
3.4. Killer cell immunoglobulin-like receptor (KIR) immunostaining results
IHC staining for KIR expression had a significantly higher rate of KIR positivity in CRC tissue samples compared to control samples. Among the 36 CRC patient samples, 86% (31 out of 36) were positive for KIR staining. The staining intensity ranged from weak (+) to strong (+++), and heterogeneous staining patterns were observed across different regions of the same tumor. Figure 2 shows staining intensity. KIR expression was predominantly localized in the cell nucleus, with some cases also showing cytoplasmic staining. Representative microscopic images of IHC-stained samples are shown in Figure 3. Patients’ tumor samples can be seen in Figures 3A, 3B, and 3C. Figure 3D shows the negativity of KIR immunostaining for tumor samples. Figures 3E and 3F show the healthy control tissue. Figure 3A shows the strongest KIR positivity for tumor samples. A notable observation in our study was the variability in KIR staining intensity within the same tumor. Differences in KIR expression were observed not only between different tumors but also within distinct areas of the same tumor. KIR staining was mainly nuclear, although faint cytoplasmic staining was present in certain cases. Figure 4 shows KIR staining in tumor sites.
3.5. Correlation between KIR and clinicopathological features
We also investigated the relationship between KIR and clinicopathological factors, including tumor depth (T), lymph node (N), and metastasis (M) involvement as TNM stage. Among the 36 CRC patients, 83.3% of females and 87.5% of males were KIR positive, with no significant difference in KIR expression between sexes (p = 1). An analysis of the relationship between age (mean = 62.3 years) and KIR expression in the patient group showed that the mean age of individuals with KIR expression was 64.10 ± 10.36 years, whereas those without KIR expression had a mean age of 51.40 ± 0.35 years. This difference was statistically significant (p = 0.02). There were no meaningful associations identified between KIR and factors such as tumor stage, depth of invasion, or lymph node involvement.
3.6. Serum sHLA-G levels
Serum levels of sHLA-G were measured in both CRC patients and healthy controls. The median sHLA-G concentration in CRC patients was 227.78 ng/L, while the median concentration in the control group was 231.02 ng/L. No significant associations were observed between serum sHLA-G levels and clinicopathological factors, including cancer stage, tumor invasiveness, and the number of lymph nodes involved (p = 0.815).
3.7. Comparison of KIR, HLA-G, and sHLA-G
The analysis comparing KIR, HLA-G, and sHLA-G expression showed no notable correlation between KIR and sHLA-G levels (p = 0.707), nor between HLA-G and sHLA-G levels (p = 0.641). Among CRC patients, 86.1% were positive for KIR expression, whereas only 16.7% had HLA-G positivity. As no HLA-G or KIR expression was detected in the healthy control group, the significance of sHLA-G levels in controls was not analyzed further.
Discussion
CRC is recognized as a growing global health concern, with its incidence steadily increasing every year. Globally, CRC ranks as the third most diagnosed, while in Türkiye, it is the fourth most prevalent cancer [12, 13]. CRC is ranked second among cancer-related deaths globally [12, 14].
According to a 2023 report, more than 20 million new cancer cases were reported worldwide, with approximately 9.7 million deaths (48.5%), placing CRC as one of the leading causes of cancer mortality1.
Despite advancements in cancer treatment, the 5-year survival rate for CRC remains at approximately 65%2. These statistics emphasize the need for new therapeutic approaches, especially in the field of immunotherapy.
One of the key mechanisms that cancer cells use to evade immune system detection is the downregulation or alteration of surface antigens. These modifications enable tumor cells to avoid recognition and elimination by immune cells, including NK cells and cytotoxic T lymphocytes [15–17]. Effective immune surveillance depends on the proper expression of HLA on tumor cells. Alterations in HLA expression allow tumor cells to evade immune system responses, particularly those mediated by NK cells, which may lead to poor clinical outcomes [18–20].
Our study sought to investigate the expression of HLA-G and KIR markers in CRC tissues, as well as sHLA-G level in CRC patients. Our results showed a significant difference for HLA-G and KIR markers between CRC patients and healthy controls. Specifically, 16.7% of CRC tissue samples were HLA-G positive, while 86.1% were positive for KIR expression. These findings are consistent with previous research suggesting that increased HLA-G expression in tumor tissues is associated with immune evasion and a poor prognosis [21, 22]. The interaction between HLA-G and KIR likely plays a critical role in inhibiting NK cell activity, allowing tumor cells to evade destruction [23–25].
Several studies have reported elevated HLA-G expression in a variety of cancers, including lymphomas, lung cancer, and CRC [26–28]. For instance, a research group found that 65% of CRC tissue samples had HLA-G expression, while no expression was detected in normal colorectal tissues or benign adenomas [21]. Our findings are consistent with this, as we observed a higher expression of HLA-G in CRC tissues compared to healthy controls. The absence of HLA-G expression in healthy tissues further supports its role as a marker of malignant transformation and immune evasion [22].
In certain cancers, the absence of HLA-G expression is associated with better clinical outcomes, as it makes tumor cells more susceptible to lysis induced by NK cells [2]. The HLA-G positivity rate observed in our study (16.7%) was below that reported in previous studies. This could be attributed to the limited number of samples analyzed. Nevertheless, the strong association between HLA-G and KIR expression highlights their potential role in promoting immune evasion in CRC.
Interestingly, unlike some previous studies that have suggested elevated serum sHLA-G levels are correlated with poor prognosis and immune suppression [29, 30], we did not find a significant association between sHLA-G levels and clinicopathological factors in CRC patients. This discrepancy may be explained by differences in sample sizes, patient populations, or assay methodologies. In order to enhance our knowledge about the role of sHLA-G in CRC, future research involving larger patient groups are necessary.
In our analysis, a significant relationship between KIR expression and patient age was observed, with older patients showing higher levels of KIR positivity (p = 0.020). Despite this, no notable associations were identified between KIR and pathological features. The results indicate that age-related alterations in immune function could have an impact on KIR expression, though additional studies are needed to clarify the mechanisms involved.
Overall, our study highlights the importance of targeting HLA-G and KIR as potential therapeutic strategies for CRC. Blocking KIR receptors may enhance NK cell-mediated cytotoxicity, potentially improving clinical outcomes for CRC patients. Future research should focus on elucidating the mechanisms by which HLA-G and KIR interactions influence NK cell function and exploring how these pathways can be targeted for cancer immunotherapy.
Conclusion
The findings of this study indicate that HLA-G levels are markedly increased in CRC patients, indicating its critical role in helping tumor cells evade immune detection. By interacting with KIR receptors on NK cells, HLA-G contributes to the suppression of NK cell activity, allowing tumor cells to escape immune-mediated destruction. Although our lack of knowledge regarding the cell type responsible for KIR positivity in our findings is a significant limitation of our study, the use of methods such as double staining in future studies could resolve this uncertainty and support our belief that both HLA-G and KIR can serve as valuable prognostic markers.
Overall, our findings suggest that HLA-G and KIR have the potential to be promising targets for future cancer immunotherapies. Further research into their interactions with the immune system will be crucial for developing more effective treatments for CRC and improving patient outcomes. In particular, characterizing the genetic and functional properties of these interactions could contribute to the development of more targeted treatments against cancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Park HS Cho U Im SY Yoo CY Jung JH Loss of human leukocyte antigen class I expression is associated with poor prognosis in patients with advanced breast cancer Journal of Pathology and Translational Medicine 2019 53 2 75 85 10.4132/jptm.2018.10.11 30424591 PMC 6435992 · doi ↗ · pubmed ↗
- 2Madjd Z Spendlove I Pinder SE Ellis IO Durrant LG Total loss of MHC class I is an independent indicator of good prognosis in breast cancer International Journal of Cancer 2005 117 2 248 255 10.1002/ijc.21163 15900607 · doi ↗ · pubmed ↗
- 3Albertsson PA Basse PH Hokland M Goldfarb RH Nagelkerke JF NK cells and the tumour microenvironment: implications for NK-cell function and anti-tumour activity Trends in Immunology 2003 24 11 603 609 10.1016/j.it.2003.09.007 14596885 · doi ↗ · pubmed ↗
- 4Gambella A Scabini S Zoppoli G De Silvestri A Pigozzi S HLA-G as a prognostic marker in stage II/III colorectal cancer: not quite there yet Histochemistry and Cell Biology 2022 158 6 535 543 10.1007/s 00418-022-02141-w 35902421 PMC 9726768 · doi ↗ · pubmed ↗
- 5Guo ZY Lv YG Wang L Shi SJ Yang F Predictive value of HLA-G and HLA-E in the prognosis of colorectal cancer patients Cellular Immunology 2015 293 1 10 16 10.1016/j.cellimm.2014.10.003 25461612 · doi ↗ · pubmed ↗
- 6Garrido F Perea F Bernal M Sánchez-Palencia A Aptsiauri N The escape of cancer from T cell-mediated immune surveillance: HLA class I loss and tumor tissue architecture Vaccines (Basel) 2017 5 1 7 10.3390/vaccines 5010007 28264447 PMC 5371743 · doi ↗ · pubmed ↗
- 7Tersigni C Meli F Neri C Iacoangeli A Franco R Role of Human leukocyte antigens at the feto-maternal interface in normal and pathological pregnancy: An update International Journal of Molecular Sciences 2020 21 13 4756 10.3390/ijms 21134756 32635423 PMC 7370064 · doi ↗ · pubmed ↗
- 8Mao J Feng Y Zhu X Ma F The molecular mechanisms of HLA-G regulatory function on immune cells during early pregnancy Biomolecules 2023 13 8 1213 10.3390/biom 13081213 37627278 PMC 10452754 · doi ↗ · pubmed ↗