Absence of Internal Low Echoes Can Be an Important Diagnostic Clue for Intraductal Tubulopapillary Carcinomas of the Pancreas: A Case Report
Yurie Kitano, Shoji Oura

TL;DR
A case report highlights unique ultrasound features of intraductal tubulopapillary carcinoma of the pancreas, aiding in its diagnosis.
Contribution
Identifies absence of internal low echoes as a novel diagnostic clue for intraductal tubulopapillary carcinomas.
Findings
The tumor showed distinct margins, enhanced posterior echoes, and no internal low echoes.
The tumor lacked mucin production and caused less frequent icterus compared to other pancreatic tumors.
Abstract
Due to the low incidence of intraductal tubulopapillary neoplasms (ITPNs) of the pancreas, no typical images of them have been clarified. A 57-year-old man visited our hospital due to vomiting and abdominal pain. A blood test showed a high white blood cell count of 17,200/μL and a markedly elevated amylase level of 4,035 IU/L. CT showed swelling of the pancreatic head, which highly suggested a possible pancreatic head tumor. The patient received ulinastatin and antibiotic therapy for pancreatic head tumor-induced acute pancreatitis. An upper gastrointestinal endoscopy revealed a mass at the greater duodenal papilla. Endoscopic biopsy of the duodenal mass pathologically showed that the duodenal tumor was an adenoma. Endoscopic ultrasound showed common bile and main pancreatic duct dilatation and an oval mass with distinct margins, internal high echoes, and no posterior echo attenuation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
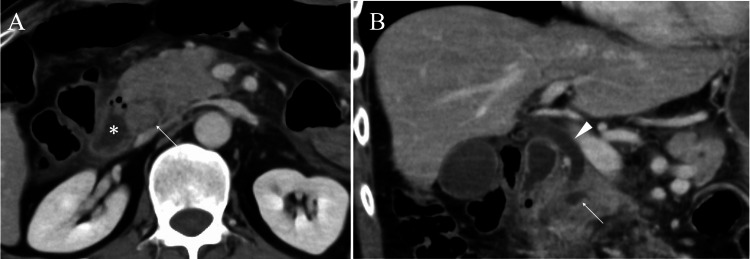 Figure 1
Figure 1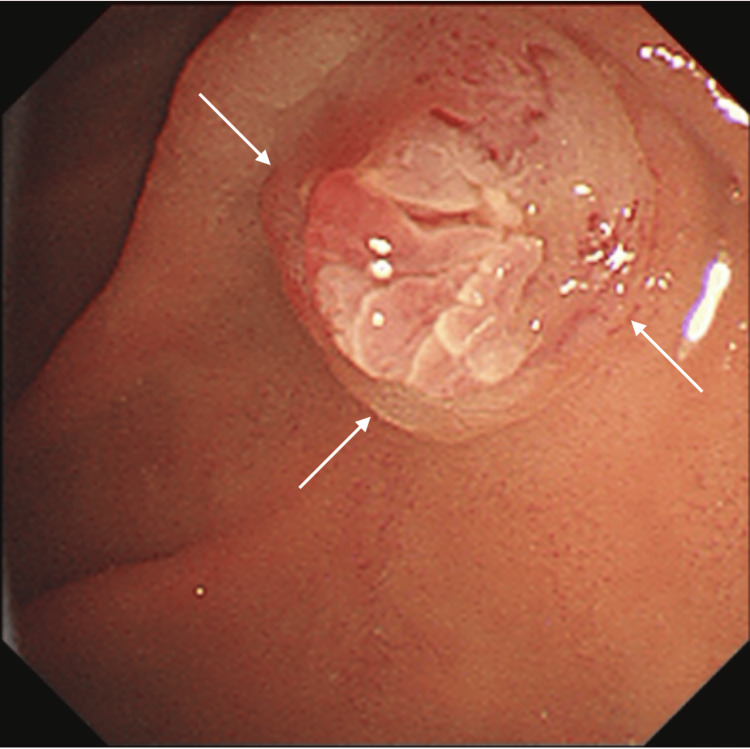 Figure 2
Figure 2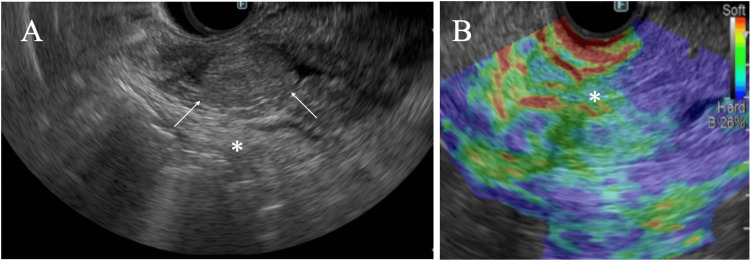 Figure 3
Figure 3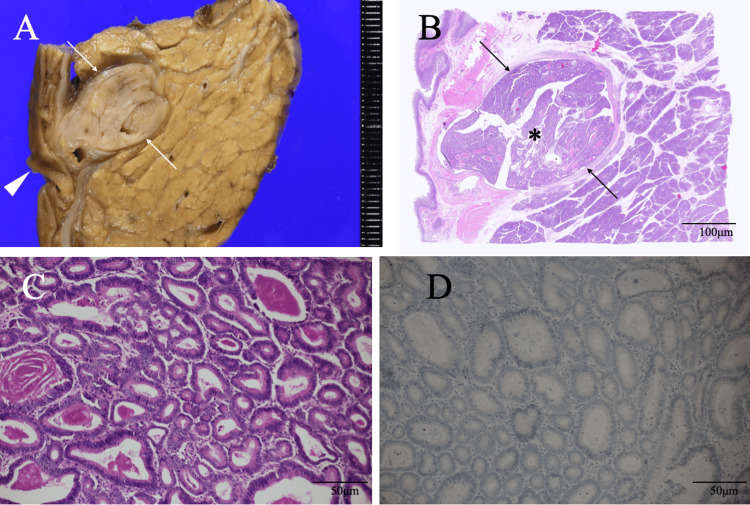 Figure 4
Figure 4| Characteristics | ITPN | IPMN | Adenocarcinoma | NET |
| Icterus | Rare | Possible | Possible | Possible |
| Mucin production | - | ++ | ± | ± |
| Echo findings | ||||
| Internal low echoes | None | Focally present | Frequent | Frequent |
| Posterior echoes | Enhanced | Enhanced | Attenuated | Enhanced |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Neuroendocrine Tumor Research Advances · Esophageal Cancer Research and Treatment
Introduction
Pancreatic cancer initially causes no specific symptoms and is often detected at advanced stages due to its anatomical characteristics. Although pancreatic cancer patients ultimately present various symptoms such as abdominal pain and weight loss [1], they are often unable to undergo curative resection even at their first symptom onset, generally showing extremely dismal clinical outcomes. On the other hand, patients with pancreatic head cancer tend to develop icterus and are sometimes able to undergo curative surgery after some kind of biliary drainage.
Intraductal tubulopapillary neoplasms (ITPNs) of the pancreas account for fewer than 1% of exocrine pancreatic tumors and non-invasive pancreatic cancers, have either high-grade dysplasia or non-invasive cancer components, and generally show growth patterns of tubule-forming structures [2]. In other words, they have both no or least fibrous components, often observed in pancreatic cancers, and the mass softness. In addition, ITPNs do not have mucin, unlike intraductal papillary mucinous neoplasms (IPMNs) [3,4]. These findings, therefore, rarely make ITPNs to cause icterus even when located at the pancreas head and quasi completely obstruct the main bile duct.
Like in the diagnosis of other solid malignancies, CT, MRI, and ultrasound are the mainstays in the diagnosis of pancreatic tumors. In addition, endoscopic retrograde cholangiopancreatography [5] and endoscopic ultrasound (EUS) [6] evaluations are imperative for diagnostic physicians to harvest the tissue of the target lesion in the pancreas. Typical image findings of ITPNs, however, remain uncertain due to the extremely low incidence of ITPNs.
Here, we report a rare case of ITPN arising in the pancreatic head without icterus, which makes us speculate that ITPNs have no internal low echoes due to their pathological structures.
Case presentation
A 57-year-old man with intellectual disability visited our hospital due to vomiting and abdominal pain. Communication difficulties of the patient prevented us from determining the exact location of the abdominal pain. A blood test showed a high white blood cell count of 17,200/μL (reference range: 3,300-8,600/μL) and a markedly elevated amylase level of 4,035 IU/L (reference range: 44-132 U/L) with a 99.9% (reference range: 28-72%) pancreatic-type subunit. In addition, CT showed swelling of the pancreatic head, which highly suggested a possible pancreatic head tumor and made us speculate that the pancreatic head tumor could have caused acute pancreatitis (Figure 1).
CT findings.(A) Axial view CT showing a presumed pancreatic head tumor (arrow) adjacent to the duodenum (asterisk). (B) Coronal view CT showing pancreatic (arrow) and bile (arrowhead) duct dilatation.
The patient, therefore, received ulinastatin and antibiotic therapy for pancreatic head tumor-induced acute pancreatitis, leading to the prompt normalization of elevated amylase levels and symptom relief. An upper endoscopy performed to investigate abdominal pain revealed a mass in the greater duodenal papilla (Figure 2).
Endoscopic findings.An upper gastrointestinal endoscopy revealing a protruded mass (arrows) at the greater duodenal papilla.
Pathological study of the biopsy specimen showed atypical cells growing in a glandular fashion in the duodenal mucosa and led to the pathological diagnosis of a duodenal adenoma. EUS showed common bile and main pancreatic duct dilatation and an oval mass around the bile duct-pancreatic duct junction with distinct margins, internal high echoes, and no posterior echo attenuation, highly suggesting that the pancreatic head mass had caused acute pancreatitis and could be a possible malignancy (Figure 3).
Endoscopic ultrasound (EUS) and elastography.(A) EUS showed a well-circumscribed mass (arrows) with internal high echoes and enhanced posterior echoes (asterisk). (B) Endoscopic elastography showed that the mass was expressed as greenish (asterisk).
Despite the lack of a definitive diagnosis of pathological malignancy, potential relapse of acute pancreatitis due to needle biopsy of the pancreatic head mass made us treat the patient with pancreatic head and duodenal resection, followed by regional node dissection to avoid undertreatment. Postoperative pathological study clarified the duodenal mass to be an intestinal-type adenoma and showed that the solid mass in the pancreatic duct was 18 mm in size and consisted of cuboidal to columnar atypical cells growing mainly in a tubular fashion with severe dysplasia and no mucin production around the tumor cells. Immunostaining of the tumor cells showed MUC5AC, MUC2, trypsin, and BCL1 negativity, leading to the diagnosis of intraductal tubulopapillary carcinoma (Figure 4).
Pathological findings.(A) The bisected mass was a solid mass (arrows) with clear borders near the greater duodenal papilla (arrowhead). (B) Low magnified view showed that the pancreas head mass (asterisk) was seen occupying almost the entire dilated pancreatic duct (arrows). (C) Magnified view showed atypical cells growing in a tubular fashion. (D) MUC5AC immunostaining showed no positive cells.
The patient recovered uneventfully, was discharged on the 11th day after the operation, and is scheduled to be followed up on an outpatient basis.
Discussion
Pancreatic cancer generally has abundant fibrous components, develops no symptoms until it becomes quite large or invades neighboring organs/tissues around the pancreas when located in the pancreatic body or tail, but causes bile duct and pancreatic duct stenosis or obstruction when located at the pancreatic head, sometimes leading to early detection of the pancreatic head cancer. In contrast, ITPNs only have delicate fibrovascular cores and lack fibrous component areas and are generally soft and well-demarcated tumors [2,7]. IPMNs also have no or least fibrous components but sometimes develop icterus when located at the pancreatic head and quasi obstruct the common bile duct [3,4]. Even if ITPNs are the same size and at the same location of pancreatic head IPMNs, they are less likely to cause icterus, presumably due to the mass softness and the lack of mucus.
Unlike icterus, ITPNs are prone to cause acute pancreatitis, as observed in this case. Diagnostic physicians, therefore, should strongly note that masses present in the pancreatic head, both with dilated bile and pancreatic ducts and no icterus, are highly ITPNs. In addition, when the target masses are judged as ITPNs on images and clinical findings, it is reasonable for attending surgeons to apply surgery to patients without pathological confirmation of the pancreatic head mass to avoid needle biopsy-induced pancreatitis.
It is well known that fibrous components not only give masses their hardness but also make mass margins unclear when present mixed with tumor cells at the tumor margins [8,9]. Conversely, ITPNs and IPMNs have no or least fibrous components at their mass margins, generally making their masses have well-circumscribed margins, a typical imaging finding.
EUS showed that the present ITPN had internal high echoes and enhanced posterior echoes. Internal high echos are formed through abundant ultrasound wave backscattering, which is generally caused by the presence of microvoids in papillary/tubular structures or of different acoustic impedance-bearing pathological components, e.g., fat [10]. ITPNs have tubulopapillary structures, including microvoids, and do not have areas of homogenous pathological components with similar acoustic impedance, which implies the lack of internal low echoes. In addition, fibrous components attenuate ultrasound waves, often causing posterior echo attenuation. ITPNs, however, have no or little fibrous components, which generally lead to making posterior echoes enhanced. IPMNs have similar pathological structures to those of ITPNs and naturally show predominant internal high echoes. IPMNs, however, always have mucinous areas within them and generally show at least focal low echoes or different internal high echoes to those caused by the papillary structures [11]. Therefore, it is imperative for diagnostic physicians to note that internal high echoes of IPMNs are slightly different from those of ITPNs (Table 1).
Although various etiologies of ampullary adenomas have been suggested, one of which is irritation by the bile [12]. Why an ampullary adenoma and an ITPN had coexisted closely remains naturally uncertain. However, it cannot be denied that the presence of ITPN in the pancreatic head may have increased the stimulation to the papilla, resulting in the development of the ampullary adenoma.
Well-defined tumors in the pancreas head, accompanied by bile duct and pancreatic duct dilation, with internal high echoes and enhanced posterior echoes, are likely to be ITPNs or IPMNs. In addition, when lacking icterus despite the presence of main bile duct dilatation, diagnostic physicians should suspect that the pancreatic head tumors are more likely to be ITPNs than IPMNs.
Conclusions
We highly speculate that both ITPNs and IPMNs can be located at the pancreatic head and show distinct margins due to the lack of fibrous components at mass borders. Diagnostic physicians should include ITPNs and IPMNs in the differential diagnosis of pancreatic head tumors when tumors have clear margins, no internal low echoes, and enhanced posterior echoes. In addition, when pancreatic head tumors have dilatation of the bile and pancreatic ducts and no icterus, physicians should strongly suspect them to be ITPNs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The risk of pancreatic cancer in symptomatic patients in primary care: a large case-control study using electronic records Br J Cancer Stapley S Peters TJ Neal RD Rose PW Walter FM Hamilton W 1940194410620122261712610.1038/bjc.2012.190PMC 3388562 · doi ↗ · pubmed ↗
- 2Pancreatic intraductal tubulopapillary neoplasm WHO Classification of Tumours: Digestive System Tumours Basturk O Esposito I Fukushima N 317318 Lyon International Agency for Research on Cancer 2019
- 3Histopathological diagnosis of pancreatic intraepithelial neoplasia and intraductal papillary-mucinous neoplasms: interobserver agreement Pancreas Longnecker DS Adsay NV Fernandez-del Castillo C 3443493120051625836810.1097/01.mpa.0000186245.35716.18 · doi ↗ · pubmed ↗
- 4An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms Am J Surg Pathol Hruban RH Takaori K Klimstra DS 9779872820041525230310.1097/01.pas.0000126675.59108.80 · doi ↗ · pubmed ↗
- 5Diagnosis of pancreatic carcinoma. Imaging techniques and tumor markers Pancreas Niederau C Grendell JH 668671992155734810.1097/00006676-199201000-00011 · doi ↗ · pubmed ↗
- 6Diagnostic endoscopic ultrasound: technique, current status and future directions Gut Liver Ang TL Kwek AB Wang LM 4834961220182929160110.5009/gnl 17348 PMC 6143442 · doi ↗ · pubmed ↗
- 7Intraductal tubulopapillary neoplasm of the pancreas: an update from a pathologist's perspective Arch Pathol Lab Med Rooney SL Shi J 1068107314020162768497810.5858/arpa.2016-0207-RA · doi ↗ · pubmed ↗
- 8Accurate pathological prediction of small breast cancer with pathological component-based image evaluation: a case report Cureus Kitano Y Oura S Honda M 017202510.7759/cureus.78026 PMC 1186121940013226 · doi ↗ · pubmed ↗