Challenges in Identifying Uncommon Clinical Isolates of Candida Species Using Conventional Phenotypic Methods: A Clinical Concern
Leimapokpam S Devi, Mukesh Sharma, Moumita Sardar

TL;DR
This study shows that traditional methods for identifying Candida species, especially rare ones like C. auris, are unreliable, leading to potential misdiagnosis and treatment issues.
Contribution
The study evaluates the limitations of conventional and chromogenic methods in identifying uncommon Candida species in a rural hospital setting.
Findings
Conventional phenotypic and chromogenic methods failed to accurately identify Candida auris.
Non-albicans Candida species showed higher resistance to antifungals like fluconazole and voriconazole.
Long-term antibiotic use was the most common risk factor for Candida infections in the study population.
Abstract
Background Candida species, particularly non-albicans Candida species, have emerged as a major cause of human infection, often exhibiting multidrug resistance due to either acquired or intrinsic resistance to antifungals. Therefore, accurate speciation of Candida isolates is crucial. However, despite reported misidentification issues with conventional methods, many mycology laboratories, including those in resource-poor healthcare facilities, still rely on them. This study compared various Candida speciation methods, including conventional phenotypic methods, chromogenic media, and the VITEK 2 compact system (bioMérieux, Marcy l'Etoile, France), and assessed the antifungal susceptibility patterns of clinical isolates at a rural tertiary care hospital. Methodology This prospective cross-sectional study was conducted from May 2024 to April 2025. Candida species were isolated from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
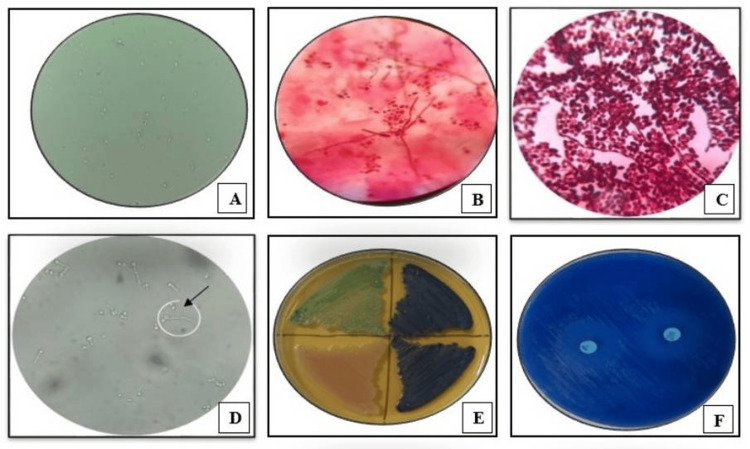 Figure 1
Figure 1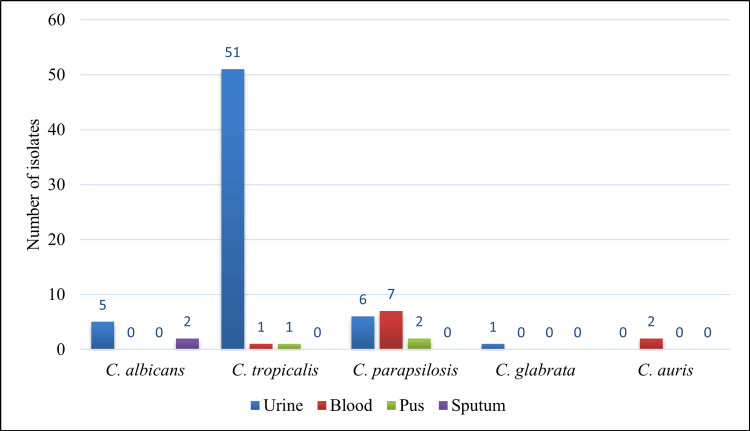 Figure 2
Figure 2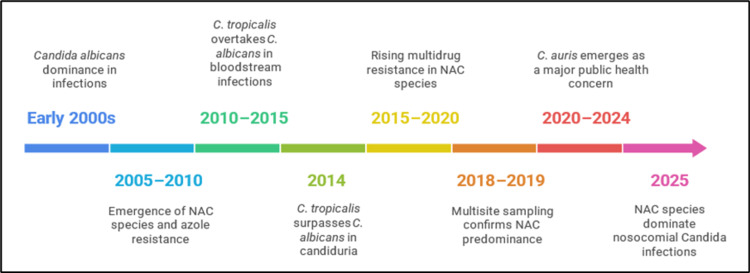 Figure 3
Figure 3| Variables | Description | |
| Age (years) | Range | 2-79 |
| Mean ± SD | 42.3 ± 18.9 | |
| Gender | Male | 37 (47.4%) |
| Female | 41 (52.6%) | |
| Male:female | 1:1.1 | |
| Patients attending | IPD | 58 (74.4%) |
| OPD | 20 (25.6%) | |
| Risk factors | Present in (total = 78) No. (%) | Type of | Statistical analysis (odds ratio) | |||
|
| NAC (n = 71) No. (%) | Odds ratio | 95% CI | p-value | ||
| Diabetes | 13 (16.7) | 5 (38.5) | 8 (61.5) | 19.68 | 3.26-118.78 | 0.001 |
| Chronic kidney disease | 6 (7.7) | 2 (33.3) | 4 (66.7) | 6.7 | 0.97-45.9 | NS (0.05) |
| Urinary catheterization | 8 (10.3) | 3 (37.5) | 5 (62.5) | 9.9 | 1.71-57.05 | 0.01 |
| Mechanical ventilation | 6 (7.7) | 2 (33.3) | 4 (66.7) | 6.7 | 0.97-45.9 | NS (0.05) |
| Long-term antibiotic use | 16 (20.5) | 6 (37.5) | 10 (62.5) | 36.6 | 3.97-337-03 | 0.001 |
| Long periods in intensive care unit | 11 (14.1) | 4 (36.4) | 7 (63.6) | 12.1 | 2.25-65.94 | 0.003 |
| Immunosuppression | 4 (5.1) | 1 (25) | 3 (75) | 3.7 | 0.33-42.15 | NS (0.28) |
|
| Carbohydrate fermentation test | Carbohydrate assimilation test | |||||||
| Glucose | Sucrose | Maltose | Lactose | Glucose | Sucrose | Lactose | Trehalose | Raffinose | |
|
| F | - | F | - | A | A | - | A | - |
|
| F | F | F | - | A | A | - | A | - |
|
| F | - | - | - | A | A | - | A | - |
|
| F | - | - | - | A | - | - | A | - |
|
| Conventional methods | HiCrome | VITEK 2 YST ID No. (%) | ||||
| No. (%) | Sensitivity (%) | Specificity (%) | No. (%) | Sensitivity (%) | Specificity (%) | ||
| C. albicans | 7 (9) | 100 | 100 | 7 (9) | 100 | 100 | 7 (9) |
| C. tropicalis | 53 (68) | 100 | 100 | 52 (66.7)¥ | 98.1 | 100 | 53 (68) |
| C. parapsilosis | 17 (21.8) | 100 | 96.9 | 16 (20.5)€ | 100 | 98.4 | 15 (19.2) |
| C. glabrata | 1 (1.2) | 100 | 100 | 0 (0) | 0 | 0 | 1 (1.2) |
| C. auris | 0 (0)* | 0 | 0 | 0 (0)* | 0 | 0 | 2 (2.6) |
| Total | 78 (100) | - | - | 75 (96.2) | - | - | 78 (100) |
| Antifungal agents | Antifungal resistance | ||||||
| Total (n = 78) No. (%) |
| Non-albicans | |||||
| Total (n = 71) No. (%) |
|
|
|
| |||
| Fluconazole | 45 (57.7) | 3 (42.9) | 42 (59.2) | 27 (50.9) | 12 (80) | 2 (100) | 1 (100) |
| Itraconazole | 52 (66.7) | 3 (42.9) | 49 (69) | 34 (64.2) | 12 (80) | 2 (100) | 1 (100) |
| Voriconazole | 47 (60.3) | 3 (42.9) | 44 (62) | 33 (62.3) | 8 (53.3) | 2 (100) | 1 (100) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Pneumocystis jirovecii pneumonia detection and treatment
Introduction
Candida species have emerged as a major cause of human infection over the past two decades, leading to high mortality rates [1-3]. While it is a commensal in the mucosal oral cavity, gastrointestinal tract, and vagina in healthy humans, it is considered an opportunistic fungal pathogen causing superficial infections of skin and mucous membranes to systemic life-threatening invasive infections [1,3,4]. The high mortality rates associated with Candida infections could be due to the increasing incidence of invasive and septicemic infections, particularly among immunocompromised individuals [3]. Globally, Candida species have been recognized as a leading cause of hospital-acquired infections, with systemic Candida infections ranking fourth among the most common causes of bloodstream infections (BSIs) acquired in hospitals [3,5]. Among Candida species, Candida albicans is the most prevalent species globally, with the exception of a few Asian nations where non-albicans Candida (NAC), specifically Candida tropicalis, is the predominant species [6,7]. An Indian study revealed an alarming prevalence, with NAC isolates accounting for 63.3% of cases, and C. tropicalis being the most prevalent, followed by Candida glabrata and Candida krusei [8].
Despite the fact that clinical manifestations of infections associated with different members of NAC are usually indistinguishable, several NAC species either acquire resistance over time or have intrinsic resistance against commonly used antifungals [5]. Several virulence factors facilitate the transition of Candida species from commensal to a potent pathogen, including adherence to host tissues and medical devices, formation of biofilm, secretion of extracellular hydrolytic enzymes (e.g., proteases, lipases, phospholipases, esterases, and phosphatases), toxins, complement receptors, and phenotypic switching [9]. Therefore, identification of Candida isolates to the species level is essential for effective treatment of patients with Candida infections.
While several studies have reported the prevalence and distribution of Candida species in different clinical settings, there is a lack of information on their characterization and susceptibility patterns in rural tertiary care centers, where these facilities often face challenges, such as limited resources, lack of specialized expertise, and delayed access to diagnostic facilities. These factors can impact the timely identification and management of Candida infections, potentially leading to suboptimal treatment outcomes [10]. Moreover, conventional phenotypic methods for Candida speciation, which commonly use morphological and biochemical properties of each species, often misidentify uncommon Candida species such as Candida kefyr, Candida auris, and Candida lusitaniae [11]. Therefore, this study aimed to compare Candida speciation methods, including conventional phenotypic methods, growth on chromogenic medium, and the VITEK 2 compact system (bioMérieux, Marcy l'Etoile, France), among Candida species isolated from various clinical samples from patients attending a rural tertiary care hospital. Additionally, the antifungal susceptibility pattern of the isolates to widely used antifungal drugs was assessed.
Materials and methods
This prospective cross-sectional study was conducted from May 2024 to April 2025 at the Microbiology Laboratory, Shree Guru Gobind Singh Tricentenary (SGT) Hospital, Haryana, India. The study protocol received approval from the Institutional Ethical Committee (IEC/FMHS/PhD/2023-05).
Study population
Inclusion Criteria
Patients of all ages and genders with clinically suspected candidiasis who provided written consent were included in the study. A pre-designed proforma, adapted from a CDC document [12], was used to collect information on age, gender, and other demographic characteristics, as well as risk factors such as diabetes, recent surgery, long-term antibiotic use, and use of indwelling medical devices, for further data analysis.
Exclusion Criteria
Patients receiving antifungal therapy were excluded to prevent potential interference with the antifungal susceptibility testing results.
Collection of Candida isolates
Candida species (n = 78) were isolated from various clinical specimens, including blood, sputum, pus, and urine from the study population by standard microbiological techniques. The isolates were subsequently included in the study for further speciation using standard conventional phenotypic methods, growth on chromogenic Candida differential medium (HiCrome *Candida *differential agar), and the VITEK 2 compact system. Isolation of Candida species was performed by subculturing on Sabouraud dextrose agar (SDA) supplemented with chloramphenicol. Blood cultures were processed using the BacT/Alert system (bioMérieux, Marcy l'Etoile, France), and after flagging positive, subcultures were done on SDA for Candida isolation. All inoculated SDA tubes were incubated at 37°C for 24-48 hours, and the isolates were further subjected to various methods for speciation and antifungal susceptibility testing (Figure 1).
Identification and antifungal susceptibility testing of Candida species(A) Potassium hydroxide mount of sputum sample showing budding yeast cells (40x). (B) Gram stain of sputum sample showing Gram-positive budding yeast cells with pseudohyphae (100x). (C) Gram stain of fungal culture showing Gram-positive budding yeast cells with pseudohyphae (100x). (D) Germ tube test positive, wet mount preparation (40x). (E) HiCrome Candida differential agar showing differential growth of Candida species, Candida albicans (light green), Candida tropicalis (blue), and Candida glabrata (cream). (F) Antifungal susceptibility testing of Candida species on Mueller-Hinton agar supplemented with methylene blue
Methods for speciation of Candida isolates
Conventional phenotypic methods for Candida speciation, such as the germ tube test, growth at 45°C, carbohydrate fermentation, and carbohydrate assimilation, were performed [13]. For the germ tube test, isolates showing characteristic germ tube formation within 2-3 hours of incubation in human serum at 37°C were considered positive. For growth at 45°C, isolates with positive germ tube test results were inoculated on SDA and incubated at 45°C for 48 hours; C. albicans grows at this temperature, helping to differentiate it from Candida dubliniensis, which is also a germ tube-positive Candida species. Carbohydrate fermentation was carried out using Andrade peptone water with individual carbohydrates (glucose, maltose, lactose, and sucrose), and acid and gas production were observed to determine the fermentative capability of the isolate. Carbohydrate assimilation testing involved assessing the ability of Candida isolates to utilize different carbohydrates as the sole carbon source, evaluated by growth in media containing individual carbohydrates.
HiCrome Candida differential agar (HiMedia Laboratories Pvt. Ltd., Mumbai, India) was used to differentiate Candida species based on colony color and morphology, with species-specific chromogenic reactions aiding in identification. Species-specific colony colors are as follows: light green colonies for C. albicans, cream to white for C. glabrata, metallic blue colonies for C. tropicalis, purple fuzzy colonies for C. krusei, and white to cream color colonies for C. parapsilosis. The VITEK 2 compact system is an automated system with fluorescence-based detection and colorimetric technology that employs a VITEK 2 YST ID card, utilizing 46 biochemical reactions for rapid and accurate yeast species, specifically for Candida isolates within 18-24 hours [14].
Antifungal susceptibility testing for all the Candida isolates was performed using the disc diffusion method and interpreted according to Clinical and Laboratory Standards Institute (CLSI) guidelines [15]. The following antifungal discs from HiMedia Laboratories Pvt. Ltd., India, were used: fluconazole (25 µg), itraconazole (10 µg), and voriconazole (1 µg). C. albicans ATCC 90028 and C. tropicalis ATCC 750 were used as quality control strains.
Statistical analysis
Data on categorical variables including antifungal susceptibility results were expressed as frequencies and percentages. Comparisons of conventional phenotypic methods, growth on chromogenic medium, and the VITEK 2 compact systems for speciation of *Candida *isolates were evaluated using the Chi-squared test. The association between risk factors with *Candida *infections was analyzed by using the odds ratio [16]. A p-value < 0.05 was considered statistically significant.
Results
A total of 78 Candida species were isolated from various clinical specimens obtained from patients attending different clinical departments. The patients’ ages ranged from two to 79 years, with a mean age of 42.3 years. The majority of the patients were women (52.6%), while men accounted for 37 cases (47.4%). Among the 78 patients, 58 (74.4%) were from inpatient departments (IPD) and 20 (25.6%) were from outpatient departments (OPD) (Table 1).
The distribution of Candida species by specimen revealed varied manifestations, with the majority isolated from urine (n = 44; 56.4%), followed by blood (n = 19; 24.4%), pus (n = 6; 7.7%), and sputum (n = 9; 11.5%). A total of seven Candida isolates were identified as C. albicans, while the remaining isolates were NAC species. The majority (five out of seven) of the C. albicans were from urine samples, and two were isolated from sputum samples (Figure 2). All Candida isolates from blood and pus were NAC species. Of the 53 C. tropicalis isolates identified, 51 (96.2%) were isolated from urine, while the other two isolates were obtained from blood and pus. Seven out of 15 C. parapsilosis isolates were obtained from blood, six from urine, and two from pus. All C. auris isolates were from blood, whereas a C. glabrata strain was obtained from urine. When the distribution of Candida species by specimen type and patient type was assessed, no statistical significance was observed (p > 0.05, calculated using the χ^2^ test).
Distribution of Candida species among various clinical specimens
Risk factor analysis of patients with Candida infections indicated that long-term antibiotic use (22.5%) followed by diabetes (16.7%) and prolonged intensive care unit (ICU) stays (14.1%) were frequently associated factors (Table 2). The odds of exposures, including diabetes, urinary catheterization, long-term antibiotic use, and prolonged ICU stays, were higher among patients with C. albicans infections than those with NAC species infections, highlighting a positive association of these risk factors and C. albicans infections. However, there was no statistically significant difference between the two types of infections in terms of chronic kidney disease, mechanical ventilation, and immunosuppression (p < 0.05).
Comparison of various Candida speciation methods for accuracy
The identification of Candida species was performed using standard conventional tests, including the germ tube test, growth at 45°C, carbohydrate fermentation, and assimilation tests. Out of the 78 clinical isolates, seven (9%) tested positive in the germ tube test, confirming their identification as C. albicans/C. dubliniensis, while the remaining 71 (91%) germ tube-negative isolates were classified as NAC. Furthermore, growth at 45°C was observed in all the germ tube-positive Candida isolates. Patterns of carbohydrate fermentation and assimilation by the Candida isolates revealed that seven of the isolates were those of C. albicans. The remaining NAC species included 53 isolates of C. tropicalis, 17 isolates of C. parapsilosis, and one isolate of C. glabrata (Table 3). C. albicans fermented glucose and maltose with acid and gas production, while it assimilated glucose, sucrose, and trehalose. C. tropicalis fermented glucose, sucrose, and maltose with acid and gas production, while it assimilated glucose, sucrose, and trehalose. C. parapsilosis fermented glucose while it assimilated glucose, sucrose, and trehalose. C. glabrata fermented glucose, whereas it assimilated both glucose and trehalose.
Based on colony color and morphology on HiCrome Candida differential agar, the majority (52/78) of the Candida isolates were identified as C. tropicalis, followed by C. parapsilosis (16/78) and C. albicans (7/78). Three Candida isolates could not be identified due to non-specific colony color and morphology on the chromogenic medium (Table 4).
All Candida isolates were subjected to an automated identification system using the VITEK 2 YST ID, which was considered the reference method due to its ability to identify uncommon Candida species. The most frequently isolated Candida species was C. tropicalis (53/78), followed by C. parapsilosis (15/78), C. albicans (7/78), C. auris (2/78), and C. glabrata (1/78) (Table 4).
The comparison of results from different phenotypic methods used to speciate the 78 Candida species is shown in Table 4. The VITEK 2 YST ID was considered the reference method for speciation, and subsequent comparisons with other methods were conducted. For the identification of C. albicans, C. tropicalis, and C. glabrata, the agreement between conventional methods and the VITEK 2 YST ID was 100%. For the identification of C. parapsilosis, the sensitivity and specificity of conventional methods were found to be 100% and 96.9%, respectively. Although Candida species may be rapidly and cost-effectively identified using HiCrome Candida differential agar, non-specific or atypical colony color or morphology may result in misidentification. The specificity for identifying C. tropicalis using chromogenic medium was 100%, while the sensitivity was 98.1%. For the identification of C. parapsilosis, the sensitivity and specificity were 100% and 98.4%, respectively. Both conventional methods and chromogenic medium misidentified or failed to identify C. auris strains. These findings emphasize the utility of combined phenotypic methods for preliminary identification and highlight the importance of automated systems like the VITEK 2 YST ID for accurate identification, especially of phenotypically similar or emerging Candida species.
Antifungal resistance profile
Overall, the antifungal resistance profile of Candida isolates was 57.7% for fluconazole, 66.7% for itraconazole, and 60.3% for voriconazole (Table 5). Although the number of C. albicans isolates was lower compared to NAC species, their antifungal resistance profiles were analyzed. NAC species showed higher resistance to all antifungals tested compared to C. albicans, although the difference was statistically insignificant. The two C. auris isolates and one C. glabrata isolate exhibited resistance to all antifungals, i.e., fluconazole, itraconazole, and voriconazole. C. parapsilosis also showed higher resistance to the antifungals (53.3% to 80%).
Discussion
Fungi, previously deemed non-pathogenic or less virulent, are now acknowledged as a primary contributor to morbidity and mortality in immunocompromised and critically ill patients [9]. The incidence of Candida infections, mostly opportunistic infections in immunocompromised individuals, has been increasing globally [3]. In immunocompromised individuals, Candida species can cause invasive infections that may disseminate to internal organs. Furthermore, new treatments for various diseases, surgery, long-term ICU stays, and earlier broad-spectrum antibiotic usage have increased the number of immunosuppressed individuals, thereby increasing the incidence of disseminated candidiasis [2,3,17].
Globally, C. albicans was once the predominant etiological agent causing candidiasis. However, a recent trend toward NAC species has been reported [7,8]. A comparable pattern has been observed in the present study, highlighting a notable shift toward an increasing incidence of Candida infections due to NAC species, such as C. tropicalis, C. parapsilosis, C. auris, and C. glabrata. In contrast to earlier studies conducted at the same hospital, which reported incidence rates of C. albicans infections as 51.6% (years 2011-2013) [18] and 40% (years 2016-2019) [19], the present study shows a significant decline in C. albicans infections to 9%, indicating a changing epidemiology of Candida infections. Among NAC species, C. tropicalis is often associated with nosocomial infections and has been reported as the second most commonly isolated species after C. albicans [20]. This is corroborated by the present study, which identified C. tropicalis as the most frequently isolated NAC species (74.6%, 53/71). A timeline for the evolution of clinical isolates of Candida species in Indian healthcare settings is depicted in Figure 3. This finding is consistent with the significant shift reported by Deorukhkar et al. from Western India, who found that 63.3% (331/523) of Candida species isolated from various clinical specimens were NAC species, with C. tropicalis (35.1%, 116/331) being the most predominant species, followed by C. glabrata (28.1%) and C. krusei (16.3%) [8]. Furthermore, Ahmed et al. from Northern India reported a higher frequency of NAC species (85.9%, 61/71) among Candida isolates from blood cultures, with C. tropicalis (35.2%) as the most common species, followed by C. glabrata (21.1%) and C. krusei (9.9%). Additionally, rare Candida species such as Candida guilliermondii, Candida pelliculosa, and Candida utilis have been reported [21]. BSIs caused by C. auris are associated with high mortality rates of 30%-60% [22]. In the present study, all Candida isolates from blood cultures were identified as NAC species, including two C. auris strains, and were obtained from hospitalized patients. A study by Rajni et al. conducted in ICUs of two hospitals in Northwestern India reported C. auris as the predominant Candida species, constituting 42% of candidemia cases, which is consistent with other studies showing C. auris as an emerging cause of concern in Indian healthcare settings [23].
Evolution of Candida species in clinical settings in IndiaImage credits: Sardar M generated this image using Napkin AI tool (accessed on August 9, 2025), using findings from references [19,21-27]
The increasing prevalence of infections caused by NAC species has been reported, accounting for more than 50% of invasive candidiasis in a sentinel-surveillance study in the United States and Canada [2]. In the present study, although the majority of NAC species were isolated from urine (81.7%), over half of the C. parapsilosis and all C. auris isolates originated from candidemia patients. The significant incidence of urinary tract infections attributed to Candida species highlights the emergence of this fungus as a notable etiology, particularly in IPD patients (70%, n = 44). Similar to our findings, Deorukhkar et al. reported that the majority of Candida isolates were from urine, with 60.8% identified as NAC species and 39.2% as C. albicans [8]. In addition to being better adapted to the urinary system, NAC species are more challenging to eliminate than C. albicans [7]. Risk factors such as the presence of urinary catheters, constant exposure to antifungal drugs, urinary abnormalities, advanced age, diabetes mellitus, abdominal surgeries, and pregnancy are frequently associated with candiduria [24]. Overall risk factor analysis of patients in the present study revealed prolonged antibiotic usage, diabetes, and extended ICU stays as frequently associated factors. Aruna and Jahappriya found diabetes mellitus to be the most frequently associated risk factor among patients with various Candida infections [25]. Another study reported an increased risk of acquiring nosocomial Candida BSIs in severe COVID-19 patients who had prolonged ICU stays, multiple courses of broad-spectrum antibiotics, mechanical ventilation, and other invasive devices [23].
Phenotypic methods are predominantly used for diagnosing fungal infections in Asia, with 81.7% of laboratories depending on non-commercial phenotypic methods and 44.7% also employing commercial phenotypic methods used for identifying Candida species [11]. The present study evaluated the accuracy of various phenotypic methods employed for the identification of Candida species. Phenotypic methods, including conventional methods such as the germ tube test, growth at 45°C, carbohydrate fermentation and assimilation tests, and growth on HiCrome Candida differential agar, were compared with the results obtained through the automated VITEK 2 compact system. The VITEK 2 YST ID identified two C. auris strains among the Candida isolates, whereas conventional methods erroneously identified both strains as C. parapsilosis. Additionally, growth on HiCrome Candida differential agar resulted in the inability to identify two C. auris strains, one C. tropicalis, and one C. glabrata due to non-specific colony color on the medium. A high rate of misidentification of uncommon Candida species by conventional methods has been reported [11]. The present study found 100% sensitivity for phenotypic conventional methods in identifying Candida species, including the germ tube test, growth at 45°C, and carbohydrate fermentation and carbohydrate assimilation tests. The specificity for identifying C. parapsilosis was 96.9%, attributed to the misidentification of two C. auris strains as C. parapsilosis. Although phenotypic conventional methods are considered the gold standard for identifying Candida species, they are labor-intensive and time-consuming. Additionally, it has been reported that there is no reliable phenotypic conventional method to accurately distinguish between closely related germ tube test-positive Candida species, often leading to misidentification of C. dubliniensis and Candida africana strains as C. albicans in clinical mycology laboratories [26]. Moreover, recently identified uncommon Candida species, e.g., C. auris, may be misidentified as several other organisms when using conventional or traditional phenotypic methods for yeast identification [27]. In the present study, all the C. albicans strains were accurately identified by HiCrome Candida differential agar; however, the sensitivity and specificity for identifying NAC species were 87.2% and 98.6%, respectively. Mutlu Sariguzel et al. evaluated the performance of CHROMagar Candida, VITEK 2 YST, and VITEK MS for identifying Candida isolates. In their study, two Candida isolates were misclassified as C. parapsilosis by CHROMagar Candida, and the speciation of C. glabrata was inconsistent with the reference method [28]. Saxena et al. reported that the VITEK 2 system accurately differentiated closely related Candida species, including uncommon species of Candida such as C. albicans, Candida famata, Candida ciferrii, Candida gulleri, and C. tropicalis, using 15 h using the VITEK 2 system, in contrast to identification by growth on chromogenic medium [29]. According to Esmat et al., the VITEK 2 demonstrated a sensitivity of 96% and specificity of 100% in accurately identifying Candida species, outperforming CHROMagar, which showed a sensitivity of 89% and specificity of 100% [30].
NAC species infections have clinical manifestations similar to those of C. albicans infections; however, they differ in terms of epidemiology, virulence factors, and especially the pattern of resistance to antifungal drugs [2,7,8]. Multidrug-resistant strains including C. auris have been reported among NAC species due to their ability to evade the mechanisms of action of different antifungal drugs, thus developing resistance. Additionally, some of these Candida species have demonstrated the ability to evade host immunity. The present study revealed that NAC species exhibited higher resistance to fluconazole and itraconazole, while C. albicans showed slightly higher resistance to voriconazole. This resistance to azoles may be attributed to alterations in target enzymes, limited drug access to the target, or a combination of both. Consequently, the significant resistance to azoles, which are the primary treatment choices, poses significant challenges in clinical practice. Our findings are in concordance with those of Deorukhkar et al. and Aruna and Jahappriya, which revealed that NAC species exhibited higher resistance to azoles than C. albicans in isolates from diverse specimens [8,25]. These findings suggest that the widespread or injudicious use of azoles has contributed to the development of resistance to these commonly relied upon antifungal drugs. Accurate identification of NAC species, especially C. auris, is therefore essential for effective treatment and infection prevention.
The limitations of this prospective cross-sectional study include a relatively small sample size and the restricted carbohydrate panel used in fermentation and assimilation tests for Candida species identification. Another limitation was its focus solely on azoles, whereas a more comprehensive approach would have included other antifungal classes, such as polyenes (e.g., amphotericin B) and pyrimidines (e.g., flucytosine), as well as newer antifungal drugs, e.g., caspofungins. Furthermore, determining the minimum inhibitory concentration for each antifungal drug by C. albicans and NAC species would have provided more nuanced and clinically relevant results, enabling healthcare providers to make more informed treatment decisions and optimize patient care.
Conclusions
The present study highlights an increasing trend of NAC species as the predominant cause of Candida infections among patients in rural Haryana, India. This worrisome emergence of NAC spp., almost replacing the commonly isolated species C. albicans in rural communities, deserves attention to promote accurate identification of Candida species and regular antimicrobial surveillance, which is necessary to monitor changes in antifungal resistance patterns.
Accurate identification of clinical Candida isolates is crucial for choosing the right antifungal treatment, as NAC species often show increased resistance to antifungals. Although rapid and reliable automated systems, such as the VITEK 2 compact system, and molecular diagnostic methods are available, their high cost restricts widespread use, making conventional techniques the primary means of identifying Candida species in most clinical laboratories, including those in developing countries. However, misidentification of rare Candida spp. such as C. auris by the conventional method often occurs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology and antifungal susceptibility patterns of invasive fungal infections (IF Is) in India: a prospective observational study J Fungi (Basel) Dabas Y Xess I Pandey M 33820213504997410.3390/jof 8010033 PMC 8777790 · doi ↗ · pubmed ↗
- 2Epidemiology and outcomes of invasive candidiasis due to non-albicans species of Candida in 2,496 patients: data from the Prospective Antifungal Therapy (PATH) registry 2004-2008 P Lo S One Pfaller MA Andes DR Diekema DJ 09201410.1371/journal.pone.0101510 PMC 408156124991967 · doi ↗ · pubmed ↗
- 3Resistance of Candida to azoles and echinocandins worldwide Clin Microbiol Infect Pristov KE Ghannoum MA 7927982520193096510010.1016/j.cmi.2019.03.028 · doi ↗ · pubmed ↗
- 4Methods of determination of biofilm formation by Candida albicans Res J Microbiol Janakiram B Myneni RB Kumar KA Gousia SK Latha JN 9096122017 https://scialert.net/abstract/?doi=jm.2017.90.96
- 5Molecular genetic approaches to identification, epidemiology and taxonomy of non-albicans Candida species J Med Microbiol Sullivan DJ Henman MC Moran GP O'Neill LC Bennett DE Shanley DB Coleman DC 399408441996863695610.1099/00222615-44-6-399 · doi ↗ · pubmed ↗
- 6Candidiasis and other emerging yeasts Curr Fungal Infect Rep Sharma M Chakrabarti A 15241720233674127110.1007/s 12281-023-00455-3PMC 9886541 · doi ↗ · pubmed ↗
- 7The emergence of non-albicans Candida species as causes of invasive candidiasis and candidemia Curr Infect Dis Rep Sobel JD 427433820061706463510.1007/s 11908-006-0016-6 · doi ↗ · pubmed ↗
- 8Non-albicans Candida infection: an emerging threat Interdiscip Perspect Infect Dis Deorukhkar SC Saini S Mathew S 615958201420142540494210.1155/2014/615958 PMC 4227454 · doi ↗ · pubmed ↗