A Simplified Three-Item Clinical Score to Identify Exertional Hypoxemia in Fibrotic Interstitial Lung Disease: A Real-World Cohort Study
Rogerio Rufino, Isabela Tamiozzo Serpa, Leonardo Palermo, Elizabeth Bessa, Bruno Rangel, Mariana Lopes, Agnaldo José Lopes, Mariana Costa Rufino, Cláudia Henrique da Costa, Anamelia Costa Faria

TL;DR
This study developed a simple 3-point clinical score to identify patients with lung disease at high risk of low oxygen levels during physical activity.
Contribution
A simplified 3-item clinical score with high sensitivity for predicting exertional hypoxemia in fibrotic ILD patients.
Findings
A score of ≥2 points identified high-risk patients with 100% sensitivity.
Risk of desaturation increased with score categories (17.1% for low risk, 95.1% for high risk).
The simplified score performed as well as complex models (AUC 0.82) but was easier to use.
Abstract
Background: Exertional oxygen desaturation (SpO2 ≤ 88%) during the six-minute walk test (6MWT) is a key prognostic marker in interstitial lung disease (ILD), yet access to the test is often limited in clinical practice. Developing simple, bedside tools to identify patients at risk may support early risk stratification and guide clinical decision-making. Methods: We conducted a retrospective, real-world cohort study in a tertiary referral center between January 2024 and July 2025, including 150 patients, of whom 67.33% (101 patients) were using supplemental oxygen. Clinical and physiological data collected within 30 days of the 6MWT were analyzed. The primary outcome was exertional hypoxemia, defined as peripheral oxygen saturation (SpO2) ≤ 88% at the end of the test. Four predictive approaches were evaluated: multivariable logistic regression, stepwise logistic regression, and a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
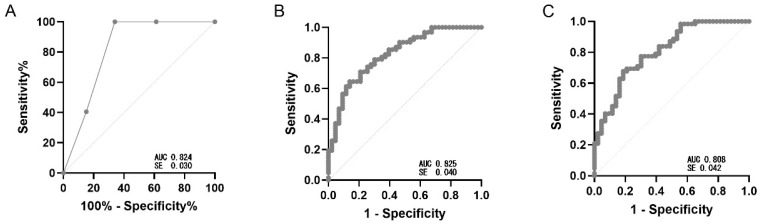 Figure 1
Figure 1- —FAPERJ
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Chronic Obstructive Pulmonary Disease (COPD) Research · Inflammatory Myopathies and Dermatomyositis
1. Introduction
Oxygen therapy is a cornerstone intervention in chronic lung diseases, classically indicated for patients with severe hypoxemia—defined as a partial pressure of arterial oxygen (PaO_2_) ≤ 55 mmHg or peripheral oxygen saturation (SpO_2_) ≤ 88% at rest—or for those with intermediate oxygen levels (PaO_2_ 55–59 mmHg) in the presence of cor pulmonale or polycythemia [1]. These indications stem from landmark clinical trials in the 1970s conducted in patients with chronic obstructive pulmonary disease (COPD), in which ≥ 15 h per day of long-term oxygen therapy (LTOT) significantly reduced mortality [2]. Since then, oxygen therapy has also been recommended based on the same criteria for interstitial lung diseases (ILDs), although the supporting evidence is less robust and often extrapolated from COPD populations [3].
Among ILDs, idiopathic pulmonary fibrosis (IPF) is the most frequent phenotype and carries the worst prognosis, with a median survival of only 2–3 years after diagnosis [4]. More recently, the concept of progressive pulmonary fibrosis (PPF) has been introduced to encompass heterogeneous ILD subtypes that share a similarly relentless clinical trajectory [5]. In this setting, hypoxemia may be absent at rest but frequently manifests during exertion. Desaturation during the 6 min walk test (6MWT) is a reproducible marker of poor prognosis and an independent predictor of mortality in fibrotic ILD, and it is a primary physiological criterion for prescribing oxygen [6,7]. Despite its widespread use, clinical trials have yielded mixed results: oxygen supplementation can improve dyspnea and exercise tolerance, yet consistent survival benefits remain elusive [1,8]. Current international guidelines recommend LTOT for severe resting hypoxemia and ambulatory oxygen for exertional desaturation, but these recommendations are based on low-certainty evidence [9,10].
Persistent logistical barriers further complicate optimal oxygen therapy decisions. Access to specialized centers remains limited in many regions, and standardized functional assessments, including the 6MWT and polysomnography, are not universally available [1,11]. Moreover, the need for trained personnel, appropriate facilities, and reproducible testing protocols often restricts the use of 6MWT to tertiary care settings. As a result, many patients with exertional hypoxemia may go unrecognized or remain undertreated [1,12].
Given these challenges, there is a clear clinical need for simple, pragmatic tools capable of identifying ILD patients at risk of exertional hypoxemia, particularly in environments where standardized exercise testing is unavailable [13]. In this study, we aimed to address this gap by developing and evaluating predictive approaches that integrate easily obtainable clinical information—notably the presence of cough—with routine pulmonary function measures (FVC and DLCO). Our objective was to assess whether a simplified clinical–functional score could accurately predict exertional hypoxemia, defined as SpO_2_ ≤ 88% at the end of the 6MWT, thereby informing day-to-day oxygen therapy decisions and improving patient triage.
2. Methods
2.1. Study Design
This was a retrospective, observational, real-world study based on electronic medical record review of patients with fibrotic interstitial lung disease followed at Piquet Carneiro University Polyclinic between January 2024 and July 2025. The protocol was approved by the Institutional Research Ethics Committee (CAAE: 80166424.3.0000.5259) and conducted in accordance with national and international ethical standards for human research (Supplementary Table S1).
2.2. Population and Inclusion Criteria
Patients with a confirmed diagnosis of idiopathic pulmonary fibrosis (IPF) or progressive pulmonary fibrosis (PPF), established according to the clinical, radiological, and physiological criteria in force at the time of care, were included in the study [5,14]. To ensure comparability across variables, only cases with ancillary tests performed within a maximum interval of 30 days were considered eligible. Patients with missing values for FVC, DLCO, or cough status were excluded (n = 12); their demographic and clinical characteristics were comparable to those of the analyzed cohort.
2.3. Sampling
The study was primarily designed to develop and internally validate a simple clinical–functional score for predicting exertional hypoxemia, rather than to detect small between-group differences. Based on conventional statistical assumptions (α = 0.05, β = 0.20, power = 80%) and a planned 2:1 allocation of home oxygen users to non-users, a total sample size of approximately 120–150 participants was considered sufficient to ensure an adequate number of events per variable for multivariable modeling, reliable estimation of classification metrics, and internal validation.
2.4. Data Sources
Data were extracted from electronic medical records and included:
- Clinical characteristics: age, sex, presence of cough, and smoking history;
- Physiological parameters: forced vital capacity (FVC% predicted) and diffusing capacity for carbon monoxide (DLCO% predicted);
- Oxygenation: peripheral oxygen saturation (SpO_2_) at rest and during exertion;
Pulmonary function tests (spirometry and DLCO) and the 6MWT were performed and interpreted in accordance with ATS/ERS consensus guidelines and standard operating procedures of the local laboratory [15,16,17]. Patients receiving long-term oxygen therapy performed the 6MWT while using their prescribed oxygen flow.
2.5. Outcome
Primary outcome. Exertional hypoxemia defined as SpO_2_ ≤ 88% at the end of the 6 min walk test (6MWT), performed and interpreted per ATS/ERS standards, with equipment maintenance/calibration per manufacturer and society recommendations and standardized corridor length/encouragement as specified by ATS/ERS guidance [17,18]. SpO_2_ values were recorded at test completion, as nadir measurements were not consistently documented in the medical records. Secondary outcomes. (i) Home oxygen use at the index visit (baseline characteristic), and (ii) exploratory resting hypoxemia (SpO_2_ ≤ 88% at rest), when available [1,19]. Secondary outcomes were not used to train or select the primary predictive models. All models were developed to discriminate the primary outcome.
Cough was considered present when patient-reported symptoms persisted continuously for ≥8 weeks [20].
2.6. Statistical Analysis
Discriminative analyses used SpO_2_ ≤ 88% during the 6 min walk test (6MWT) as the reference outcome for receiver operating characteristic (ROC) analysis, including area under the curve (AUC), sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV), all at the Youden-optimal threshold. Comparisons stratified by oxygen-use status were considered baseline descriptive analyses and were conducted separately, with patients categorized as home-oxygen users or non-users. Continuous variables were summarized as mean ± standard deviation (SD) or median [interquartile range, IQR], according to distribution. Normality was assessed using the Shapiro–Wilk test and homoscedasticity with Levene’s test. Between-group comparisons employed Student’s t test (or Welch’s t test when variances were unequal) under normality assumptions, and the Mann–Whitney U test otherwise. Categorical variables were reported as counts (percentages) and compared using Pearson’s χ^2^ test; when any expected cell frequency was <5, the Fisher exact test was applied. For multi-category comparisons (e.g., diagnostic groups), Cramér’s V was calculated as an effect-size measure. Confidence intervals for AUC were estimated using 1000 bootstrap replicates. All statistical tests were two-sided with α = 0.05. Analyses were performed in a validated statistical environment, and ROC analyses, descriptive statistics, and hypothesis tests were conducted using GraphPad Prism v10.6. Discriminative analyses for exertional hypoxemia used SpO_2_ ≤ 88% during the 6 min walk test (6MWT) as the reference standard [21]:
- Univariable ROC analyses (reference markers): ROC curves for FVC% predicted and DLCO% predicted were generated, reporting AUC and Youden-optimal cut-offs. Shapiro–Wilk results guided descriptive summaries (mean ± SD vs. median [IQR]);
- Multivariable logistic regression model: A conventional logistic model was constructed including FVC% predicted, DLCO% predicted, and cough as independent predictors. Regression coefficients (β) were estimated from the cohort data, and the linear predictor was used for discrimination and performance metrics.Equation—Logit(p) = β0 + β1·FVC + β2·DLCO + β3·Cough
- Stepwise logistic regression model: A stepwise selection procedure (bidirectional, based on Akaike information criterion) was applied to identify the most informative subset of predictors among the same candidate variables. Final model coefficients were derived from this data-driven selection.Equation—Logit(p) = β0 + β1·FVC + β2·DLCO
- Simplified clinical score (0–3): A point-based score was created by assigning 1 point each for FVC% predicted ≤ 61, DLCO% predicted ≤ 53, and presence of cough (total range 0–3 points). Cut-offs for FVC ≤ 61% and DLCO ≤ 53% were derived from the present cohort using Youden’s index from univariate ROC curves. This pragmatic scoring system was designed for bedside triage, with ≥2 points prespecified as the threshold for high risk.Equation—Score = (FVC ≤ 61) + (DLCO ≤ 53) + (Cough present)
3. Results
A total of 150 patients were included; 101 (67.3%) were on home oxygen at baseline and 49 (32.7%) were not. Sex distribution was comparable across groups, with no male predominance. Ethnicity was also similar (p = 0.799). Chronic cough was more frequent among oxygen users (77.2% vs. 55.1%; p = 0.006), and ever-smoker status was likewise more prevalent (58.4% vs. 30.6%; p = 0.001). Age was comparable (65.0 [56.0–72.0] years in oxygen users vs. 65.7 ± 11.5 years in non-users; p = 0.439) (Table 1).
In contrast, oxygen users showed more impaired lung function, with FVC 50.8 ± 14.9% vs. 66.1 ± 16.9% (p < 0.001) and DLCO 37.0 [25.0–52.0]% vs. 55.0 ± 18.7% (p < 0.001). The cut-off values for forced vital capacity (FVC ≤ 61%) and diffusing capacity of the lung for carbon monoxide (DLCO ≤ 53%) were derived from the present dataset, based on the Youden index obtained from receiver operating characteristic (ROC) curve analysis. Resting SpO_2_ was lower in the oxygen group (95.0 [92.8–97.0]%) than in non-users (97.0 [96.0–98.0]%; Mann–Whitney, p < 0.001). At the end of the 6 min walk test (6MWT), SpO_2_ also remained lower among oxygen users (84.0 [79.0–87.0]%) compared with non-users (92.1 ± 3.3%; Mann–Whitney, p < 0.001) (Table 1).
By diagnosis, in the oxygen group (n = 101) the distribution was HP (hypersensitivity pneumonitis) 32.7% (33/101), CTD-ILD (grouping SSc, RA, MCTD, IPAF) 39.6% (40/101), IPF 24.7% (25/101), and Other 3.0% (3/101); in the non-oxygen group (n = 49), CTD-ILD 49.0% (24/49), IPF 28.6% (14/49), HP 20.4% (10/49), and other 2.0% (1/49). The chi-square test showed no statistically significant difference between distributions (χ^2^(3) = 6.31; p = 0.097; Cramér’s V = 0.205), indicating a trend toward higher HP among oxygen users and more other diagnoses among non-users, without statistical significance.
Model performance for the primary outcome (SpO_2_ ≤ 88% during the 6 min walk test [6MWT]) is summarized as follows. Five predictive and statistical approaches were evaluated: univariable ROC analyses for FVC% predicted and DLCO% predicted, multivariable logistic regression, stepwise/best-subset logistic regression, an additive rule, and a simplified clinical–functional score (Table 2).
Discrimination was summarized by AUC with 95% CIs (bootstrap); sensitivity and specificity are reported with 95% CIs. Because PPV/NPV and accuracy vary with prevalence, values shown in Table 2 and Figure 1 reflect the study sample. Stepwise variable selection did not change the model composition, resulting in the same predictors (FVC% predicted, DLCO% predicted, cough) as the multivariable logistic regression. Therefore, only one logistic model is presented. Observed desaturation risk was 17.1% (0–1 points), 58.6% (2 points), and 95.1% (3 points), supporting a three-tier risk stratification (low, intermediate, high) to guide testing priorities (Table 3).
4. Discussion
This study presents consistent findings derived from a real-world clinical setting, using clinical and physiological information that is routinely available in the follow-up of patients with fibrotic interstitial lung disease (ILD). The methodological choice of restricting ancillary tests to a maximum interval of 30 days increased the uniformity of measurements and reduced bias related to temporal variation in disease status. In addition, selecting simple variables such as cough, FVC, and DLCO provided not only solid discriminatory performance but also high feasibility for clinical implementation. Clear inclusion criteria and the use of widely accepted statistical methods enhance the reproducibility of these results and strengthen their potential for external validation. The empirical thresholds (FVC ≤ 61% and DLCO ≤ 53%) correspond closely to ranges typically used to denote moderate-to-severe physiological impairment in ILD, supporting their face validity and potential generalizability.
FVC and DLCO remain fundamental parameters for the management and risk stratification of pulmonary fibrosis. A decline of absolute values ≥ 10% in FVC% predicted and ≥15% in DLCO% predicted is associated with poorer outcomes and reflects distinct dimensions of disease severity—volumetric and diffusing capacity impairment, respectively [22,23,24]. Their combined assessment improves prognostic accuracy, particularly in complex scenarios such as combined pulmonary fibrosis and emphysema [25]. In the present study, both parameters were key predictors of exertional desaturation during the 6MWT.
Chronic cough is highly prevalent in fibrotic ILD and is associated with poorer quality of life, higher morbidity, and increased mortality [26]. Incorporating this clinical variable into the predictive model improved its discriminative power, demonstrating that easily obtainable clinical information can meaningfully complement functional measurements for risk stratification.
The 6MWT remains the reference standard for evaluating exertional desaturation and guiding oxygen therapy in patients with ILD and is strongly endorsed by international guidelines [27]. However, its implementation requires strict standardization, appropriate staff training, and adequate physical space. Factors such as musculoskeletal pain, peripheral functional limitations, and variability in testing protocols can influence performance and reproducibility [17,28]. In this context, simple predictive tools become particularly relevant, as they allow initial screening in settings with limited resources or when performing a standard 6MWT is not feasible [29,30].
Recent studies have explored clinical-functional models to anticipate the occurrence of exertional hypoxemia. A previous study reported a C-index of 0.70 for predicting exertional hypoxemia by combining variables such as age, body mass index, diagnosis of idiopathic pulmonary fibrosis, FVC% predicted, and DLCO% predicted [31]. Other analyses demonstrated that most desaturation events occur within the first three minutes of the 6MWT, suggesting the feasibility of abbreviated protocols [32,33]. Our findings are consistent with this evidence, showing that a three-item score, using cough, FVC% predicted, and DLCO% predicted, with greater simplicity and strong potential for clinical implementation. Although discrimination was moderate rather than excellent, the simplicity and bedside feasibility of the score support its clinical adoption as a screening tool.
The proposed scoring system provides a practical framework for triaging patients according to their risk of exertional desaturation. Individuals scoring 0–1 points can be safely managed with routine follow-up, undergoing a 6MWT when available. Those with 2 points should be prioritized for comprehensive functional testing, while patients with 3 points warrant immediate evaluation with 6MWT and consideration of ambulatory oxygen therapy. This pragmatic approach may help clinicians optimize testing resources and identify high-risk individuals earlier, particularly in healthcare settings where access to exercise testing is limited.
Because the score was derived and internally tested within a single cohort, external validation in independent populations is essential before routine clinical adoption. We also acknowledge limitations related to the retrospective design, possible selection bias, and moderate sample size, as well as dependence on internally derived cut-offs. This study has limitations inherent to its retrospective, electronic medical record–based design, including potential selection and information biases, variability in clinical documentation, and incomplete standardization of testing procedures. The relatively modest sample size and the imbalanced distribution between groups (2:1) may limit precision and generalizability and influence prevalence-dependent metrics such as positive predictive value. Nevertheless, the use of widely available variables supports the reproducibility of the proposed score across diverse clinical settings.
Although exertional desaturation prediction has been explored previously, our study provides a minimalist, bedside tool that preserves accuracy (AUC 0.82), ensures maximal sensitivity for screening (cut-off > 2 points: sensitivity 100%), and relies on universally available variables, facilitating use in resource-limited settings.
In summary, our results reinforce the feasibility of using a simple clinical–functional score to identify patients with fibrotic ILD at higher risk of exertional hypoxemia. The combination of cough, FVC% predicted, and DLCO% predicted allows effective initial screening and can help prioritize more complex assessments such as the 6MWT. Owing to its simplicity, low cost, and robust discriminatory performance, the proposed tool can be easily incorporated into clinical workflows, particularly in resource-limited environments. Future studies should externally validate this simple score to confirm its utility across diverse ILD populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jacobs S.S. Krishnan J.A. Lederer D.J. Ghazipura M. Hossain T. Tan A.M. Carlin B. Drummond M.B. Ekström M. Garvey C. Home Oxygen Therapy for Adults with Chronic Lung Disease. An Official American Thoracic Society Clinical Practice Guideline Am. J. Respir. Crit. Care Med.2020202 e 121e 141Erratum in Am. J. Respir. Crit. Care Med. 2021, 203, 1045–104610.1164/rccm.202009-3608 ST 33185464 PMC 7667898 · doi ↗ · pubmed ↗
- 2Ahmadi Z. Sundh J. Bornefalk-Hermansson A. Ekström M. Long-Term Oxygen Therapy 24 vs 15 h/day and Mortality in Chronic Obstructive Pulmonary Disease P Lo S ONE 201611 e 016329310.1371/journal.pone.016329327649490 PMC 5029935 · doi ↗ · pubmed ↗
- 3Cordeiro R. Nunes A. Smith O. Renzoni E.A. Oxygen in interstitial lung diseases Breathe 20231922027110.1183/20734735.0271-202237378062 PMC 10292795 · doi ↗ · pubmed ↗
- 4Koudstaal T. Wijsenbeek M.S. Idiopathic pulmonary fibrosis La Presse Médicale 20235210416610.1016/j.lpm.2023.10416637156412 · doi ↗ · pubmed ↗
- 5Raghu G. Remy-Jardin M. Richeldi L. Thomson C.C. Inoue Y. Johkoh T. Kreuter M. Lynch D.A. Maher T.M. Martinez F.J. Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline Am. J. Respir. Crit. Care Med.2022205 e 18e 4710.1164/rccm.202202-0399 ST 35486072 PMC 9851481 · doi ↗ · pubmed ↗
- 6Bell E.C. Cox N.S. Goh N. Glaspole I. Westall G.P. Watson A. Holland A.E. Oxygen therapy for interstitial lung disease: A systematic review Eur. Respir. Rev.20172616008010.1183/16000617.0080-201628223395 PMC 9489021 · doi ↗ · pubmed ↗
- 7Clark K.P. Degenholtz H.B. Lindell K.O. Kass D.J. Supplemental Oxygen Therapy in Interstitial Lung Disease: A Narrative Review Ann. Am. Thorac. Soc.2023201541154910.1513/Annals ATS.202304-391CME 37590496 · doi ↗ · pubmed ↗
- 8Otake K. Misu S. Fujikawa T. Sakai H. Tomioka H. Exertional Desaturation Is More Severe in Idiopathic Pulmonary Fibrosis Than in Other Interstitial Lung Diseases Phys. Ther. Res.202326323710.1298/ptr.E 1021837181481 PMC 10169312 · doi ↗ · pubmed ↗