Accuracy of Emergency Physician-Performed Echocardiography for Diastolic Dysfunction in Suspected Acute Heart Failure: A Systematic Review and Meta-Analysis
Shao-Min Huang, Yu-Hsuan Yeh, Cheuk-Kwan Sun, Hsuan-Wei Chu

TL;DR
Emergency physicians can accurately rule out heart failure using ultrasound, but it's less reliable for confirming the condition.
Contribution
This study provides a meta-analysis on the diagnostic accuracy of emergency physician-performed echocardiography for diastolic dysfunction.
Findings
EP-performed FCU showed excellent sensitivity (94%) for ruling out diastolic dysfunction.
Specificity was moderate (59%), limiting its use for confirming the diagnosis.
Three of four studies had a high risk of bias, suggesting potential limitations in the findings.
Abstract
Background: This study compared the accuracy of diagnosing left ventricular diastolic dysfunction (DD) between emergency physician (EP)-performed focused cardiac ultrasound (FCU) and cardiologist-interpreted reference standards in adult patients presenting to the emergency department (ED) with suspected acute heart failure (HF). Methods: PubMed, Embase, and the Cochrane Central Register of Controlled Trials were systematically searched for studies focusing on adult ED patients with symptoms of acute HF that compared the accuracy of DD diagnosis between EP-performed FCU and reference standards including cardiologist-reviewed FCU clips, formal transthoracic echocardiography, or invasive hemodynamics without language/date restrictions. Results: Meta-analysis of four eligible observational studies (327 patients enrolled; 298 analyzed) demonstrate excellent sensitivity of EP-performed FCU…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
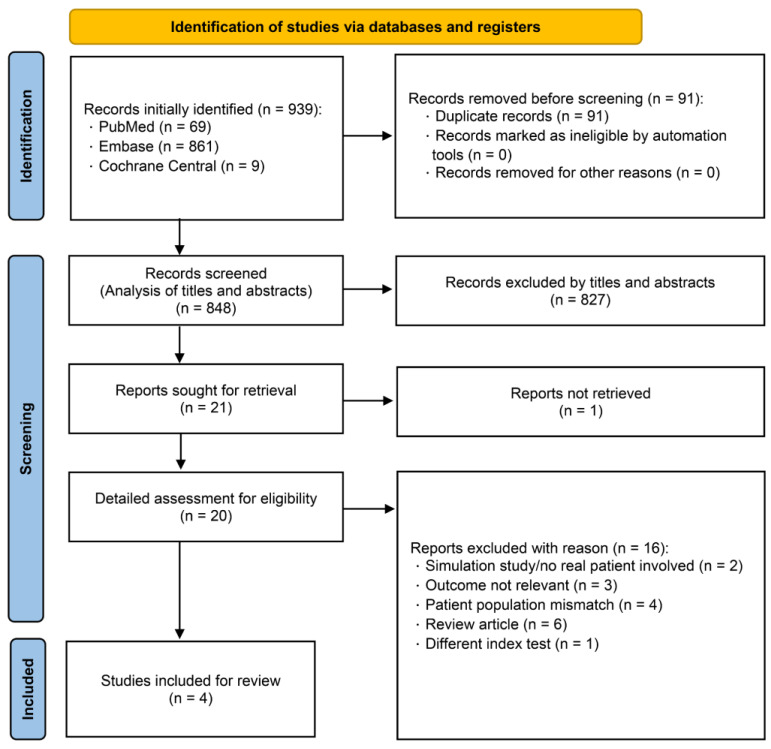 Figure 1
Figure 1 Figure 2
Figure 2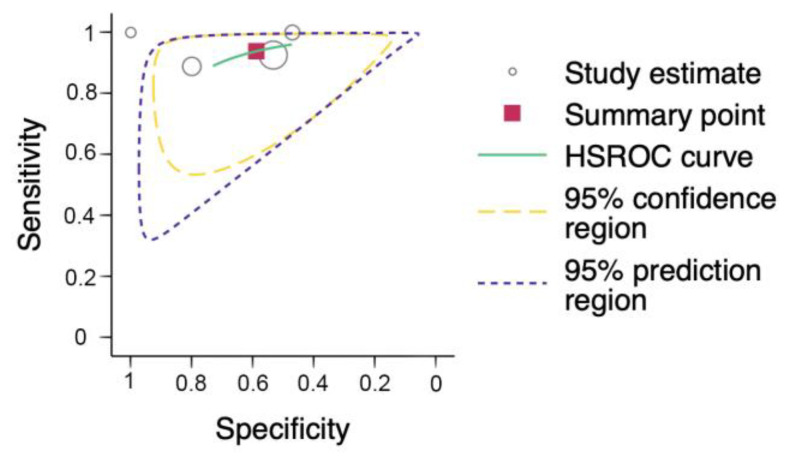 Figure 3
Figure 3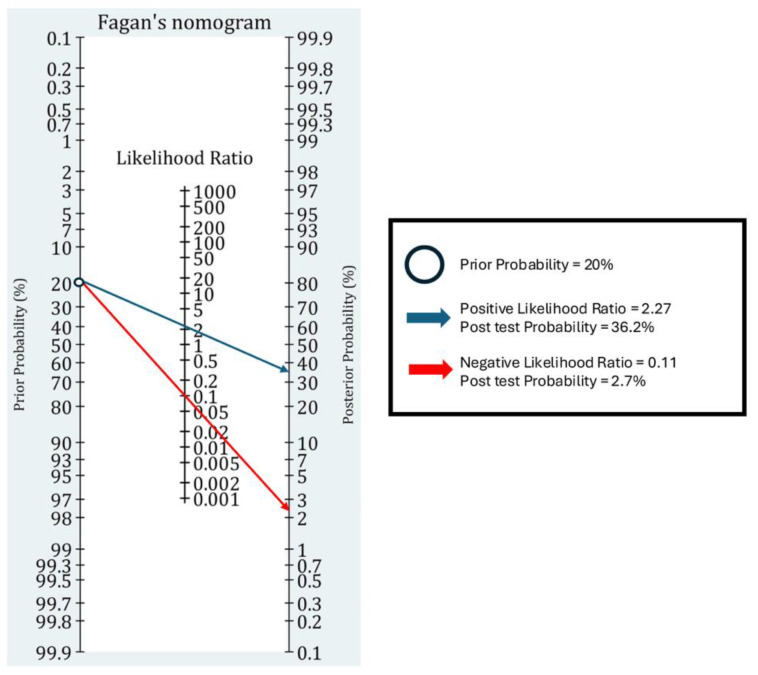 Figure 4
Figure 4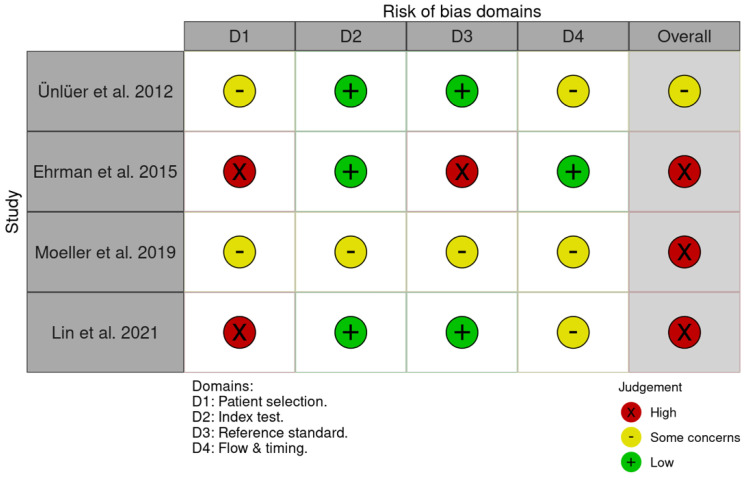 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Cardiovascular Function and Risk Factors · Heart Failure Treatment and Management
1. Introduction
Left ventricular diastolic dysfunction is a critical contributor to acute heart failure regardless of ejection fraction (EF) [1]. Diastolic dysfunction involves increased stiffness of the left ventricle with compensatory elevation in filling pressures and a reduced stroke volume, thereby triggering heart failure symptoms particularly during exertion even when the EF is preserved [2,3,4,5,6]. Heart failure with preserved EF (HFpEF), which involves elevated left-ventricular filling pressures, comprises approximately half of all heart failure population [7]. Notably, one in six patients over 65 with unexplained exertional dyspnea has unrecognized heart failure, mostly HFpEF, underscoring diastolic dysfunction-driven HFpEF as a frequent yet underdiagnosed cause of acute breathlessness [8,9].
Despite being the reference-standard modality for assessing diastolic function, formal TTE (trans-thoracic echocardiography) is seldom immediately available as a point-of-care diagnostic tool in the emergency department (ED). To bridge the diagnostic gap, emergency physicians increasingly utilize focused cardiac ultrasound, incorporating simplified Doppler indices and supportive markers such as left atrial size for prompt evaluation of diastolic function [10,11,12,13,14].
However, assessing diastolic dysfunction via focused cardiac ultrasound (FCU) in the ED remains technically challenging. Major international guidelines caution against relying solely on FCU for diastolic evaluation. Consensus statements from the American Society of Echocardiography/American College of Emergency Physicians (ASE/ACEP, 2010) and the European Society of Cardiology’s Acute Cardiac Care group (ESC/EACVI, 2013) uniformly recommend formal TTE over FCU without advanced training for accurate diastolic assessment [15,16]. On the other hand, with accumulating studies aiming at validating emergency physician-performed diastolic function assessment against formal TTE [10,11,12], the 2023 Advanced Emergency Medicine Ultrasonography (AEMUS) Core Content revision, led by the American Board of Emergency Medicine (ABEM), explicitly lists diastolic function assessment as a core advanced cardiac ultrasound competency [17]. Several single-center ED studies have explored the reliability of adopting simplified FCU approaches for assessing diastolic dysfunction in patients with suspected acute heart failure and reported promising diagnostic performance [10,11,12,13,14]. Nevertheless, to date, the results of those studies remain disparate, possibly attributable to a lack of formal synthesis and a standardized diagnostic pathway.
Therefore, this meta-analysis compared the reliability and clinical applicability of emergency physician-performed focused cardiac ultrasound (EP-FCU) with cardiologist-interpreted reference standards in identifying diastolic dysfunction regardless of the ejection fraction.
In accordance with the PIT format (i.e., Population/Index test/Target condition) based on the Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy (Cochrane DTA) [18], the current systematic review aimed at updating the current evidence regarding the diagnostic accuracy of EP-FCU (Index test) among adults presenting to the emergency department with symptoms suggestive of acute heart failure (Population) compared with that of formal TTE, cardiologist-reviewed ultrasound clips, or invasive hemodynamic measurements that served as reference tests for identifying the presence of left ventricular diastolic dysfunction (Target Condition).
2. Materials and Methods
The current meta-analysis and systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses of Diagnostic Test Accuracy (PRISMA-DTA) guidelines (Supplementary Files S1 and S2) [19] and adhered to the methodological recommendations outlined in the Cochrane Handbook for Diagnostic Test Accuracy Reviews [18] for study selection, review, and evidence synthesis. This study was prospectively registered with PROSPERO (registration ID: CRD420251046794).
2.1. Source and Search Strategy
Two independent reviewers (SMH and YHY) systematically searched electronic databases including PubMed (1946–present), Embase (Elsevier, 1947–present), and the Cochrane Central Register of Controlled Trials (CENTRAL) on 6 May 2025. No restrictions regarding language, publication date, or study type were imposed. Potentially eligible articles were identified by combining controlled vocabulary (MeSH/Emtree) and free-text terms for the index test (i.e., “focused cardiac ultrasound”, “point-of-care ultrasound”, “tissue Doppler”, “E/e′”), the target condition (i.e., “diastolic dysfunction”, “heart failure with preserved ejection fraction”), and the emergency care setting/personnel (i.e., “emergency department”, “emergency physician”) using Boolean operators and database-specific syntax. Reference lists of identified studies and relevant review articles were manually screened to identify additional eligible studies. The detailed search strategies and full list of search terms are provided in Supplementary File S3.
2.2. Eligibility Criteria and Study Selection
Studies were eligible for inclusion if they recruited adult patients (≥18 years) presenting to the emergency department with acute dyspnea or other clinical symptoms suggestive of acute heart failure. The index test of interest was EP-FCU, utilizing any view or Doppler parameter specifically for assessing diastolic function. Acceptable reference standards included either (a) FCU clips reviewed by a cardiologist or accredited sonographer, (b) formal TTE, or (c) invasive hemodynamic assessment performed during the same clinical encounter.
We considered prospective or retrospective observational diagnostic accuracy studies without language or publication date restrictions. Conference abstracts were eligible if they reported adequate data to construct a 2 × 2 contingency table. Studies enrolling fewer than 20 participants were excluded. All retrieved publications from electronic database searches were imported into EndNote 21 (Clarivate, Denver, CO, USA) for Mac to remove duplicates. The remaining records were then exported into the web-based software Rayyan (web-based application without public version) [20] for the initial title and abstract screening.
2.3. Screening and Assessment of Studies
The same two independent reviewers (SMH and YHY) screened the retrieved records based on titles and abstracts and subsequently reviewed full-text articles against predefined inclusion criteria. Disagreements were resolved through discussion with a third reviewer (HWC) till a consensus was reached. During the initial screening phase, clearly irrelevant records were excluded based on predetermined exclusion criteria. Full-text articles for studies that passed initial screening were then retrieved and rigorously assessed for eligibility against the predefined inclusion and exclusion criteria. In addition, the reference lists of the included articles were manually examined to identify any potentially relevant studies not captured by the original database searches. Reasons for exclusion of individual studies are documented in Supplementary File S4.
2.4. Data Extraction
Essential data from eligible papers were independently extracted by the same two reviewers (SMH and YHY) to a bespoke data extraction form that included information regarding study characteristics (e.g., author, year of publication, country) and study details (e.g., sample size, patient demographics, index-test protocol, reference-standard criteria). Primary outcomes included pooled sensitivity and specificity, while secondary outcomes comprised positive likelihood ratio (PLR) and negative likelihood ratio (NLR).
We dichotomized diastolic dysfunction as positive for any grade (I–III) and negative for normal findings. When a study reported an indeterminate/uninterpretable category for either the index test (EP-FCU) or the reference standard, we excluded such cases from 2 × 2 extraction while recording the per-study counts. This rule was applied consistently across studies.
2.5. Risk of Bias Assessment
The same two independent reviewers (SMH and YHY) assessed the risk of bias for the included studies using the Quality Assessment of Diagnostic Accuracy Studies—2 (QUADAS-2) tool [21], specifically tailored to this systematic review. Reviewers were blinded to each other’s ratings during this process.
The QUADAS-2 tool evaluates four primary domains relevant to diagnostic accuracy studies: patient selection, index test (emergency physician-performed assessment of diastolic dysfunction), reference standard (stored FCU clips reviewed by a cardiologist or accredited sonographer, formal TTE, or invasive hemodynamic measurement), and the flow and timing of the study processes. Each domain was categorized as having a low, high, or unclear risk of bias. A summary plot illustrating the overall assessment of risk of bias across included studies was generated using the Robvis visualization tool (Shiny web app; no public version) [22].
2.6. Statistical Analysis and Data Synthesis
Indeterminate (or “uninterpretable”) results were defined a priori as initially enrolled participants in whom either the index test (EP-performed focused cardiac ultrasound, EP-FCU) or the reference standard could not yield a definitive classification of diastolic function. We constructed study-level 2 × 2 tables using a complete-case rule: Only participants with a conclusive “positive” (the presence of DD regardless of grading) or “negative” (normal) classification on both the index test and the reference standard contributed to the primary meta-analysis, while those labelled indeterminate by either test were excluded from the 2 × 2 tables. The numbers of patients with definitive classifications and those who were excluded due to indeterminate results were recorded and reported.
All statistical analyses were conducted using Stata 18 with the metandi command. A bivariate random-effects model was adopted to derive pooled estimates of sensitivity and specificity, along with corresponding 95% confidence intervals (CIs), presented via coupled forest plots. Moreover, we generated a hierarchical summary receiver-operating characteristic (HSROC) curve and summary point to assess the overall diagnostic performance [23].
We prespecified sensitivity analysis using Meta-DiSc 2.0 [24] that excluded the small, high-risk-of-bias studies and reported pooled sensitivity, specificity, PLR, and NLR for the sensitivity analysis.
3. Results
3.1. Search Results
Of a total of 939 studies initially retrieved through our systematic search, 20 deemed potentially eligible following title and abstract screening were subjected to a full-text review. Eventually, four prospective observational studies met all predefined inclusion criteria. The detailed selection process is depicted in Figure 1. Of the 327 patients initially enrolled in the four eligible studies, 298 eventually contributed to our pooled analysis after excluding those with indeterminate classifications. In detail, 69 patients were included with no indeterminate case in the study by Ünlüer et al. [10], 44 were recruited after excluding 18 indeterminate cases from 62 patients initially enrolled in the study by Ehrman et al. [11], 20 were included with no indeterminate case in the study by Moeller et al. [25], and 165 were enrolled following the exclusion of 11 indeterminate cases from 176 patients initially recruited in the study by Lin et al. [12].
3.2. Description of Included Studies
The characteristics of the four eligible studies are shown in Table 1, while the diagnostic performance of EP-FCU for diastolic dysfunction is summarized in Table 2. The forest plot of the four studies, compiled using Review Manager 5.4.1 [26], is displayed in Figure 2. A comprehensive list of all excluded studies with specific reasons for their exclusion is available in Supplementary File S4.
In the prospective observational study by Ünlüer et al. (2012) [10], three attending emergency physicians received a brief diastology training course (i.e., three-hour didactic session and three-hour hands-on practice) before performing limited bedside FCU on 69 dyspneic adults (mean age 63 ± 9 years; all EF ≥ 50%). They assessed basic trans-mitral Doppler indices (E/A ratio, deceleration time, isovolumic relaxation time), which were subsequently compared with those acquired with formal TTE performed by a cardiologist within two hours using tissue Doppler-based diagnosis. Stringent exclusion criteria of that study (age < 40 years, pregnancy, acute coronary syndrome, atrial fibrillation, significant valvular disease, or tachycardia) may have optimized imaging conditions, potentially enhancing diagnostic accuracy. That study demonstrated a sensitivity of 89% (95% CI, 77 to 96%) and specificity of 80% (95% CI, 52 to 96%) of EP-FCU, suggesting reasonable diagnostic utility.
In the study conducted by Ehrman et al. (2015) [11], two ultrasound fellowship-trained emergency physicians underwent identical diastology training (i.e., three-hour didactic plus three-hour hands-on) and performed FCU on 62 adults (mean age 56 ± 14 years; 48% male) presenting with undifferentiated dyspnea. They employed both trans-mitral Doppler (E/A ratio) and tissue Doppler parameters (i.e., septal & lateral e′, E/e′), according to simplified 2009 American Society of Echocardiography (ASE) criteria. The reference standard was a blinded cardiologist’s reinterpretation of emergency physician acquired images. Diagnostic performance indicated high sensitivity (100%, 95% CI: 87 to 100%) but limited specificity (47%, 95% CI: 23 to 72%), reflecting notable limitations in positive predictive utility.
In the small-sample study by Moeller et al. (2019) [25], FCU was performed by an ultrasound fellowship-trained emergency physician using pulse-wave and tissue Doppler measurements with the findings compared to formal sonography interpreted by a blinded cardiologist. Among the 20 patients evaluated, the emergency physician correctly identified 19 patients as positive for diastolic dysfunction and one patient as negative based on the cardiologist’s assessment. This resulted in high sensitivity (i.e., 100%, 95% CI: 82 to 100%) and high specificity (i.e., 100%, 95% CI: 3 to 100%).
Lin et al. (2021) [12] further expanded these findings in a study involving twelve ultrasound-fellowship-trained emergency physicians, who completed a comparable diastology training program (i.e., two-hour didactic plus two-hour hands-on). They performed a comprehensive FCU evaluation (including E/A ratio, septal e′, lateral e′, E/e′, and left atrial size) on 176 patients (mean age 64 ± 14 years; 65% male; 63% EF < 50%) presenting with dyspnea, syncope, or chest pain. Their scans were validated against same-day cardiologist-performed TTE using a modified 2016 ASE diastolic algorithm with a septal e′ cutoff set at <8 cm/s and an average interval of approximately four hours between scans. EP-FCU exhibited high sensitivity (93%, 95% CI: 87 to 96%) but moderate specificity (53%, 95% CI: 34 to 72%), highlighting similar diagnostic characteristics to those reported by Ehrman et al.
3.3. Overall Diagnostic Values of EP-FCU for Diastolic Dysfunction
Across all four studies, EP-FCU demonstrated high sensitivity (89 to 100%) and an excellent NLR (0 to 0.14) but moderate specificity (47 to 100%) and a modest PLR (1.89 to 4.44) for diastolic dysfunction.
After meta analysis by Stata 18 metandi command [22], the sensitivity of EP-FCU to diagnose diastolic dysfunction was 94% (95% CI: 87 to 97%) and the specificity was 59% (95% CI: 42 to 74%), with a summary PLR of 2.27 (95% CI: 1.55 to 3.33) and a summary NLR of 0.11 (95% CI: 0.05 to 0.21), supporting EP-FCU as a rule-out tool based on the results of cardiologist-performed TTE (Figure 3 and Table 3).
We performed a sensitivity analysis excluding the small—sample study by Moeller et al. (2019; n = 20) [25] using Meta-DiSc 2.0 [24]. The pooled estimates were sensitivity 93% (95% CI: 87% to 96%), specificity 59% (95% CI: 42% to 75%) and PLR 2.27 (95% CI: 1.36 to 3.18), NLR 0.12 (95% CI: 0.05 to 0.19). Absolute differences were 1 percentage point for sensitivity and 0.01 for NLR, with broadly overlapping CIs, indicating robustness of our pooled estimates after exclusion of that study [25].
3.4. Clinical Utility of EP-FCU to Diagnose Diastolic Dysfunction
The clinical utility of EP-FCU was evaluated using a scenario-based approach. We assumed pre-test probabilities of 10%, 20%, and 30% to reflect plausible ranges in the ED populations. Post-test probabilities for positive and negative EP-FCU were derived from the meta-analytic positive and negative likelihood ratios using odds-based Bayes equations. The 20% scenario was displayed in a Fagan nomogram for demonstration (Figure 4) with all scenarios being summarized numerically in Table 4.
Using the summary estimates (PLR = 2.27; NLR = 0.11) in the main analysis, the post-test probabilities after a positive EP-FCU result were 20.1%, 36.2%, and 49.3% for pre-test probabilities of 10%, 20%, and 30%, respectively; after a negative result, they were 1.2%, 2.7%, and 4.5%, respectively (Table 4).
For decision-making, we used a 2% rule—out threshold for ED safety considerations as previously described [27]. Based on our calculated NLR of 0.11, the maximal pre-test probability to achieve a 2% rule-out threshold after a negative result was 16%; only the 10% scenario met this threshold. These estimates support a triage role for EP-FCU in ruling out DD in lower-prevalence settings. In contrast, in higher pre-test contexts, our results indicated the need for additional diagnostic parameters (e.g., natriuretic peptides) to rule out the diagnosis. Our findings also showed that positive EP-FCU results increased the post-test probability of DD to 20–49% across different scenarios (Table 4), which is insufficient for ruling in DD and would warrant confirmatory testing (e.g., formal TTE).
3.5. Assessment of Methodological Quality
The QUADAS-2 tool was used to assess the risk of bias across the four studies, with the results presented in a traffic-light plot generated by the Robvis tool [22] (Figure 5).
In the patient-selection domain, the studies by Ehrman et al. (2015) [11] and Lin et al. (2021) [12] were rated as having a high risk due to convenience sampling. In the reference-standard domain, the study by Ehrman et al. (2015) [11] presented a risk of incorporation bias, as the cardiologist-reviewed emergency physician-acquired echo clips were directly used to classify diastolic function. This approach may lead to incorporation and misclassification biases, particularly if scanning techniques were suboptimal or key measurements [e.g., left atrial volume and peak tricuspid regurgitation (TR) velocity] routinely included in formal TTE were omitted. In flow-and-timing domain, the studies by Ünlüer et al. (2012) [10] and Lin et al. (2021) [12] were judged to present with an unclear risk because the interval between EP-FCU and formal TTE varied from less than two hours to up to eight hours, during which patient hemodynamics might change, posing a risk of misclassification bias. Currently, no consensus exists regarding the optimal interval between these imaging assessments within which the hemodynamic fluctuation is minimal to ensure optimal data comparison. Finally, Moeller et al. (2019) [25] provided insufficient data to answer signaling questions across all four domains; thus, the risk of bias for all four domains was unclear, resulting in an overall high risk of bias for their study.
4. Discussion
4.1. Key Findings
To the best of our knowledge, the current study is the first systematic review and meta-analysis to evaluate EP-FCU accuracy in identifying diastolic dysfunction in patients with suspected acute heart failure. Our analysis demonstrated that EP-FCU achieved high sensitivity (94%, 95% CI: 87 to 97%) and a low NLR (0.11, 95% CI: 0.05 to 0.21) but moderate specificity (59%, 95% CI: 42 to 74%) and a modest PLR (2.27, 95% CI: 1.55 to 3.33), supporting greater utility in ruling out rather than ruling in diastolic dysfunction in patients with suspected acute heart failure.
In scenario-based clinical-utility analyses (pre-test 10%/20%/30%), a negative EP-FCU reduced post-test risk to 1.2%, 2.7%, and 4.5%, respectively; under a 2% rule-out threshold relevant to ED practice, this supports a triage role for rule out DD primarily in lower-prevalence settings (≤16% pre-test). Accordingly, because at higher pre-test probabilities (~20–30%) even a negative EP-FCU leaves post-test risks >2% (~2.7–4.5%) and a positive EP-FCU alone yields only ~20–49%—insufficient to rule-in—formal TTE (and/or a structured diagnostic pathway) is recommended when pre-test risk exceeds 16% or when EP-FCU is positive/indeterminate or image quality is limited.
4.2. Integration with International Guidelines
The findings of this review are notably relevant in clinical practice, as they highlight an evolving tension between current consensus-driven clinical recommendations and recent shifts in training paradigms within emergency medicine. On the one hand, foundational consensus statements from the ASE/ACEP (2010) [15] and ESC/EACVI (2013) [16] have traditionally emphasized the inappropriateness of using FCU without comprehensive training for a definitive assessment of diastolic function. On the other hand, the recent 2023 AEMUS Core Content revision explicitly lists diastolic function assessment as a core competency [17], signaling a significant shift in training expectations.
Our systematic review may provide useful evidence to navigate this transitional period. In contrast with the cautious stance of earlier guidelines that denied the reliability of EP-FCU as a diagnostic modality for diastolic dysfunction [15,16], the excellent sensitivity (94%) and low NLR (0.11) identified in the current study supported its use as a triage tool for ruling out this condition. Our findings are in line with the recommendation of the recent AEMUS guidelines that included ultrasound skills in the core training program for emergency physicians [17]. Nevertheless, the moderate specificity (59%) and modest PLR (2.27) rendered it inappropriate as a standalone tool for ruling in the diagnosis. In this way, our work may help bridge the gap between these perspectives by defining both the current utility and the clear limitations of EP-FCU.
4.3. Limitations
Consistent with GRADE for test accuracy [18,28], we summarize limitations across four domains—external validity (applicability), internal validity (risk of bias), inconsistency (heterogeneity), and imprecision—and then add a brief note on natriuretic peptides for clinical context.
External validity (applicability) of our study result for routine ED practice may be limited by operator expertise. Therefore, the involvement of fellowship-trained physicians in three of the four included studies [11,12,25] may not reflect the average ED setting. Applicability is also constrained by the participant spectrum. Two studies (Ünlüer et al. [10], Lin et al. [12]) excluding common comorbidities such as atrial fibrillation, significant valvular disease, or tachycardia—conditions frequently encountered in undifferentiated ED presentations—so generalizability to real world ED populations may be limited.
The internal validity of the included studies may be threatened by several risks of bias, which was evaluated by QUADAS-2. In the patient selection domain, the studies by Ehrman et al. (2015) [11] and Lin et al. (2021) [12] use convenience sampling rather than consecutive/random sampling, which “may produce estimates of test accuracy that do not reflect the performance of the test in clinical practice”. Two studies (Ünlüer et al. [10], Lin et al. [12]) also excluded common comorbidities (atrial fibrillation, significant valvular disease, tachycardia), risking patient-selection (spectrum) bias—in addition to the applicability concerns noted above. Also the recruitment of patients with both preserved and reduced ejection fraction in the studies by Ehrman et al. [11] and Lin et al. [12] may have contributed spectrum bias, as diastolic parameters such as E/A ratio and E/e′ behave differently across the EF spectrum. Reference standard-related bias was present in three out of the four studies. In the study by Ehrman et al., cardiologists reinterpreted the images acquired by emergency physicians, thereby introducing incorporation bias and misclassification bias. In addition, the timing between EP-FCU and formal TTE varied significantly; it was less than two hours in Ünlüer et al. [10], but up to eight hours in that by Lin et al. [12]. Such time gaps could allow for changes in hemodynamic status, potentially leading to misclassification bias.
The inconsistency (heterogeneity) in our findings may be explained by the wide variation in index test protocol across our included studies, in which EP-FCU did not represent a single uniform index test but rather a spectrum different protocols—from transmitral inflow only (Ünlüer) [10] to protocols incorporating TDI and left atrial size (Ehrman [11]; Lin [12]). Such a discrepancy in protocols implied the utilization of different positivity thresholds, thereby producing a threshold effect—movement along the ROC curve with higher sensitivity at the expense of specificity, and vice versa. This phenomenon is visible in the coupled forest plots (Figure 2). Specifically, setting aside the small-sample-size study by Moeller et al. [25], the other studies formed a V-shaped arrangement consistent with the presence of a threshold effect. The wide variation in EP-FCU index test protocols across our included studies may be a significant limitation of our study outcome. Further large-scale clinical investigations focusing on specific protocols are warranted to verify our findings.
Imprecision of our study outcomes was also notable. The inclusion of only four studies (327 enrolled; 298 analyzed) in our meta-analysis contributed to a wide confidence region of the summary sensitivity and specificity.
Lastly, all four studies based their diagnosis of DD only on echocardiography. On the other hand, although a number of heart failure diagnostic guidelines recommend incorporating natriuretic peptides (BNP/NT-proBNP) into the diagnostic pathways [2,4,5,6], prior studies indicated that up to about 30% of patients with HFpEF may have normal BNP values despite the presence of symptoms, echocardiographic abnormalities, and evidence derived from invasive hemodynamic procedures (e.g., elevated filling pressures) [5,29,30].
4.4. Future Research Directions
Our findings, which suggested the applicability of EP-FCU as a rule out triage tool for undifferentiated dyspnea in low prevalence ED settings, warranted validation from further large-scale studies that should enroll average emergency physicians without ultrasound fellowship training to better reflect the real-world ED scenario. Moreover, instead of convenience sampling of ED patients adopted in two of our included studies [11,12], consecutive or randomized sampling may help in minimizing potential sampling bias [18]. In addition, common comorbidities such as atrial fibrillation, significant valvular disease, and tachycardia may not be routinely excluded to avoid spectrum bias [18]. Furthermore, the observed protocol variation indicates that future EP-FCU should emphasize the utilization of a fixed positivity threshold (e.g., ASE guidelines-aligned) coupled with the adoption of a standardized protocol (e.g., measurement parameters, interval between EP-FCU and formal TTE) as well as the implementation of a standardized EP-FCU training program and imaging quality control measures to minimize heterogeneity through reducing the threshold effect and decreasing equipment and operator variability. Finally, the development and validation of artificial intelligence (AI)-assisted quantification tools with a strong emphasis on applicability in the evaluation of cardiac function in an emergency medical setting may further broaden the horizon in this area [31].
5. Conclusions
To our best knowledge, this is the first systematic review and meta-analysis to evaluate the diagnostic accuracy of EP-FCU for assessing diastolic dysfunction in patients with suspected acute heart failure. Our findings demonstrated that while EP-FCU showed excellent sensitivity (94%, 95% CI: 87 to 97%) and a low NLR (0.11, 95% CI: 0.05 to 0.21) that supported its use as an effective tool to rule out diastolic dysfunction, its moderate specificity (59%, 95% CI: 42 to 74%) and limited PLR (2.27, 95% CI: 1.55 to 3.33) precluded its standalone use as a definitive diagnostic modality. Our results highlighted the viability of EP-FCU as an effective initial point-of-care triage tool in the differential diagnosis of patients presenting with acute dyspnea based on comparison with formal TTE that still serves as the standard for definitive diagnosis as recommended by the ASE/ACEP (2010) and ESC/EACVI (2013) guidelines [15,16].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pfeffer M.A. Shah A.M. Borlaug B.A. Heart Failure with Preserved Ejection Fraction in Perspective Circ. Res.20191241598161710.1161/CIRCRESAHA.119.31357231120821 PMC 6534165 · doi ↗ · pubmed ↗
- 2Pieske B. Tschope C. de Boer R.A. Fraser A.G. Anker S.D. Donal E. Edelmann F. Fu M. Guazzi M. Lam C.S.P. How to diagnose heart failure with preserved ejection fraction: The HFA-PEFF diagnostic algorithm: A consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC)Eur. Heart J.2019403297331710.1093/eurheartj/ehz 64131504452 · doi ↗ · pubmed ↗
- 3Heidenreich P.A. Bozkurt B. Aguilar D. Allen L.A. Byun J.J. Colvin M.M. Deswal A. Drazner M.H. Dunlay S.M. Evers L.R. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation 2022145 e 895e 103210.1161/CIR.000000000000106335363499 · doi ↗ · pubmed ↗
- 4Mc Donagh T.A. Metra M. Adamo M. Gardner R.S. Baumbach A. Bohm M. Burri H. Butler J. ČelutkienėJ. Chioncel O. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure Eur. Heart J.20214235993726 Erratum in Eur. Heart J. 2021, 42, 490110.1093/eurheartj/ehab 36834447992 · doi ↗ · pubmed ↗
- 5Nagueh S.F. Sanborn D.Y. Oh J.K. Anderson B. Billick K. Derumeaux G. Klein A. Koulogiannis K. Mitchell C. Shah A. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography and for Heart Failure with Preserved Ejection Fraction Diagnosis: An Update from the American Society of Echocardiography J. Am. Soc. Echocardiogr.20253853756910.1016/j.echo.2025.03.01140617625 · doi ↗ · pubmed ↗
- 6Nagueh S.F. Smiseth O.A. Appleton C.P. Byrd B.F.3rd Dokainish H. Edvardsen T. Flachskampf F.A. Gillebert T.C. Klein A.L. Lancellotti P. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging J. Am. Soc. Echocardiogr.20162927731410.1016/j.echo.2016.01.01127037982 · doi ↗ · pubmed ↗
- 7Omote K. Verbrugge F.H. Borlaug B.A. Heart Failure with Preserved Ejection Fraction: Mechanisms and Treatment Strategies Annu. Rev. Med.20227332133710.1146/annurev-med-042220-02274534379445 PMC 9002335 · doi ↗ · pubmed ↗
- 8van Riet E.E. Hoes A.W. Limburg A. Landman M.A. van der Hoeven H. Rutten F.H. Prevalence of unrecognized heart failure in older persons with shortness of breath on exertion Eur. J. Heart Fail.20141677277710.1002/ejhf.11024863953 · doi ↗ · pubmed ↗