Emergency Surgical Management of Chemotherapy-Induced Tumor Rupture in a Patient with MYCN-Amplified Neuroblastoma: A Case Report
Katsuhiro Ogawa, Satoshi Makita, Ami Utsunomiya, Hajime Asai, Hiroki Ishii, Daiki Kato, Yoichi Nakagawa, Kaito Hayashi, Shunya Takada, Aitaro Takimoto, Akihiro Yasui, Masamune Okamoto, Takahisa Tainaka, Chiyoe Shirota, Hiroo Uchida

TL;DR
A 4-year-old girl with high-risk MYCN-amplified neuroblastoma required emergency surgery after her tumor ruptured following chemotherapy, highlighting the importance of early surgical readiness in such cases.
Contribution
This case report highlights the critical role of prompt surgical intervention in managing chemotherapy-induced tumor rupture in high-risk MYCN-amplified neuroblastoma.
Findings
Emergency laparotomy and tumor resection were life-saving in a patient with ruptured MYCN-amplified neuroblastoma.
Embolization alone may not prevent abdominal compartment syndrome in such cases.
Multimodal therapy following surgery led to 2 years of remission.
Abstract
Tumor rupture with neuroblastoma is an uncommon but serious complication, particularly in high-risk cases involving MYCN amplification. When rupture occurs soon after induction chemotherapy is initiated, rapid deterioration and abdominal compartment syndrome (ACS) may develop. Early identification of high-risk patients and their readiness for surgical management are essential to optimizing outcomes. A 4-year-old girl presented with a large left adrenal mass and elevated neuroblastoma markers. Imaging showed a heterogeneous 11 × 9.5 × 17-cm tumor encasing the renal hilum. Because of intratumoral hemorrhage, biopsy was deferred and induction chemotherapy was initiated. Seven days later, sudden abdominal distension and severe anemia developed. Contrast-enhanced CT confirmed intraperitoneal bleeding from the ruptured tumor. Transarterial embolization, including occlusion of the left renal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
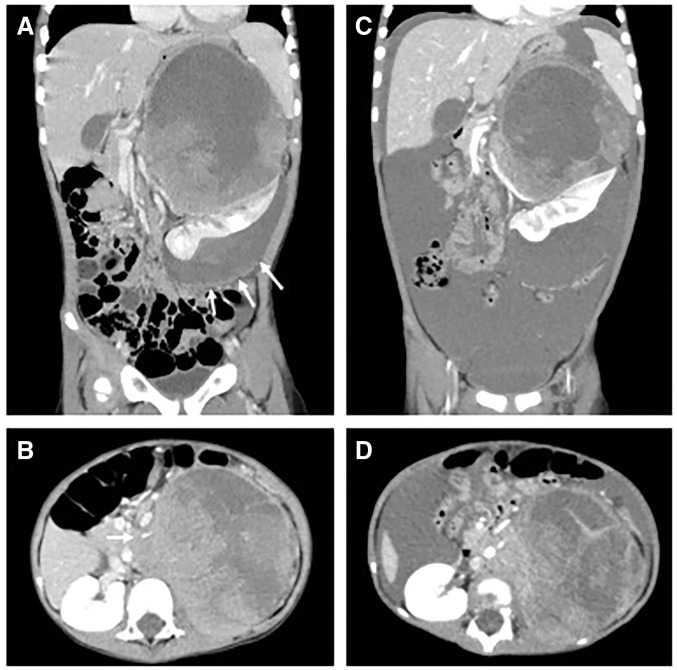 Fig. 1
Fig. 1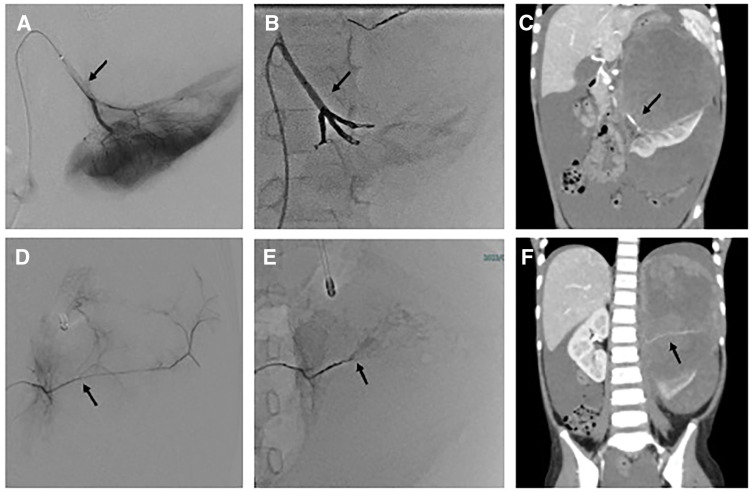 Fig. 2
Fig. 2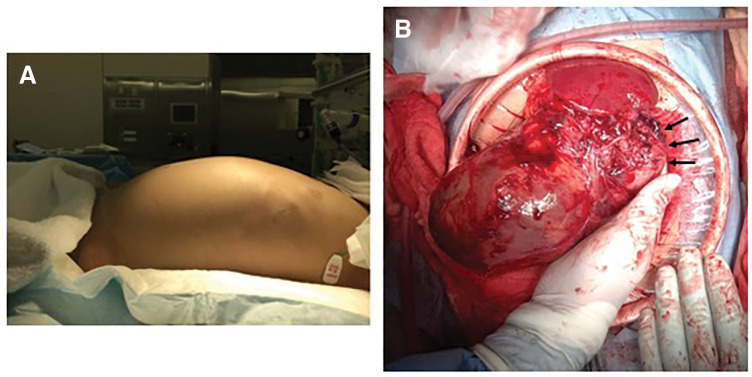 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroblastoma Research and Treatments · Management of metastatic bone disease · Vitamin C and Antioxidants Research
Abbreviations
ACS abdominal compartment syndrome Cre creatinine FFP fresh frozen plasma RCC red cell concentrate TAE transarterial embolization
INTRODUCTION
Neuroblastoma is one of the most prevalent types of solid tumors in the pediatric population. Cases diagnosed at an advanced stage are generally treated using a multimodal approach that includes chemotherapy, surgical intervention, radiotherapy, and immunotherapy.^1)^ MYCN-amplified tumors are associated with a poor prognosis and require intensive therapeutic interventions.^2)^ Although tumor rupture during the initiation of induction chemotherapy is infrequent, it can result in severe complications, including massive intraperitoneal hemorrhage and abdominal compartment syndrome (ACS), particularly in cases characterized by a substantial tumor burden or vascular involvement.^3,4)^ Prompt identification and effective management of these complications are crucial to ensuring patient survival.^5)^
We present a rare case of high-risk MYCN-amplified neuroblastoma in a 4-year-old girl who developed tumor rupture and ACS soon after the initiation of induction chemotherapy that required emergency surgical intervention. Additionally, we examined the significance of risk assessments and therapeutic strategies to similar high-risk scenarios by reviewing the literature.
CASE PRESENTATION
A 4-year-old girl presented to a local clinic with fever and abdominal pain. During examination, a palpable abdominal mass was identified. Subsequent abdominal ultrasonography revealed a substantial tumor located at the upper pole of the left kidney. Therefore, the patient was referred to our hospital for further assessment of the mass. On admission, a hematological analysis indicated anemia with a hemoglobin level of 10.5 g/dL after transfusion of red blood cell concentrate at the referring hospital. Tumor markers were notably elevated; her neuron-specific enolase level exceeded 300.0 ng/mL (normal range: < 16.3 ng/mL). By contrast, urinary catecholamine metabolites remained within the normal limits, with a vanillylmandelic acid level of 5.8 μg/mg creatinine (Cre) and a homovanillic acid level of 21.5 μg/mg Cre. Contrast-enhanced abdominal CT revealed a heterogeneous 17 × 11 × 9.5-cm mass that caused compression of the left kidney. The kidney appeared deformed because of significant displacement and exhibited a beak sign suggestive of possible tumor invasion into the renal parenchyma. Lateral to the kidney, a low-density area encapsulated by a membrane suggestive of a hematoma was also identified (Fig. 1A). The central region of the tumor lacked enhancement, indicating necrosis or tumor degeneration. The left renal artery and vein were encased between the tumor and enlarged para-aortic lymph nodes, consistent with risk factors defined by imaging (Fig. 1B). Metaiodobenzylguanidine scintigraphy demonstrated uptake at the tumor periphery without evidence of distant metastases. PET CT revealed the absence of distant lesions. Based on the elevated tumor markers and imaging findings, a diagnosis of neuroblastoma was established. Owing to the presence of intratumoral hemorrhage and the associated high risk of further bleeding, biopsy was deemed unsafe and therefore postponed. The patient initially received treatment comprising 1 course of COG A3961 chemotherapy, including carboplatin and etoposide, for intermediate-risk neuroblastoma. On day 7, the patient exhibited significant abdominal distention and anemia with a hemoglobin level of 4.7 g/dL. A subsequent contrast-enhanced CT revealed increased ascites; thus, tumor rupture was suspected (Fig. 1C–1D). At the time of clinical deterioration associated with tumor rupture, no marked changes in vital signs were observed, and the patient did not fulfill the criteria for hemorrhagic shock. Laboratory tests showed a hemoglobin level of 4.7 g/dL, and a continuous furosemide infusion was required to maintain urine output. Consequently, emergency transarterial embolization (TAE) was performed targeting the suspected feeding arteries of the tumor, the left renal artery (Fig. 2A–2C), inferior phrenic artery, and adrenal branches of the celiac trunk (Fig. 2D–2F), despite the absence of a clearly identifiable bleeding source. Because multiple feeding arteries to the tumor originated from the renal artery, embolization of the renal artery was unavoidable. Hemorrhage caused by tumor rupture was controlled using TAE. Angiographic hemostasis was achieved in 2 h and 28 min. However, the patient’s intra-abdominal pressure increased from 14 to 20 mmHg after the procedure; during the subsequent 2 h, urine output was 0 mL (anuria), and the patient required endotracheal intubation with invasive mechanical ventilation (Fig. 3A). These findings were consistent with the development of ACS, prompting an emergency laparotomy on the same day. During a midline laparotomy, a substantial volume of hemorrhagic ascites was observed in the abdominal cavity. The neoplasm originated from the left adrenal gland and was accompanied by para-aortic lymphadenopathy encasing the renal hilum and displacing the kidney in a caudal direction. The tumor capsule was ruptured near the inferior aspect of the spleen (Fig. 3B). The renal artery and vein were identified and ligated after dissection through the enlarged lymph nodes, and the left ureter was subsequently transected. En bloc resection of the tumor and left kidney was performed. The operative duration was 4 h and 15 min, and total blood loss was 2968 mL in a 14.4 kg patient who received intraoperative transfusions of RCC 560 mL, FFP 480 mL, and platelet concentrate 10 units (200 mL). A histopathological examination confirmed neuroblastoma originating from the adrenal gland with invasion into the adjacent renal parenchyma. A molecular analysis revealed MYCN amplification. According to the International Neuroblastoma Risk Group,^6)^ this was a high-risk case.
Contrast-enhanced abdominal CT findings. (A, B) Initial contrast-enhanced abdominal CT revealed a well-defined 17 × 11 × 9.5-cm heterogeneous mass compressing the left kidney. A low-density area lateral to the kidney encapsulated by a membrane suggestive of a hematoma was also identified (white arrows in A). The left renal artery and vein were encased between the tumor and enlarged para-aortic lymph nodes, consistent with IDRFs (white arrow in B). (C, D) Contrast-enhanced CT performed 7 days after the initiation of induction chemotherapy revealed increased ascites and findings suggestive of tumor rupture.IDRF, imaging-defined risk factor
Angiography findings. (A–C) Selective angiography images of the left renal artery (arrows) before and after transarterial embolization. (D–F) Images obtained after selective angiography and embolization of the left adrenal artery (arrows), which was identified as a tumor-feeding vessel.
Intraoperative findings. (A) Clinical photograph showing abdominal distension prior to surgery. (B) The tumor capsule was ruptured near the inferior aspect of the spleen (black arrows).
After surgery, chylous ascites developed; however, it resolved by POD 11, thus allowing for drain removal. Chemotherapy utilizing the 05A3 protocol, which included cyclophosphamide, vincristine, pirarubicin, and cisplatin, was recommenced on day 16. The patient completed 11 cycles of chemotherapy, followed by autologous peripheral blood stem cell transplantation, proton beam therapy (30.6yE/17F), and 6 cycles of anti-GD2 antibody treatment. Retinoic acid therapy is currently being considered; however, it has not yet been approved for use in Japan. At 2 years postoperatively, complete remission has been maintained.
DISCUSSION
This report presents a rare but severe case of MYCN-amplified neuroblastoma that resulted in tumor rupture and ACS soon after initiation of induction chemotherapy in a 4-year-old girl. Although hemorrhage that resulted from tumor rupture was controlled by TAE, ACS progression required emergency surgical intervention. Ultimately, a successful outcome was achieved through a multidisciplinary approach.
Tumor rupture in neuroblastoma is a rare but life-threatening complication, particularly during or after chemotherapy. Its pathophysiology involves a sudden increase in intratumoral pressure, progression of necrosis, and breakdown of the immature tumor vasculature.^4,7)^ MYCN-amplified neuroblastomas exhibit high proliferative activity and abnormal vascular structures, rendering them susceptible to hemorrhage and rupture after cytotoxic therapy.^2,8)^ Voglino et al. reported that among 44 patients with high-risk neuroblastoma, 4 (9%) experienced hemorrhagic complications, specifically hemothorax or intraperitoneal bleeding, within 2–7 days after initiating induction chemotherapy.^9)^ Our case involved a high-risk neuroblastoma, and chemotherapy-induced tumor rupture resulted in massive hemorrhagic ascites and ACS. Although rare, high-risk neuroblastoma can have a severe clinical course; therefore, a careful pretreatment assessment is essential. Imaging findings such as large tumor size, capsular tension, central necrosis, and invasion into adjacent organs or vessels may be indicators of potential rupture and should be closely evaluated.
A retrospective analysis of 47 cases of ruptured neuroblastoma identified a tumor diameter greater than 13.2 cm as a significant risk factor for rupture.^3)^ In our case, the tumor measured 17 × 11 × 9.5 cm, with the longest axis at 17 cm; therefore, it was categorized as high risk. However, because intratumoral hemorrhage occurred at presentation, the apparent tumor size may have been enlarged by hemorrhagic expansion; therefore, the dimensions before rupture may not have been accurately reflected. Although the applicability of the cutoff of 13.2 cm remains unclear, tumor enlargement clearly contributed to rupture. The tumor was also identified as an undifferentiated neuroblastoma with MYCN amplification, which is a recognized risk factor for rupture according to genetic pathology.
Intraperitoneal hemorrhage was suspected after the tumor ruptured; therefore, TAE was performed. TAE is a minimally invasive technique that achieves hemostasis; therefore, it has gained attention as an effective method of controlling bleeding in pediatric patients with solid tumors. However, while TAE is generally minimally invasive, it can be time-consuming; for patients in hemorrhagic shock, emergency laparotomy may be prioritized for rapid hemostasis. In our hemodynamically stable patient without shock, the bleeding source appeared embolization-amenable, and immediate surgical backup was available, supporting TAE as the first-line hemostatic approach. Yoshida et al. documented a pediatric case of a ruptured adrenal tumor that was successfully stabilized with TAE before surgery; therefore, TAE may be an effective bridge to surgical intervention for hemorrhagic solid tumors in pediatric patients.^10)^ The literature regarding TAE for tumor rupture with neuroblastoma is limited. This report describes the efficacy of TAE as an initial intervention for tumor rupture in patients with neuroblastoma.
In this case, tumor rupture resulted in rapid intraperitoneal hemorrhage and fluid accumulation. Although TAE achieved temporary hemostasis, sustained elevation of intra-abdominal pressure resulted in ACS. Minimally invasive decompressive procedures, such as percutaneous drainage or hematoma evacuation, are considered first-line interventions for ACS, particularly when tumors are near to major vessels or vital organs, because surgical resection is a high-risk procedure in such cases.^11,12)^ Several studies have reported the effectiveness of these approaches, including percutaneous decompression, which improved intra-abdominal pressure and organ function in pediatric patients.^4,13)^
In the present case, TAE included the left renal artery, which was identified as the major tumor-feeding vessel, thus rendering renal preservation unfeasible. Because nephrectomy was anticipated and the tumor appeared technically resectable, emergency surgery was deemed appropriate. The achievement of en bloc resection of the tumor and left kidney was fortuitous. In contrast, many ruptured neuroblastoma present with extensive involvement of major vessels and adjacent organs, which may preclude safe resection. In such scenarios, conservative management including percutaneous drainage may be the only feasible method of stabilizing intra-abdominal pressure. When definitive resection is not feasible due to extensive vascular involvement or physiological instability, damage control strategies, such as temporary decompression and staged surgery,^4)^ have been reported in rare pediatric cases.Our decision pathway similarly emphasized physiology-first stabilization, escalating from TAE to definitive surgery once ACS criteria were met.
Although surgical resection was definitive and successful in this case, it cannot be universally applied to all patients with tumor rupture and ACS. The decision to proceed with surgery must be carefully individualized by considering the anatomical extent, tumor biology, and hemodynamic stability. Further accumulation of cases and discussions is warranted to determine the optimal strategies for managing ACS in patients with high-risk neuroblastoma after TAE.
CONCLUSIONS
Tumor rupture is a rare but life-threatening complication of high-risk MYCN-amplified neuroblastoma and ACS after induction chemotherapy. Despite hemostasis achieved with TAE, emergency tumor resection was necessary. This case emphasizes the need for pretreatment risk assessments and early surgical readiness of high-risk cases. Surgical resection can serve as a definitive treatment for ACS when anatomically feasible.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maris JM. Recent advances in neuroblastoma. N Engl J Med 2010; 362: 2202–11.20558371 10.1056/NEJ Mra 0804577 PMC 3306838 · doi ↗ · pubmed ↗
- 2Schleiermacher G, Mosseri V, London WB, et al. Segmental chromosomal alterations have prognostic impact in neuroblastoma: a report from the INRG project. Br J Cancer 2012; 107: 1418–22.22976801 10.1038/bjc.2012.375PMC 3494425 · doi ↗ · pubmed ↗
- 3Qin H, Yang S, Cai S, et al. Clinical characteristics and risk factors of 47 cases with ruptured neuroblastoma in children. BMC Cancer 2020; 20: 243.32293329 10.1186/s 12885-020-06720-9PMC 7092550 · doi ↗ · pubmed ↗
- 4Lode HN, Henze G, Siebert N, et al. Management of tumor rupture and abdominal compartment syndrome in an infant with bilateral high risk stage 4 neuroblastoma: a case report. Medicine (Baltimore) 2019; 98: e 16752.31441848 10.1097/MD.0000000000016752 PMC 6716702 · doi ↗ · pubmed ↗
- 5Je BK, Kim HK, Horn PS. Abdominal compartment syndrome in children: clinical and imaging features. AJR Am J Roentgenol 2019; 212: 655–64.30645165 10.2214/AJR.18.20119 · doi ↗ · pubmed ↗
- 6Cohn SL, Pearson AD, London WB, et al. The International Neuroblastoma Risk Group (INRG) classification system: an INRG Task Force report. J Clin Oncol 2009; 27: 289–97.19047291 10.1200/JCO.2008.16.6785 PMC 2650388 · doi ↗ · pubmed ↗
- 7Canete A, Gerrard M, Rubie H, et al. Poor survival for infants with MYCN-amplified metastatic neuroblastoma despite intensified treatment: the International Society of Paediatric Oncology European Neuroblastoma Experience. J Clin Oncol 2009; 27: 1014–9.19171715 10.1200/JCO.2007.14.5839 · doi ↗ · pubmed ↗
- 8Valteau-Couanet D. Event-free survival of patients with high-risk neuroblastoma treated with an N 6-like induction treatment. J Clin Oncol 2005; 23: 6262–3; author reply 6263.10.1200/JCO.2005.01.206216135497 · doi ↗ · pubmed ↗