Serodiagnosis of amoebic abscess: a retrospective diagnostic accuracy study of kits marketed in Europe
E. Prétot, M-P. Brenier-Pinchart, P. Tirard-Collet, F. Gabriel, F. Touafek, A. Marteau, L. Delcey, C. Amiot, D. Dupont, H. Fricker-Hidalgo, H. Sokol, A. Moreno-Sabater, F. Grenouillet

TL;DR
This study compares four serology kits for diagnosing amoebic abscesses, finding that combining certain tests improves accuracy.
Contribution
The study provides a comparative evaluation of four European-market serology reagents for amoebic abscess diagnosis.
Findings
Bordier ELISA showed the highest sensitivity (97.5%) for detecting amoebic abscess.
ELITex Bicolor Amoeba latex reagent had the highest specificity (98.6%).
Combining Bordier ELISA and ELI.H.A Amoeba with ELITex Bicolor Amoeba for confirmation improved diagnostic performance.
Abstract
Amoebiasis is a cosmopolitan parasitic disease caused by Entamoeba histolytica. The most lethal form is extra-intestinal amoebiasis, mainly manifesting as liver abscesses. Diagnosis is based on clinical, radiological, and biological tests. However, there are currently few serology reagents still available on the European market for in vitro diagnosis, and comparative studies of existing reagents are required. We evaluated the performances of the four currently available reagents, either as standalone tests or in combination. Two enzyme-linked immunosorbent assays (ELISAs) for the detection of E. histolytica IgG were assessed: one manufactured by Bordier and the other by NovaTec. Additionally, an indirect hemagglutination technique, ELI.H.A Amoeba, and a latex particle agglutination technique, ELITex Bicolor Amoeba, both produced by ELITech Microbio, were evaluated. A total of 442 serum…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
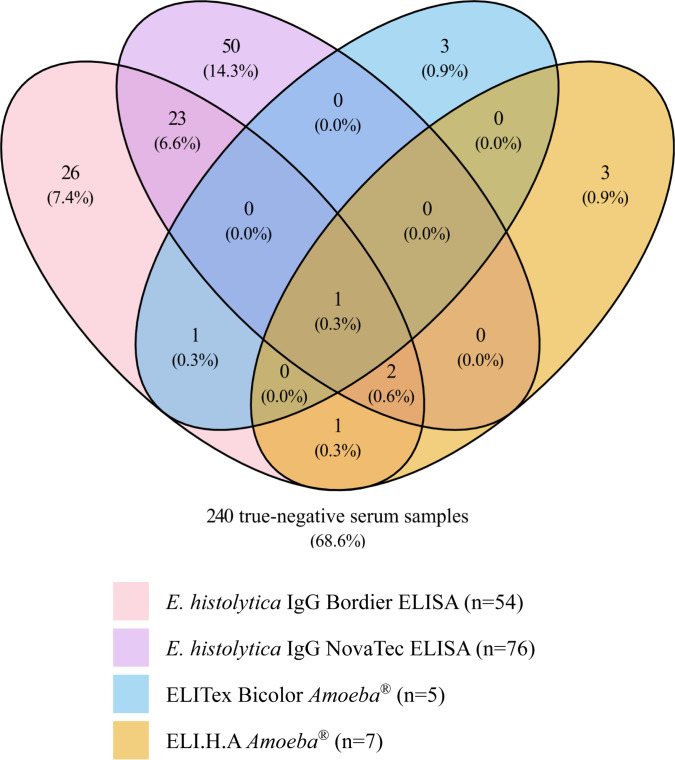 Fig 1
Fig 1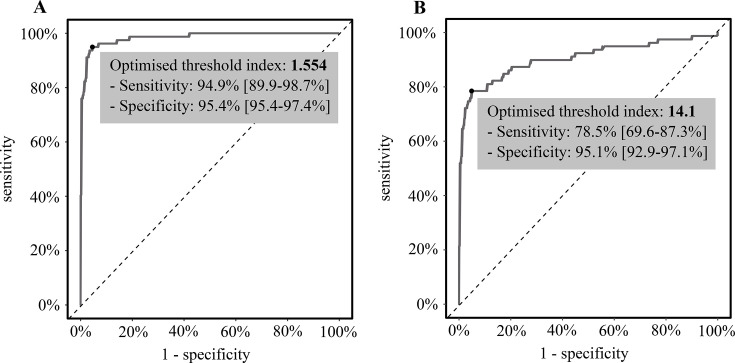 Fig 2
Fig 2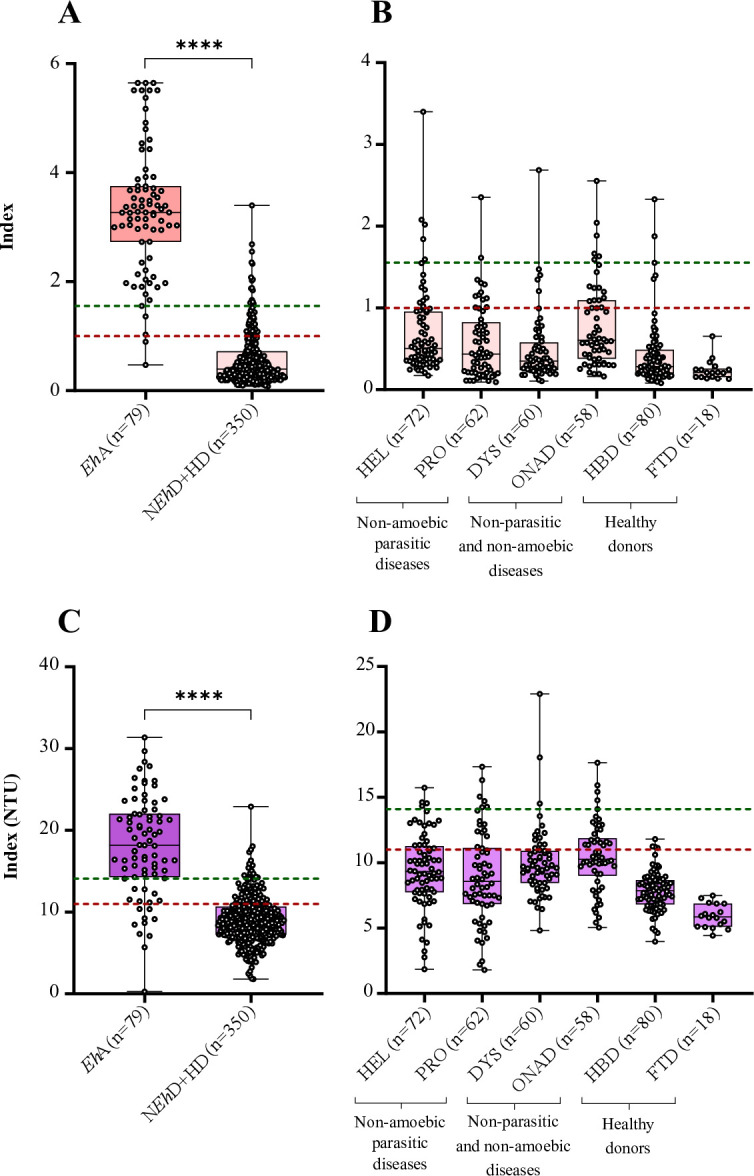 Fig 3
Fig 3| No. tested | Bordier ELISA | NovaTec ELISA | ELI.H.A | ELITex Bicolor | |||||
|---|---|---|---|---|---|---|---|---|---|
| Pos | Neg | Pos | Neg | Pos | Neg | Pos | Neg | ||
| 79 | 77 | 2 | 69 | 10 | 75 | 4 | 71 | 8 | |
| N | 350 | 54 | 296 | 76 | 274 | 7 | 343 | 5 | 345 |
| Se (%) | 429 | 97.5 (97.4–98.8) | 87.3 (87.3–88.6) | 94.9 (94.9–96.2) | 89.9 (89.8–91.1) | ||||
| Sp (%) | 84.6 (84.5–85.8) | 78.3 (78.3–79.5) | 98.0 (98.0–99.3) | 98.6 (98.5–99.9) | |||||
| AUC | 0.984 (0.972–0.997) | 0.905 (0.857–0.953) | 0.983 (0.963–1.003) | 0.948 (0.914–0.982) | |||||
| Accuracy (%) | 86.9 (86.9–88.2) | 80.0 (79.9–81.2) | 97.4 (97.4–98.7) | 97.0 (96.9–98.3) | |||||
| LR+ | 6.32 (6.31–6.65) | 4.02 (4.02–4.05) | 47.47 (47.38–47.61) | 62.91 (62.50–63.09) | |||||
| LR− | 0.03 (0.03–0.04) | 0.16 (0.16–0.17) | 0.05 (0.05–0.06) | 0.10 (0.10–0.11) | |||||
| Commercial method | Threshold | Sensitivity (%) | Specificity (%) | Accuracy (%) | LR+ | LR− |
|---|---|---|---|---|---|---|
| 1 (manufacturer) | 97.5 (97.4–98.8) | 84.6 (84.5–85.8) | 86.9 (86.9–88.2) | 6.32 (6.31–6.65) | 0.03 (0.03–0.04) | |
| 1.554 (optimized) | 94.9 (94.9–96.2) | 95.4 (95.4–96.7) | 95.3 (95.3–96.6) | 20.77 (20.74–20.84) | 0.05 (0.05–0.06) | |
| 11 (manufacturer) | 87.3 (87.3–88.6) | 78.3 (78.3–79.5) | 80.0 (79.9–81.2) | 4.02 (4.02–4.05) | 0.16 (0.16–0.17) | |
| 14.1 (optimized) | 78.5 (78.5–79.7) | 95.1 (95.1–96.4) | 92.1 (92.0–93.3) | 16.16 (16.13–16.22) | 0.23 (0.23–0.24) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmoebic Infections and Treatments · Diagnosis and treatment of tuberculosis · Gallbladder and Bile Duct Disorders
INTRODUCTION
Amoebiasis represents a significant global health concern, with a high mortality rate. Of the 500 million individuals infected with Entamoeba spp. (1), 10% are infected with Entamoeba histolytica (Eh), the only species known to be pathogenic to humans. Invasive forms of amoebiasis, including amoebic liver abscess, are responsible for 50 000 to 70,000 deaths per year (2, 3).
In non-endemic regions, travelers and migrants are the main populations affected. The diagnosis of amoebiasis presents a significant challenge. Digestive forms could be primarily misdiagnosed as inflammatory bowel diseases, and distinguishing amoebic liver abscess from pyogenic liver abscess is difficult. This diagnosis challenge may lead to delayed and/or inadequate management, such as longer diagnostic delay or prescription of inappropriate antibiotics. Serology is primarily employed in the diagnosis of invasive Eh forms. Although serology can also provide information for diagnosing Eh colitis, the gold standard techniques for diagnosis in these cases remain parasitological and/or molecular examination of stool samples (2–4).
In many countries, there is a growing trend towards standardizing diagnostic reagents used in hospital laboratories. This shift has resulted in the abandonment of in-house techniques in favor of commercial assays labeled for in vitro diagnosis. With stricter European regulations regarding the European Conformity marking (5), the distribution of some diagnostic assays was discontinued by manufacturers, i.e., immunofluorescence assays (Amoeba Spot IF, bioMérieux) and Ridascreen enzyme-linked immunosorbent assay (ELISA) (R-Biopharm). As a result, the number of commercial assays for amoebic abscess has been drastically reduced. Re-evaluation of the available reagents is therefore required to implement adequate diagnostic strategies depending on laboratory needs.
Implementing a diagnostic strategy requires both knowledge of how diagnostic tests compare with each other and thorough cross-validation. With this in mind, we carried out a multicenter retrospective study to compare four available serology reagents for diagnosis of amoebic abscess, using a centralized biobank of 442 serum samples from seven university hospitals in France.
MATERIALS AND METHODS
Study design and human samples
This study involved seven parasitology-mycology laboratories in France. Serum samples were collected by each laboratory within the last 10 years and had not undergone repeated freeze-thaw cycles. Samples were centralized in the biobank of the Besançon serology laboratory (SINPAF biobank, authorization AC2023-946) and stored at −20°C until testing. To ensure integrity, samples were excluded if the results were not concordant with the initial results obtained using the same technique.
In order to assess sensitivity or specificity of 95% with an α-risk of 0.05 and a marginal error of 0.05, the required total sample size was 73 (6). Serum samples (one serum sample selected per patient) were collected at the time of diagnosis or during follow-up of liver disease, echinococcosis (up to 1 year), and other parasitic diseases (up to 3 months). Patients were diagnosed with Eh abscess (EhA), Eh colitis (EhC), non-Eh disease (NEhD), such as parasitic disease (helminthiasis or protozoan disease), liver disease or immune dysfunction, or isolated positive Eh routine serology. Healthy donors (HDs) of blood or fecal matter were also included. The diagnostic criteria defining the EhA group were a combination of positive amoebic routine serology, consistent epidemiology, imaging, and treatment with metronidazole resulting in therapeutic success. If available, positive molecular biology was also an argument. The subgroup defined by an "isolated positive Eh routine serology" included patients with positive amoebic serology for one or more Eh techniques, as well as an acute episode that was clinically consistent with an amoebic abscess. However, the diagnosis of amoebiasis was rejected by a multidisciplinary team, and the patients were not treated for this pathology. Other sample selection criteria are described in Table S1.
For patients with an immune dysfunction, serum samples with at least one autoantibody titer greater than 2N (among rheumatoid factors and/or antinuclear antibodies and/or anti-citrullinated peptide antibodies) were selected (N: threshold value for positivity of each antibody respectively defined in the Besançon immunology laboratory). However, for most samples, the levels of autoantibodies were greater than 5N for at least one parameter.
Patient clinical data, including age, sex, date of diagnosis and sample collection, treatment, and outcome, were obtained from medical records.
Serological assays
Four commercial kits were evaluated: ELITex Bicolor Amoeba (latex agglutination (LA)) and ELI.H.A Amoeba (indirect hemagglutination [IHA]) manufactured by ELITech Microbio (Signes, France), and two Eh IgG ELISA kits, one from Bordier Affinity Products (Crissier, Switzerland) and the second from NovaTec Immundiagnostica GmbH (Dietzenbach, Germany).
The same operators used the commercial kits blindly at a single center, over a period of 2 months. Tests requiring macroscopic reading (IHA and LA) were read blindly in duplicate. Assays were conducted following manufacturers’ instructions, and results were interpreted using manufacturer cut-off values (Table S2). Equivocal results were considered negative. Concerning ELITex Bicolor Amoeba, the test was performed semi-quantitatively, allowing for the calculation of a titer. Briefly, a first assessment was performed at a 1:5 dilution. When agglutination was observed, the result was considered positive, and serial 1:2 dilutions were carried out up to 1:40 dilution. A second dilution (1:10) was also performed for samples that initially tested negative (1:5 dilution) by this test but having yielded a positive result in at least one other technique assessed in this study, so as to discard a potential prozone effect.
Statistical analysis
The test parameters were determined using 2 × 2 contingency tables, which allowed for the calculation of sensitivity, specificity, likelihood ratios (LR), area under the curve (AUC), and accuracy. The gold standard was an established diagnosis of amoebic abscess, determined by a combination of positive serology, consistent epidemiology, imaging, and successful treatment outcomes (Table S1). Results were analyzed using receiving operating characteristic (ROC) curves and the Youden index to determine the most appropriate threshold(s) for each ELISA test. The Youden index enables the determination of the optimal combination of sensitivity and specificity for quantitative techniques. The new index established using the Youden index has been used to assess the performance of new techniques and optimize the thresholds of the two quantitative techniques.
Serodiagnostic strategies combining two techniques were also evaluated. Negative results obtained with the first sensitive technique were considered as the final result and were not confirmed, whereas positive results with the first technique were confirmed (or refuted) using a second, more specific technique, which was considered as the final result. Performance was therefore calculated according to these final results from the combination of the two techniques.
Serum samples from patients in the EhC group were excluded from the performance analysis, as the selected kits are not indicated for diagnosis of amoebic colitis.
The data were subjected to a Wilcoxon-Mann-Whitney test for comparison. A P-value of less than 0.05 was considered statistically significant. Generation of figures, graphs, and curves was conducted using R Statistical Software version 4.3.1 (R Core Team 2021, Boston, MA, USA), GraphPad Prism version 8.0.1 (GraphPad Software, Boston, MA, USA) and Microsoft Excel version 2407 (Microsoft, Redmond, WA, USA).
RESULTS
Population characteristics
The study population included 442 patients. Demographic and diagnostic data are presented in Table S3. Patients included in the EhA group (n = 79) had amoebic liver abscess, except one patient who had cecal abscess. Molecular detection of Eh DNA in pus aspirates confirmed the diagnosis in 31 out of 34 patients with Eh amoebiasis (EhA group), for whom data were available (91%). The male-to-female ratio was 5.6, and the median age was 41 (range 2–74) (Table S3).
In order to analyze the kit performances, patients with other parasitic diseases, including eight helminthiases (n = 72) and six protozoan diseases (n = 62), or immune dysfunctions (n = 60), liver diseases (n = 29), or non-relevant isolated positive serology (n = 29) were included in this study (Table S1). Molecular biology ruled out a diagnosis of amoebic liver abscess in six out of the 29 patients of this last subgroup; the results were negative. Donors of blood (n = 80) and fecal matter (n = 18) were also included as the healthy population.
Performances of four commercial tests for Eh tissular abscess diagnosis
Sensitivity of the four kits ranged from 87.3% to 97.5% (Table 1). Bordier ELISA was the most sensitive technique, with only two serum samples yielding false-negative results. ELI.H.A Amoeba showed a sensitivity value comparable with that obtained using Bordier ELISA, with 82% of EhA serum samples exhibiting positivity with a titer ≥1,280 (Fig. S4C). ELITex Bicolor Amoeba demonstrated relatively lower sensitivity (89.9%), yielding eight false-negative results (8/79, 10.1%) (Table 1). Among the EhA group, 41 out of 79 presented a titer higher than 40, and only 3 out of 79 sera yielded a titer of 5, which represents the lowest positive dilution (Fig. S4A). No evidence of a prozone effect was observed with the LA method.
ELITex Bicolor Amoeba demonstrated the highest specificity (98.6%), with only five false-positive results (Table 1; Fig. 1). This method offered the highest increase in post-test probability of the diagnosis of Eh abscess (LR^+^). Specificity of the ELI.H.A Amoeba test is close to that of the ELITex Bicolor Amoeba test (98.0%). The negative LR (LR^-^) of ELI.H.A Amoeba was less than 0.1 (Table 1), indicating a high degree of diagnostic benefit associated with a negative test result (i.e., post-test probability to exclude EhA); the increase in post-test probability LR^+^ was also high. The specificity of the Bordier ELISA was lower than those described above. False-positive results were primarily observed in serum samples from patients with a single isolated positive serology but an excluded diagnosis of amoebiasis (14/54, 26%) (Table S5). A total of 76 false-positive serum samples were observed with NovaTec ELISA, leading to the lower specificity (Table 1).
Venn diagram of false-positive results by technique. Distribution of false-positive results versus true-negative results according to the techniques among patients without E. histolytica disease, i.e., non-E. histolytica diseases and HDs (n = 350; false-positive results for at least one technique n = 110/350, 31.4%; and true-negative results n = 240, 68.6%).
Moreover, many false-positive results were described with one or both ELISA methods (90%, 99/110), whereas very few false-positive results were observed with the LA and IHA methods (Fig. 1). Of the 110 control serum samples (NEhD and HD groups, n = 350) that yielded a false positive result, serum samples belonging to the liver disease or immune dysfunction disease groups had the highest number of false positives, regardless of the method employed (Table S5). In addition, false-positive results were also identified in patients diagnosed with filariasis, echinococcosis, leishmaniasis, and strongyloidiasis when analyzed by ELISA methods. Considering equivocal results as positive increases sensitivity and decreases specificity. The results of the two relevant techniques are provided in Table S6.
Threshold adjustment
In order to improve ELISA assay performances, ROC curves were designed to identify the optimal threshold (Fig. 2A and B). For Bordier ELISA, the optimal Youden index was 0.9, obtained with an ELISA threshold index of 1.554 (Fig. 2A). In contrast, for NovaTec ELISA, the optimal Youden index was lower at 0.74, corresponding to an ELISA threshold of 14.1 NovaTec Units (NTUs) (Fig. 2B).
ROC curves for quantitative techniques. (A) E. histolytica IgG Bordier ELISA (n = 429), reference: diagnosis of amoebic abscess; (B) E. histolytica IgG NovaTec ELISA (n = 429), reference: diagnosis of amoebic abscess.
The newly established thresholds were subsequently applied to the various populations evaluated in this study (Fig. 3). The new threshold allowed for the reduction of false-positive values without an increase in false-negative values for both methods. Table 2 presents a comparison of the performance of the ELISA techniques with the current manufacturer’s threshold and the optimized threshold. These optimizations increased the specificity of each ELISA to 95.4% and 95.1% for Bordier and NovaTec ELISAs, respectively, with a slight decrease in sensitivity for Bordier ELISA (94.9%) but a greater decrease for NovaTec ELISA (78.5%).
*Representation of index values. (A, B) By group for E. histolytica IgG Bordier ELISA, according to manufacturer’s threshold (red line = 1) and optimized threshold index (green line = 1.554) in the total cohort (n = 429) (A) or focused on non-Eh (n = 252) and HD (n = 98) subgroups (n = 350) (B). (C-D) By group for E. histolytica IgG NovaTec ELISA, according to manufacturer’s threshold (red line = 11) and optimized threshold index (green line = 14.1) in the total cohort (n = 429) (C) or focused on non-Eh (n = 252) and HD (n = 98) groups (n = 350) (D). EhA, E. histolytica abscesses; NEhD, non-E. histolytica diseases; HD, healthy donor; HEL, helminthiases; PRO, protozoan diseases; DYS, immune dysfunctions; ONAD, others non-amoebic diseases (liver diseases and isolated positive serology); HBD, healthy blood donor; FTD, fecal transplant donors. ns, non-significant, ***: significant difference, <10−4.
Evaluation of serodiagnostic strategies
Strategies combining a sensitive first-line screening test with a confirmatory test for positive first-line results were evaluated. The combination of two screening commercial kits (Bordier ELISA and IHA) increased sensitivity to 97.5%. The combination of the most sensitive techniques (Bordier ELISA and/or IHA) confirmed by the LA technique provided specificity of 99.7%, with the highest post-test probability.
Eh colitis
Eight out of the 13 samples from patients with amoebic colitis yielded positive results with all techniques employed, while three samples remained negative with all techniques (Table S7). In cases where serological tests yielded positive results, antibody levels were notably elevated. The median index for Bordier ELISA was 2.06, while NovaTec ELISA yielded a value of 16.73 NTU. Additionally, the median titers for IHA and LA were 5,120 and 20, respectively.
DISCUSSION
The results of this multicenter retrospective accuracy study demonstrated that Bordier ELISA and ELI.H.A Amoeba exhibited the highest sensitivity for Eh serological diagnosis. The ELITex Amoeba LA kit had the highest specificity value, demonstrating a low incidence of false positives in comparison to the ELISA kits. When the LA method is combined with one of the two sensitive techniques, the proportion of false-positive results is improved, particularly those observed with ELISA techniques. Furthermore, the extensive cohort of serum samples used in this study made it possible to establish improved ELISA thresholds and to reduce false-positive results.
As previously reported (7), Bordier ELISA is a sensitive technique for the diagnosis of EhA. However, our study revealed lower specificity than previously reported (84.6% versus 94.0%), probably due to the high diversity of sera included in our cohort, such as patients with liver disease or immune disorders. Concerning the ELI.H.A Amoeba technique, previously marketed as IHA Amibiase (Fumouze Diagnostics), our study obtained similar performances in terms of sensitivity and specificity to those previously reported (8–10). ELITex Amoeba, formerly marketed as Bichro-Latex Amibe test (Fumouze Diagnostics), has been described as a highly specific technique for Eh serological diagnosis (95%–99.5%) and with a sensitivity value comparable to the ELISA and hemagglutination methods (90.7%–97.8%) (1, 8–10). In contrast, our results revealed that the LA method was less sensitive in this study for the diagnosis of EhA than Bordier ELISA and ELI.H.A Amoeba. NovaTec ELISA demonstrated suboptimal sensitivity and specificity, as previously reported in the study of Larréché et al. (9). Interestingly, the values stated on the manufacturer’s website are 100.0% and 98%, respectively (11). This discrepancy is likely attributable to the design of the cohort.
Previous accuracy evaluation studies are scarce and relatively old. Thus, the observed differences in performances can be attributed to variations in the manufacture of the reagents. The discrepancies in specificity observed between studies may also be due to the size of the population studied and the subjective selection of control cases. In addition, these parameters probably influence the proportion of equivocal results (13.3% in the NEhD group in our study vs 9% in the study conducted by Boisseau (12) for the hemagglutination technique), which were considered negative in our study. Although we considered equivocal results to be negative, in practice, an equivocal result in a highly suggestive context would lead health care providers to consider an equivocal result as positive, or to repeat the test. Our research has also shown that optimizing the commercial threshold is crucial for enhancing the efficacy of commercial methods, but this requires access to a well-defined and well-conserved biobank.
It should be noted that the present study has limitations. Based on a multicenter biobank, the four techniques were performed in a single center. This could have artificially increased the performance of the hemagglutination technique, particularly. This technique is known to be associated with high interlaboratory variability due to environmental conditions, especially room temperature (13). Moreover, the availability of reagents should be considered, as this will impact the feasibility of adapting the current findings.
Another limitation is the study design. The very low prevalence of amoebic abscesses in high-income countries makes it impossible to carry out a non-retrospective study. Only studies conducted in an area with a high prevalence of amoebiasis could be prospective and allow for the predictive values of these tests to be calculated. From another point of view, the diversity of the sera included is a major strength of the study. Dysimmunitary diseases are increasingly common, and amoeba serology is part of systematic screening for donors of fecal matter in France (14), but not internationally (15). The occurrence of false-positive results in this population initially led to the rejection of donations. However, thanks to the optimization of the positive threshold through this study focused on ELISA methods, primarily used as an initial screening method, this issue should no longer be a concern. Furthermore, the inclusion of routine ELISA false-positive sera represents an intentional bias with a definite impact on the observed specificity. Another limitation is that the positive status of the serums for amebiasis was previously determined using different techniques. This may therefore call the gold standard into question.
Finally, this study also reveals that positive serology is very often associated with amoebic colitis (16, 17), although serology is not indicated for the diagnosis of this clinical form of amoebiasis (1, 18). The use of serological diagnosis for EhA is therefore difficult to interpret in highly endemic areas, as it cannot distinguish between past and current infection or scarring amoebiasis (18–20). Even in our study outside an endemic area, we cannot rule out the possibility that some false positives were patients with an old infection, but with residual antibodies.
In conclusion, large comparative studies are needed to guide clinical microbiologists in their choices. This is even more important for parasitic diseases, such as amoebic abscesses, which are rare in routine practice. In low- to middle-income countries, reagent choice is also influenced by laboratory equipment and the availability of reagents. Our work provides baseline data for what would ideally be a prospective multicenter accuracy study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1van Doorn HR, Hofwegen H, Koelewijn R, Gilis H, Peek R, Wetsteyn J, van Genderen PJJ, Vervoort T, van Gool T. 2005. Use of rapid dipstick and latex agglutination tests and enzyme-linked immunosorbent assay for serodiagnosis of amebic liver abscess, amebic colitis, and Entamoeba histolytica cyst passage. J Clin Microbiol 43:4801–4806. doi:10.1128/JCM.43.9.4801-4806.200516145144 PMC 1234111 · doi ↗ · pubmed ↗
- 2Stanley SL. 2003. Amoebiasis. Lancet 361:1025–1034. doi:10.1016/S 0140-6736(03)12830-912660071 · doi ↗ · pubmed ↗
- 3Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, et al.. 2012. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2095–2128. doi:10.1016/S 0140-6736(12)61728-023245604 PMC 10790329 · doi ↗ · pubmed ↗
- 4Shirley D-A, Farr L, Watanabe K, Moonah S. 2018. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis 5:ofy 161. doi:10.1093/ofid/ofy 16130046644 PMC 6055529 · doi ↗ · pubmed ↗
- 5Regulation (EU) 2017/746 of the European Parliament and of the Council of 5 April 2017 on in vitro diagnostic medical devices and repealing Directive 98/79/EC and Commission Decision 2010/227/EU. 2017 P. 176-332. https://eur-lex.europa.eu/legal-content/EN/TXT/HTML/?uri=CELEX%3A 32017 R 0746.
- 6Hajian-Tilaki K. 2014. Sample size estimation in diagnostic test studies of biomedical informatics. J Biomed Inform 48:193–204. doi:10.1016/j.jbi.2014.02.01324582925 · doi ↗ · pubmed ↗
- 7Beyls N, Cognet O, Stahl J-P, Rogeaux O, Pelloux H. 2018. Serodiagnosis of extraintestinal amebiasis: retrospective evaluation of the diagnostic performance of the Bordier ELISA Kit. Korean J Parasitol 56:71–74. doi:10.3347/kjp.2018.56.1.7129529853 PMC 5858671 · doi ↗ · pubmed ↗
- 8Robert R, Mahaza C, Bernard C, Buffard C, Senet JM. 1990. Evaluation of a new bicolored latex agglutination test for immunological diagnosis of hepatic amoebiasis. J Clin Microbiol 28:1422–1424. doi:10.1128/jcm.28.6.1422-1424.19902199503 PMC 267943 · doi ↗ · pubmed ↗