Expert Opinion: A Call for Early and Appropriate Symptomatic Treatment in Acute Respiratory Infections to Prevent Escalation
Peter Kardos, Andrzej Fal, André Gessner, Ernest Kuchar, Christian Ude, Ludger Klimek

TL;DR
This paper argues for early and proper treatment of acute respiratory infections to reduce symptoms and prevent complications.
Contribution
The paper emphasizes the underutilized potential of non-antibiotic symptomatic treatments to manage acute respiratory infections effectively.
Findings
Appropriate early treatment can reduce symptom severity and illness duration.
Non-antibiotic therapies have clinical and mechanistic support for managing acute respiratory infections.
Better management could reduce societal burden and antimicrobial resistance.
Abstract
Acute respiratory infections are highly prevalent and significantly impair quality of life and productivity. Despite their impact, they are often not managed according to best medical practice. A lack of knowledge about symptomatic therapies leads to mis- and under-treatment. Thus, this narrative expert opinion paper aims to highlight the importance of appropriate and early symptomatic treatment in order to assist informed therapeutic decision making and advance efforts to reduce antibiotics misuse. Clinical and mechanistic evidence supports the use of several herbal and synthetic non-antibiotic treatment options. While acute respiratory infections are usually self-limiting, treatment alleviates symptom severity, reducing the risk of inflammatory escalation. Timing of the intervention is crucial, as early initiation shortens illness duration. In conclusion, optimizing the management of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
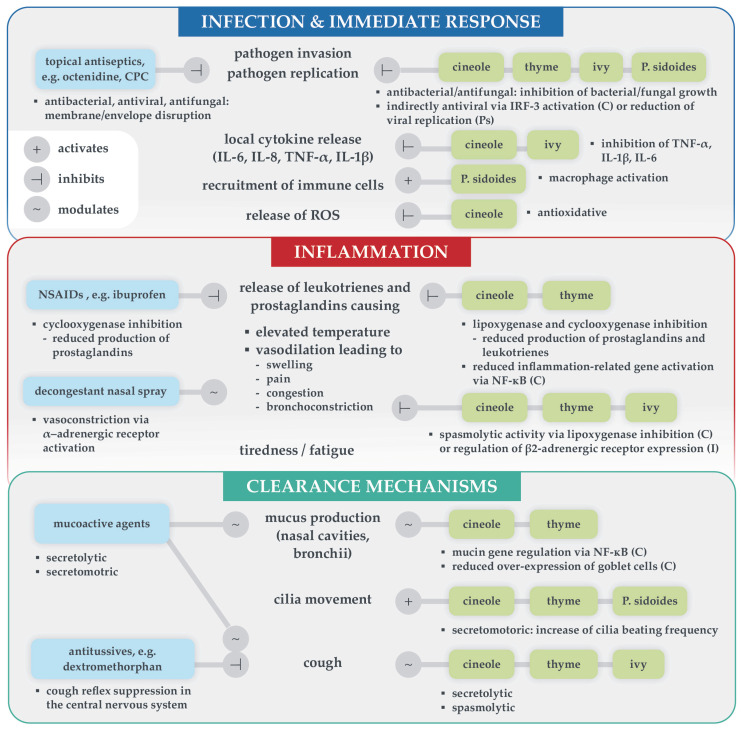 Figure 2
Figure 2- —MCM Klosterfrau Vertriebsgesellschaft mbH, Klosterfrau Healthcare Group
- —Bavarian Ministry of Science and the Arts, in the framework of the Bavarian Research Network “New Strategies Against Multi-Resistant Pathogens by Means of Digital Networking-bayresq.net”
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory and Cough-Related Research · Herbal Medicine Research Studies · Pediatric health and respiratory diseases
1. Introduction
The common cold, an umbrella term for acute upper respiratory tract infections, has substantial prevalence, peaking during the winter months in Europe [1,2]. Adults have, on average, 2–4 colds per year and children 5–8, which typically last 7–10 days. Although self-limiting, acute respiratory infections pose a significant burden on patients’ quality of life and substantially impact society due to loss of productivity, absenteeism and healthcare usage. Despite recent awareness campaigns highlighting the typically viral etiology of these diseases, irrational antibiotic treatment of uncomplicated respiratory infections remains common, contributing to the continuous and rapid increase in antimicrobial resistance [3,4]. A Europe-wide analysis revealed that almost 50% of ambulant antibiotic prescriptions were filled for respiratory infections, resulting in a reduction potential of an estimated 66–84 million packages per year, irrespective of a viral cause [3]. Driver analyses have shown that inappropriate antibiotic prescriptions for respiratory infections are partly attributable to a lack of knowledge about evidence-based symptomatic treatments, especially among the general public [5,6]. These treatments include anti-inflammatory and mucolytic herbal and synthetic pharmaceuticals, as well as topical antiseptics. Despite healthcare professionals’ (HCPs) and patients’ interest in non-antibiotic treatments, there is still uncertainty about which therapeutic options are beneficial for alleviating and shortening this usually self-limiting disease [6].
This narrative expert opinion paper therefore aims to provide an overview of clinical and mechanistic evidence for symptomatic treatments endorsed by European guidelines and supply strategies to optimize management of acute respiratory infections in practice.
2. Preventing Inflammatory Escalation in Respiratory Infections
In addition to alleviating the severity and duration of symptoms, the objective of treating acute respiratory infections is to reduce the risk of inflammatory escalation. Acute respiratory infections commonly present with a symptom cascade of sore throat, nasal and sinus congestion, headaches, cough and sometimes fever [1]. Dysregulated cytokine release plays a central role in infectious diseases: these symptoms result from a uniform and excessive innate immune response, independent of the causative pathogen [2]. In the course of a respiratory infection, symptoms usually increase during the first days due to the activation of different immune processes and clearance mechanisms, as illustrated in Figure 1. Simultaneously, resolution mechanisms are triggered, leading to a gradual spontaneous decline in inflammation and, usually, remission [7].
However, in some cases, inflammation escalates due to insufficient pathogen elimination or dysregulated mediator release, leading to self-reinforcing, excessive pro-inflammatory cytokine load (“cytokine storm”) and may require intensive treatment [8]. Escalation can lead to complications, sepsis, and acute respiratory distress syndrome. While escalation is generally rare, vulnerable groups such as small children, the elderly, and people with immunodeficiency or chronic diseases are at increased risk, as recently evidenced during the SARS-CoV-2 pandemic [8,9]. Especially in chronic conditions such as asthma, bronchiectasis, and chronic obstructive pulmonary disease, acute respiratory infections comprise the main cause of exacerbations and hospitalization [2]. Preventative strategies focus on vaccination, which is unfortunately not a feasible option against most common cold pathogens and vaccination rates are usually too low to achieve herd immunity. Instead, symptomatic treatments are available to alleviate symptoms and achieve a milder clinical course.
3. Evidence-Based Symptomatic Treatment
Clinical and mechanistic evidence suggests that several herbal and synthetic symptomatic treatments can significantly reduce symptom severity and duration of acute respiratory infections [10,11,12,13,14]. Options endorsed in relevant European guidelines include eucalyptus extract, its main constituent 1,8-cineole, ivy, thyme, and pelargonium extracts, as well as non-steroidal anti-inflammatory drugs (NSAIDs) [15,16,17,18,19].
Briefly, 1,8-cineole reduced bronchitis symptoms and cough significantly and with clinical relevance after 4 days in a placebo-controlled trial [12]. In addition to efficacy, timing, i.e., early intervention, is vital for accelerated symptom relief: an exploratory trial demonstrated that starting 1,8-cineole within 24 h of symptom onset shortened common-cold duration by approximately 1.5 days [10]. Ivy extract has been shown to significantly reduce cough frequency at day 7 in children versus baseline, and several studies have shown reduced cough and bronchoconstriction [13]. A fixed thyme/primrose extract reduced cough score by 47% in patients with acute bronchitis versus placebo in a double-blind RCT [11]. A Cochrane review demonstrated low-to-moderate efficacy for Pelargonium sidoides extract against acute rhinosinusitis and common cold [14], while another Cochrane review showed that NSAIDs can significantly relieve cold-related pain and sneezing, but not symptom score, duration or cough [20]. Additionally, topical antiseptics and herbal extracts can effectively reduce pathogen load. Treatment options targeting singular symptoms include nasal decongestants, synthetic mucoactive agents, or antitussives. However, many antitussives are not effective against acute cough [21]. Pathophysiological processes, the resulting symptoms and mechanisms of action of effective synthetic (left) and herbal (right) symptomatic treatment options are summarized in Figure 2. Mechanistic evidence is presented grouped by their target process below.
3.1. Pathogen Elimination
Topical antiseptics octenidine and cetylpyridinium chloride act directly by disrupting the integrity of lipid membranes, thus showing a broad unspecific antiseptic activity effective against various pathogens with low risk of resistance development [22]. Herbal treatments, on the other hand, have been shown to inhibit bacterial and fungal growth—demonstrated in preclinical studies [23]—and to act indirectly antiviral by upregulating cellular defense mechanisms [24,25,26].
3.2. Cytokine Regulation
Cineole and ivy extract have been shown to inhibit the release of pro-inflammatory cytokines, tumor necrosis factor α (TNF-α), and interleukins 1 and 6, thereby reducing local pro-inflammatory load [27,28].
3.3. Immune Cell Regulation
Immune cells, primarily leukocytes, are recruited to sites of inflammation. Pelargonium sidoides extract has been shown to boost this immune response by macrophage activation [26].
3.4. Antioxidation
Reactive oxygen species (ROS) are released upon apoptosis of infected cells, leading to the release of downstream mediators and causing harm to surrounding healthy cells. Cineole has been shown to have antioxidative effects, like many other plant extracts [27].
Overview of target immune processes and resulting symptoms [2] in relation to mechanisms of action of synthetic (left) and herbal (right) symptomatic treatments for acute respiratory infections. Anchors indicate activation, inhibition or modulation of the process. Detailed mechanisms are mentioned if known (octenidine [22], CPC [29], decongestant nasal spray [30], ibuprofen [31], dextromethorphan [21], cineole [24,25,27,32], ivy extract [28,33], thyme extract [34,35], P. sidoides extract [26]). Abbreviations: C cineole, CPC cetylpyridinium chloride, I ivy, IL interleukin, IRF interferon regulatory factor, NF-κB nuclear factor kappa B, NSAIDs non-steroidal anti-inflammatory drugs, Ps Pelargonium sidoides, ROS reactive oxygen species, TNF tumor necrosis factor.
3.5. Prostaglandin Regulation
Cineole, thyme extract, and NSAIDs inhibit the production of prostaglandins via the cyclooxygenase pathway [24,31,33,34]. Prostaglandins (as well as leukotrienes) are the cause of most symptoms, as their release leads to increasing body temperature and vasodilation, which in turn results in swelling, congestion, pain and bronchoconstriction, if the lungs are affected. Nasal decongestants target α-adrenergic receptors in the nose to reduce local vasodliation and swelling [30].
3.6. Secrete Mobilization
Herbal medicines support intrinsic clearance mechanisms, as many have mucolytic effects and secretomotoric effects via mucin gene regulation and cilia activation [34,36,37]. There are synthetic mucoactive substances available too, e.g., erdosteine, which has mucolytic effects and activates the cilia [33].
3.7. Cough Relief
Spasmolytic action has been demonstrated for plant-isolated compounds such as 1,8-cineole and α-hederin (contained in ivy extract) via modulation of α- and β-adrenergic receptors, respectively, in the respiratory tract, as well as for other plant extracts [28,35,37]. Synthetic antitussives such as dextromethorphan primarily target the central nervous system [21].
4. Strategies to Optimize Treatment of Acute Respiratory Infections
There is a need for effective symptomatic treatment of acute respiratory infections, not least to reduce antibiotic misuse. Symptom relief and shortening of disease duration with herbal and synthetic therapeutics is both feasible and in compliance with current guideline recommendations [15,16,17,18,19]. Yet, approximately 50% of ambulant antibiotic prescriptions for respiratory infections could be avoided due to viral cause [6]. To improve management of acute respiratory infections in practice, actions on both the individual physician, pharmacist, and patient level as well as the institutional level are necessary.
While HCPs were generally well educated regarding the efficacy of antibiotics, they need to be more familiar with effective non-antibiotic treatment options, their optimal application, and how their use contributes to antimicrobial stewardship efforts [6]. The benefit of early treatment on quality of life and activity impairment should be emphasized, highlighting that the old conviction ‘treatment does not affect symptom duration’ has been disproven [10,38]. This could be achieved by common cold-specific continuing medical education programs (CME) and additional information material provided by pharmaceutical companies. Additionally, the position of symptomatic treatments in guidelines must be strengthened. Therefore, large trials with consistent and comparable endpoints would be most useful, but require additional funding and support from non-profit or government organizations to be feasible. Expert societies or international consensus conferences should work together to reduce contradictory or inconsistent recommendations, e.g., between specialist and general practitioner guidelines (cf. [15,16]).
Patients have demonstrated significantly less knowledge about the efficacy of antibiotics in the context of respiratory infections compared to HCPs [6]. They require trustworthy information—especially in the light of a multitude of non-verifiable medical information provided by social media and artificial intelligence (AI) chat bots. Educational material should include red flags requiring immediate medical attention, the risks of inappropriate antibiotics use, which symptomatic treatments are effective instead and inform that they should be initiated as early as possible for maximum benefit. Pharmacists, in particular, take a central role in counseling patients with acute respiratory infections. As they are usually the first and often only point of care, they are in the unique position to provide patients with evidence-based advice and effective over-the-counter treatment options. Recommendations by physicians have a significant impact on patient perception of the necessity of treatment and feasible options as well. Thus, addressing early and effective symptomatic treatment when patients present themselves for certification of sick leave is advisable. On the institutional level, patient information websites run by government institutions, health insurances, and medical societies should be continuously updated to comply with current guidelines and antimicrobial stewardship strategies.
5. Conclusions
This multidisciplinary expert opinion featuring early symptomatic as opposed to antibiotic treatment of the common cold is based on both clinical experience of the authors as well as on a search of published literature. Moreover, many specialist and general medicine guidelines support effective and safe symptomatic treatment options for acute respiratory infections. It is imperative to implement evidence-based knowledge on the optimal management of acute respiratory infections among both HCPs and patients, emphasizing the benefit of early treatment initiation and the necessity to avoid inappropriate antibiotics use.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kardos P. Malek F.A. Common Cold—An Umbrella Term for Acute Infections of Nose, Throat, Larynx and Bronchi Pneumologie 20177122122610.1055/s-0042-11611227912214 PMC 7117077 · doi ↗ · pubmed ↗
- 2Heikkinen T. Järvinen A. The Common Cold Lancet 2003361515910.1016/S 0140-6736(03)12162-912517470 PMC 7112468 · doi ↗ · pubmed ↗
- 3Gessner A. Klimek L. Kuchar E. Stelzmueller I. Fal A.M. Kardos P. Potential Saving of Antibiotics for Respiratory Infections in Several European Countries: Insights from Market Research Data Antibiotics 202312117410.3390/antibiotics 1207117437508270 PMC 10376894 · doi ↗ · pubmed ↗
- 4Seedat J. Winkler M. Harendt N. Epidemiologisches Bulletin 20-21/2025 Robert-Koch-Inst.2025 Available online: https://www.rki.de/DE/Aktuelles/Publikationen/Epidemiologisches-Bulletin/2025/20-21_25(accessed on 15 September 2025)
- 5Machowska A. Stålsby Lundborg C. Drivers of Irrational Use of Antibiotics in Europe Int. J. Environ. Res. Public Health 2018162710.3390/ijerph 1601002730583571 PMC 6338985 · doi ↗ · pubmed ↗
- 6Fal A.M. Stelzmüller I. Kardos P. Klimek L. Kuchar E. Gessner A. Antibiotics Usage and Avoidance in Germany and Poland: Attitudes and Knowledge of Patients, Physicians, and Pharmacists Antibiotics 202413118810.3390/antibiotics 1312118839766578 PMC 11672592 · doi ↗ · pubmed ↗
- 7Robb C.T. Regan K.H. Dorward D.A. Rossi A.G. Key Mechanisms Governing Resolution of Lung Inflammation Semin. Immunopathol.20163842544810.1007/s 00281-016-0560-627116944 PMC 4896979 · doi ↗ · pubmed ↗
- 8Jarczak D. Nierhaus A. Cytokine Storm—Definition, Causes, and Implications Int. J. Mol. Sci.2022231174010.3390/ijms 23191174036233040 PMC 9570384 · doi ↗ · pubmed ↗