Sternoclavicular Joint Septic Arthritis Following Blunt Trauma: Successful Surgical Management and One-Year Outcome
Kamil R Jarjess, John E Tobia, Saif L Juma, Jamil Haddad, Matthew J Yousif

TL;DR
A 63-year-old man developed sternoclavicular joint septic arthritis after chest trauma and was successfully treated with surgery and antibiotics, leading to full recovery.
Contribution
This case highlights the successful surgical and medical management of a rare post-traumatic SCJ septic arthritis.
Findings
Surgical irrigation and debridement, along with antibiotic therapy, resolved the infection and restored joint function.
One-year follow-up showed no recurrence and full range of motion in the affected joint.
Chronic active inflammation was confirmed histologically, but no acute osteomyelitis was present.
Abstract
We report a case of sternoclavicular joint (SCJ) septic arthritis in a previously healthy non-smoker 63-year-old male following a direct blunt impact to the anterior chest, which served as the only identifiable predisposing factor. The patient presented with a two-month history of left SCJ pain, swelling, and a chronic draining sinus tract. Laboratory findings demonstrated leukocytosis and elevated inflammatory markers, while aspiration cultures grew methicillin-sensitive Staphylococcus aureus. Surgical management included irrigation and debridement of the SCJ with saucerization of the necrotic medial clavicle and sinus tract excision with fat pad flap closure of the SCJ, saucerization of the necrotic medial clavicle, and excision of the sinus tract with fat pad flap closure, followed by two months of intravenous antibiotics via peripherally inserted central catheter. Pathology revealed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
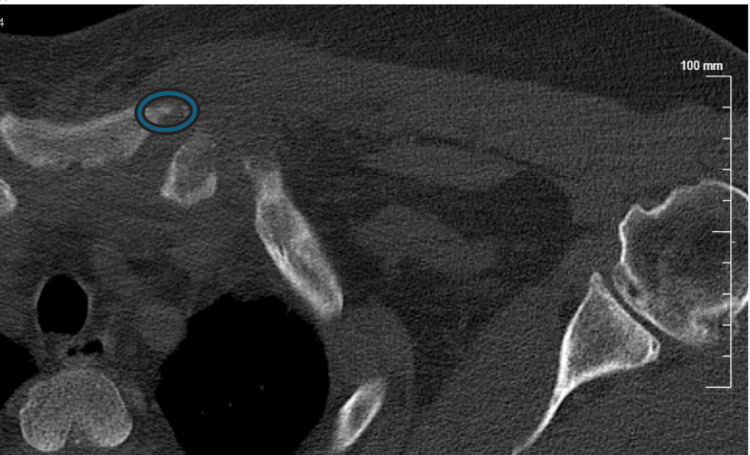 Figure 1
Figure 1 Figure 2
Figure 2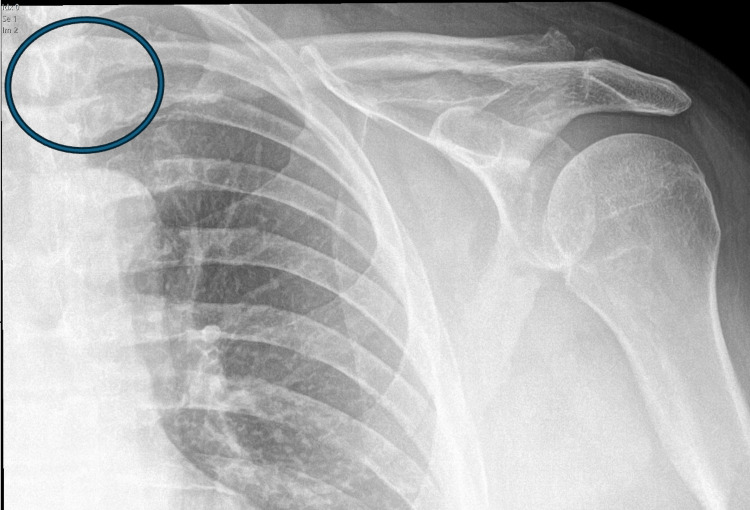 Figure 3
Figure 3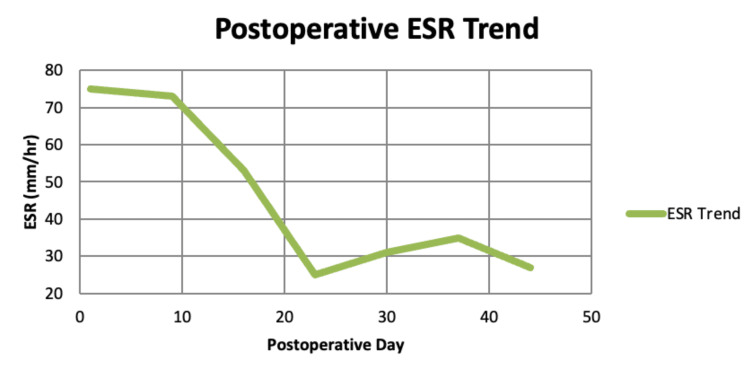 Figure 4
Figure 4| Test | Patient value | Reference range (adult male) | Interpretation |
| White blood cell count (×10³/µL) | 12.7 | 4.5–11.0 | High |
| Platelet count (×10³/µL) | 578 | 150–400 | High |
| CRP (mg/L) | 172 | <5 | High |
| ESR (mm/hr)* | 105 | ≤20 (men >50 y) | High |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder and Clavicle Injuries · Orthopedic Infections and Treatments · Infectious Diseases and Tuberculosis
Introduction
The sternoclavicular joint (SCJ) is a synovial saddle-like joint with an intra-articular disc composed of fibrocartilage lining [1,2]. The SCJ’s tight, poorly distensible capsule can generate high intra-articular pressures, which can promote dissemination of infection into surrounding tissues [2,3]. Furthermore, due to the SCJ’s intimate posterior relationship with the great vessels of the mediastinum, including the brachiocephalic vein, an infection can lead to devastating complications such as septic thrombophlebitis or mediastinitis [2,4,5].
SCJ infection is a rare condition, accounting for less than 1% of all septic arthritis cases [6]. It occurs predominantly in male patients presenting with chest pain. It is associated with a variety of risk factors such as diabetes mellitus, immunosuppression, intravenous drug use, and traumatic injury to the SCJ [2,4,6]. Blunt trauma to the chest wall can introduce infection directly or potentially exacerbate a transient, subclinical bacteremia [7]. However, as the sole identifiable etiology without systemic risk factors, it is rare, accounting for only ~12% of cases [1-3].
In order to prevent the spread of infection into the pleural space, mediastinum, and the great vessels, early recognition and swift treatment of SCJ infection is vital [8]. When treating SCJ infections, the literature reports that approximately 85% of all cases are managed with en bloc resection, 10% with debridement, and 5% with incision and drainage [7]. However, due to the nature of risk factors such as chest facets and wound events associated with invasive surgical procedures, minimally invasive surgical approaches should always be considered for patients with SCJ infection [7,9]. The SCJ joint's proximity to the great vessels of the mediastinum, such as the brachiocephalic vein and the superior vena cava, makes surgical management challenging and proves why posterior SCJ dislocations are dangerous [10,11]. Following broad-spectrum antibiotic therapy and diagnostic testing showing early stages of infection, simple incision and drainage represent one form of minimally invasive management in cases with no evidence of osteomyelitis or mediastinal involvement [6,7,12]. In comparison to incision and drainage, debridement remains a controversial treatment option for SCJ infection due to its higher recurrence rates and risks of persistent infection, requiring further surgical intervention [13].
We report the case of a non-smoker 63-year-old male, who developed an SCJ infection following blunt chest trauma, with no systemic risk factors identified, and was successfully treated with incision and drainage.
Case presentation
A 63-year-old male patient presented to the clinic with a two-month history of progressive pain, erythema, swelling, and a chronic draining sinus tract over the left sternoclavicular (SC) joint. He reported a history of blunt trauma to the joint approximately two months prior to presentation but denied intravenous drug use, recent systemic infection, or other known risk factors for septic arthritis. His medical history was prominent for a deep vein thrombosis with inferior vena cava filter placement 15 years before presentation to the clinic.
Preoperative CT images of the SCJ were obtained, which demonstrated erosive changes at the medial clavicle with cortical destruction and irregular joint margins. The axial cuts revealed surrounding soft tissue swelling consistent with inflammatory extension, while the coronal view confirmed asymmetric joint widening with bony erosion of both the clavicular and sternal sides of the articulation (Figures 1, 2). These findings supported the diagnosis of septic arthritis of the SC joint with adjacent osseous involvement, prompting the decision for operative intervention.
CT scan (bone window)The axial CT scan with bone window at the level of the sternoclavicular joint demonstrates cortical irregularity and erosive changes involving the medial (sternal) end of the left clavicle. The blue circled region highlights cortical disruption and periarticular erosion on the clavicular side, with adjacent soft tissue swelling suggestive of inflammatory extension beyond the joint.
CT scan (coronal view)The coronal CT reveals asymmetric widening of the left sternoclavicular joint compared to the contralateral side. The blue circled region highlights osseous destruction at the medial clavicle and adjacent manubrial articulation. Surrounding soft tissue density changes suggest an infectious or inflammatory process, possibly with phlegmon formation.
Initial laboratory results obtained by the infectious disease (ID) service revealed leukocytosis (WBC 12.7 × 10³/µL; normal: 4.5-11.0 × 10³/µL), thrombocytosis (platelets 578 × 10³/µL; normal: 150-450 × 10³/µL), elevated C-reactive protein (172 mg/L; normal: <5 mg/L), and an erythrocyte sedimentation rate (ESR) of 105 mm/hr (normal: 0-20 mm/hr in males) [13-15] (Table 1). Ultrasound-guided aspiration of the SC joint showed methicillin-sensitive Staphylococcus aureus (MSSA). Given persistent symptoms and continued drainage despite initial management, surgical exploration was recommended.
The patient underwent irrigation and debridement of the left SC joint, saucerization of the necrotic medial clavicle, closed reduction and manipulation under anesthesia, and excision of the chronic draining sinus tract with fat pad flap closure. Multiple intraoperative specimens, including bone and soft tissue, were collected and sent for histopathology and microbiological cultures (anaerobic, fungal, acid-fast bacillus, and wound cultures) before administration of antibiotics. Clindamycin 600 mg IV was administered intraoperatively after specimen collection. A 6-cm midline incision over the SC joint was made, the chronic draining sinus tract was excised, and a fat pad flap was fashioned for closure. Saucerization of the necrotic medial clavicle was performed. No drains or implants were placed. Intraoperatively, there was no gross purulence, but the distal clavicle demonstrated necrotic changes. Postoperative imaging revealed no acute fracture, dislocation, or residual subluxation (Figure 3).
Postoperative anteroposterior radiograph of the left shoulderAnteroposterior radiograph of the left shoulder demonstrating resection of the medial (sternal) end of the clavicle (circled in blue). Joint alignment is preserved with no evidence of residual dislocation or acute fracture.
Pathology findings
Gross examination of the surgical specimen revealed a 2.5 × 1 × 0.3 cm aggregate of hard tan-red bone fragments mixed with focal tan-pink soft tissue. Microscopic analysis demonstrated fibrocartilaginous tissue with chronic active inflammation and fragments of bone with hemorrhage and reactive changes. No definitive features of acute osteomyelitis were identified.
At postoperative week 1, cultures from the operative site grew moderate Staphylococcus aureus and a few gram-positive cocci in clusters with rare polymorphonuclear leukocytes. The patient was admitted for intravenous antibiotics, and a peripherally inserted central catheter (PICC) line was placed for prolonged therapy under ID guidance. ID service recommended cefazolin 2 g IV every 8 hours, which was continued for approximately two months. The PICC line was removed approximately two months later upon completion of the antibiotic course.
At the time of follow-up, the patient demonstrated complete wound healing, resolution of pain and swelling, and a return to baseline function without recurrence of infection. At one year postoperatively, clinical evaluation revealed a painless, anterior, reducible subluxation with a painless, symmetrical, and full range of motion of the left SCJ with a Constant-Murley score of 83.
Discussion
SCJ infections are rare, accounting for less than 1% of all septic arthritis cases [6]. They are most often associated with systemic risk factors such as intravenous drug use, diabetes mellitus, immunosuppression, and indwelling central venous catheters [2,6]. In contrast, our patient’s only notable history was localized trauma two months prior to symptoms onset, demonstrating that even in the absence of systemic risk factors, mechanical injury may predispose to infection.
This case represents a delayed presentation rather than a delayed diagnosis, as the patient did not seek medical attention until two months after the onset of symptoms. The prolonged, untreated course likely contributed to the chronic features observed, including necrotic changes of the medial clavicle and adjacent osteitis, as evident on imaging. Interestingly, histopathology revealed chronic inflammation without acute osteomyelitis, showcasing the variable pathological spectrum of SCJ infections.
Typical presenting complaints in SCJ infection include localized pain and swelling over the joint, often accompanied by erythema and limited range of motion of the upper extremity due to pain, and some patients might experience fever, malaise, or constitutional symptoms [2]. Early symptoms can mimic other musculoskeletal conditions of the upper chest or shoulder girdle, leading to a delay in diagnosis due to a low index of suspicion [2].
Staphylococcus aureus, particularly methicillin-sensitive strains (MSSA), remains the most common pathogen isolated in SCJ infections [16]. Our patient’s cultures confirmed MSSA both preoperatively and in the early postoperative period. The presence of a chronic draining sinus tract and necrotic clavicular bone without histological evidence of acute osteomyelitis is unusual. This may represent a contained, chronic infective process where the immune response had walled off the infection, leading to bony necrosis without the typical acute inflammatory infiltrate of osteomyelitis. It may represent a transition from acute to chronic infection with partial containment by surrounding tissues.
From a laboratory perspective, our patient demonstrated significant systemic inflammation at presentation, with leukocytosis (WBC 12.7 × 10³/µL), thrombocytosis (platelets 578 × 10³/µL), elevated C-reactive protein (172 mg/L), and an ESR of 105 mm/hr. Postoperatively, inflammatory markers were closely monitored, showing a progressive decline in ESR: 75 mm/hr (postoperative day 1), 73 mm/hr (postoperative day 9), 53 mm/hr (postoperative day 16), 25 mm/hr (postoperative day 23), 31 mm/hr (postoperative day 30), 35 mm/hr (postoperative day 37), and 27 mm/hr (postoperative day 44) (Figure 4). This downward trend paralleled the patient’s clinical improvement, supporting effective infection control and resolution of the inflammatory process.
Postoperative ESR trendPostoperative ESR trend demonstrating progressive decline from 75 mm/hr on day 1 to 27 mm/hr by day 44, correlating with the patient’s clinical improvement and infection resolution.ESR, erythrocyte sedimentation rate
Management of SCJ infections generally requires a combined approach of surgical intervention and targeted antibiotic therapy [2]. While the primary goal of surgery was infection control, the extensive debridement and bony resection create a local inflammatory environment that, in rare cases, can predispose to heterotopic ossification as a delayed complication. This process of aberrant bone formation has been documented in various soft tissues following trauma or surgical intervention, including highly atypical locations [17], making postoperative vigilance necessary to monitor for this potential sequela. This approach of treatment aligns with the literature emphasizing aggressive local control to prevent the recurrence of SCJ infection [16,18]. In one of the most extensive institutional series, Ali et al. reported recurrence rates as low as 2.3% overall, with flap-assisted closures achieving the most durable results [18]. Similarly, Kachala et al. found an approximate 10% recurrence rate after surgical management, with the majority of recurrences occurring in the early postoperative course [19]. Our patient’s successful outcome following debridement and flap closure aligns with reports suggesting that, in cases without mediastinal extension or extensive osteomyelitis, debridement can achieve comparable infection control to en bloc resection while minimizing morbidity [2,7].
Conclusions
We reported a SCJ infection in a 63-year-old man following blunt chest trauma without systemic risk factors. Operative irrigation and debridement, including saucerization and sinus-tract excision, along with fat pad flap closure and prolonged cefazolin therapy, achieved durable infection control. The patient returned to baseline function with a Constant-Murley score of 83 and had no recurrence at one year. This case highlights the importance of timely recognition, focused surgery, a tailored antimicrobial plan, and coordinated multidisciplinary care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sternoclavicular septic arthritis: review of 180 cases Medicine (Baltimore) Ross JJ Shamsuddin H 1391488320041511854210.1097/01.md.0000126761.83417.29 · doi ↗ · pubmed ↗
- 2Diagnosis and management of sternoclavicular joint infections: a literature review J Thorac Dis Tasnim S Shirafkan A Okereke I 441844261220203294435510.21037/jtd-20-761PMC 7475584 · doi ↗ · pubmed ↗
- 3Sternoclavicular infectious arthritis in previously healthy adults Semin Arthritis Rheum Bar-Natan M Salai M Sidi Y Gur H 1891953220021252808310.1053/sarh.2002.37284 · doi ↗ · pubmed ↗
- 4Sternoclavicular joint arthritis Arthritis Rheum Yood RA Goldenberg DL 232239231980698799110.1002/art.1780230215 · doi ↗ · pubmed ↗
- 5Sternoclavicular joint Shoulder Elbow Dhawan R Singh RA Tins B Hay SM 2963051020183021449710.1177/1758573218756880 PMC 6134528 · doi ↗ · pubmed ↗
- 6Sternoclavicular joint septic arthritis in a healthy adult: a rare diagnosis with frequent complications J Bone Jt Infect Gonçalves RB Grenho A Correia J Reis JE 389392620213474584610.5194/jbji-6-389-2021 PMC 8567852 · doi ↗ · pubmed ↗
- 7Minimally invasive surgery for sternoclavicular joint infection with osteomyelitis, large abscesses, and mediastinitis Case Rep Surg Ota H Ishida H Matsumoto H Ishiyama T 9461619202220223631704710.1155/2022/9461619 PMC 9617732 · doi ↗ · pubmed ↗
- 8Sternoclavicular joint infection Stat Pearls [Internet] Tapscott DC Benham MD Treasure Island, FL Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/31869185/31869185 · pubmed ↗