Plasmapheresis as a Life-Saving Measure for Severe Hypertriglyceridemia-Induced Acute Pancreatitis
Fahad Neduvancheri, Fathima Shahana Sumi, Rooby Shaheer, Muhammed Shereef M, Sajeesh Sivadas, Thejus Kallarikkandi, Ranjit Narayanan

TL;DR
Plasmapheresis helped save a young woman's life from a rare and severe condition involving high triglycerides and pancreatitis.
Contribution
This case demonstrates plasmapheresis as a novel and effective treatment for severe hypertriglyceridemia-induced acute pancreatitis.
Findings
A 26-year-old woman with severe HTG-induced acute pancreatitis was successfully treated with plasmapheresis.
Plasmapheresis combined with insulin therapy led to significant clinical and biochemical improvement.
The case suggests plasmapheresis could be a life-saving intervention in similar critical scenarios.
Abstract
Severe hypertriglyceridemia (HTG) presenting as acute pancreatitis (AP) in the setting of diabetic ketoacidosis (DKA) is a rare combination, reported as the enigmatic triad in literature. Here we present a case of a 26-year-old woman, with diabetes mellitus (DM) for three years, who presented with features suggestive of acute pancreatitis complicated with DKA in addition to systemic inflammatory response syndrome (SIRS) and acute respiratory distress syndrome (ARDS). Evaluation revealed severe HTG to the tune of 9947 mg/dL. She was managed with insulin infusion combined with three sessions of plasmapheresis, which led to marked clinical and biochemical improvement. This case highlights the importance of plasmapheresis as a lifesaving therapeutic option for severe HTG-induced AP.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
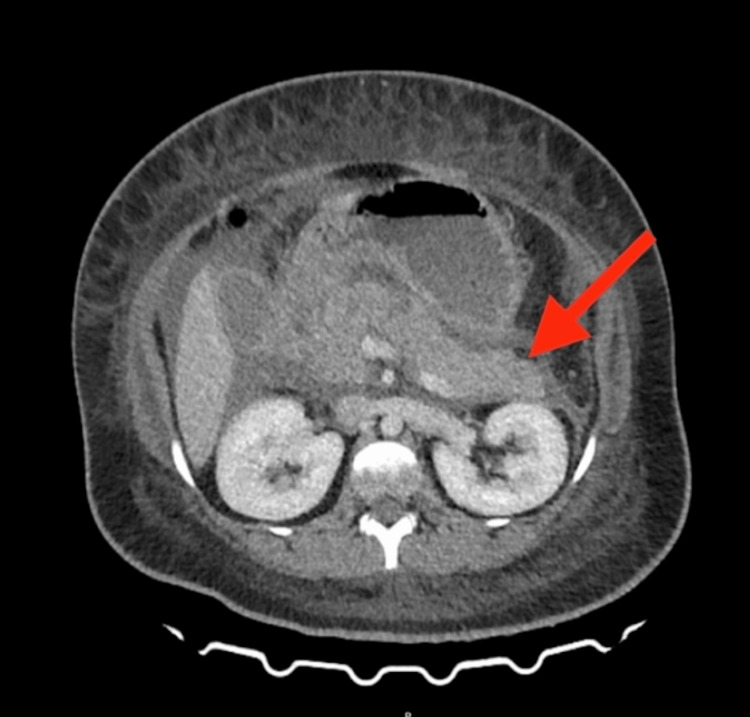 Figure 1
Figure 1 Figure 2
Figure 2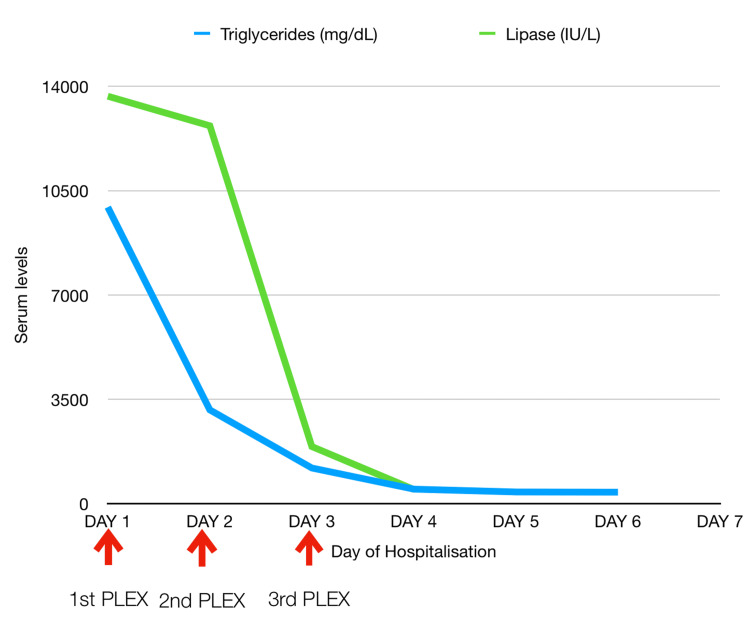 Figure 3
Figure 3| Lab test | Result | Reference value |
| Hemoglobin | 20.0 g/dL | 12-15 |
| Total leukocyte count | 17570/μL | 4000-10000 |
| Platelet | 4.18 lakhs/μL | 1.5-4.10 |
| Amylase | 313 IU/ L | 30-110 |
| Lipase | 13671 IU/L | 23-300 |
| Creatinine | 0.6 mg/dL | 0.5-1.0 |
| Blood urea nitrogen | 6.14 mg/dL | 9-20 |
| Random blood sugar | 229 | <200 |
| Total bilirubin | 0.5 | 0.2-1.3 |
| Direct bilirubin | 0.3 | 0.0-0.3 |
| Alanine transaminase | 33 U/L | 14-36 |
| Aspartate transaminase | 18 U/L | 14-36 |
| Alkaline phosphatase | 117 U/L | 38-126 |
| Sodium | 134 mmol/L | 137-145 |
| Potassium | 5.4 mmol/ L | 3.5-5.1 |
| Calcium (corrected) | 8.8 mg/dL | 8.4-10.2 |
| Triglycerides | 9947 mg/dL | <150 |
| ABG | Patient value | Reference range |
| pH | 6.95 | 7.35-7.45 |
| PaO2 | 139 mmHg | 180-220 |
| PaCO2 | 14 mmHg | 35-45 |
| HCO3 | 3.1 mmol/L | 22-26 |
| Lactate | 2.9 mmol/L | 0.5-2.2 |
| Anion gap | 19.2 mmol/L | 8-14 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Lipid metabolism and disorders · Liver Disease Diagnosis and Treatment
Introduction
The majority of acute pancreatitis (AP) is caused by gallstones (40%-70%) and alcohol (25%-35%) [1]. Hypertriglyceridemia may be associated with AP, usually when their levels are higher than 1000 mg/dL [2,3]. We report a case of a 26-year-old woman with hypertriglyceridemia and uncontrolled diabetes who presented to the emergency room (ER) with a clinical diagnosis of AP and, on evaluation, had diabetic ketoacidosis (DKA) and respiratory dysfunction.
A marked improvement in the patient's general condition and laboratory parameters was noticed following plasmapheresis. This case report highlights the role of plasmapheresis in the rapid reduction of severe hypertriglyceridemia in the setting of AP. In this instance, it served as a lifesaving therapeutic modality.
Case presentation
A 26-year-old woman with diabetes mellitus for three years and treatment non-compliance, presented to our ER with severe epigastric pain and multiple episodes of vomiting suggestive of acute pancreatitis. She denied any history of alcohol use. The patient was afebrile, with a blood pressure of 120/70 mmHg, heart rate of 92/min, and oxygen saturation of 97% on room air. Initial blood workup (Table 1) showed leukocytosis (17570/μL) with elevated C-reactive protein (297 mg/dL) and high serum lipase (13671 IU/L) and amylase (313 IU/L) levels. Her liver function tests (LFTs) and renal function tests (RFTs) were within normal limits. Blood sugars were 229 mg/dL at the time of presentation with a HbA1c of 12.9% indicating poorly controlled DM. Computed tomography of the abdomen showed bulky pancreas with peripancreatic fat stranding with no areas of calcification or evidence of gallstones--suggestive of acute pancreatitis. According to the Modified Marshall Score [4], she was initially managed conservatively with bowel rest and intravenous Ringer’s lactate. However, she developed acute onset dyspnea with desaturation from the ward approximately four hours after admission, necessitating shift to the medical intensive care unit.
Further workup revealed high glucose levels (503 mg/dL) and high-anion-gap metabolic acidosis (Table 2), with 4+ blood ketones. Etiological workup for acute pancreatitis revealed severe hypertriglyceridemia (9947 mg/dL) with normal corrected calcium levels (8.8 mg/dL).
She was promptly started on noninvasive ventilation (NIV), insulin infusion, and intensive intravenous fluid therapy (at the rate of 1.5 mL/kg/h). Subsequently, a contrast-enhanced computed tomography of the abdomen showed diffusely bulky pancreas with peripancreatic fat stranding and non-enhancing necrotic areas (Figure 1). Peripancreatic fluid was noted extending to the pelvis. The modified CT severity index was 8, suggesting severe involvement.
CT scan of abdomen and pelvis with contrast showing bulky pancreas with peripancreatic fat stranding and non-enhancing necrotic areas seen. Peripancreatic fluid noted extending to anterior renal fascia, para-colic gutters and forming a collection in pelvis.
Considering the drastic worsening of the patient's general condition and high levels of triglycerides, a decision to undertake plasmapheresis was made in consultation with nephrology. A total of 1.75 liters of plasma was removed (Figure 2) and replaced with fresh frozen plasma (FFP) and 5% albumin. Following the first session of plasmapheresis, her triglyceride levels dropped down to 3144 mg/dL. After the second session, it decreased to 1193 mg/dL, and after the third session, it decreased to 484 mg/dL (Figure 3). In total, three sessions of plasmapheresis were performed. The patient improved clinically and was shifted out of the intensive care unit by day four. Her subsequent hospital course was complicated by persistent fever with negative blood and urine cultures. She improved in due course with broad-spectrum empirical antibiotics (meropenem) and was discharged on day 12 in a clinically stable condition.
Chylous plasma filtered by plasmapheresis.
Decreasing trend of triglyceride and lipase levels after initiating plasmapheresis (PLEX).
Discussion
The triad of DKA, hypertriglyceridemia, and acute pancreatitis is a rare clinical occurrence, reported in only 4% of cases [5]. The bidirectional relationship between uncontrolled diabetes and hypertriglyceridemia has been highlighted previously [6]. While uncontrolled diabetes is a well-documented cause of hypertriglyceridemia, triglycerides as high as 9000 mg/dL suggests a primary etiology [7].
The role of plasmapheresis in HTG-induced AP still remains controversial, with literature presenting two contrasting perspectives. While specific therapies like heparin and insulin infusion are indicated in hypertriglyceridemia-induced acute pancreatitis [8], the American Society of Apheresis guidelines have approved the use of therapeutic plasmapheresis in the setting of worsening systemic inflammation or lactic acidosis [9].
In a study involving 111 episodes of HTG-induced AP treated with plasmapheresis, the average reduction in triglycerides following plasma exchange was 59%, which was double the reduction seen with conservative treatment (27%) [10]. Absolute indications for plasmapheresis, as cited in previous literature, include (a) pancreatitis refractory to pharmacological approaches, (b) serum triglycerides >1000 mg/dL, (c) serum lipase exceeding three times the upper limit of normal, (d) hypocalcemia, (e) lactic acidosis, and (f) worsening inflammation and organ dysfunction [11]. As our case fulfilled five out of the six criteria mentioned, plasmapheresis was deemed the preferred therapeutic option.
Although there has been no evidence of mortality advantage with plasmapheresis, a study focusing on 25 patients with triglyceride levels exceeding 5000 mg/dL found that the patients who received plasmapheresis had a significantly shorter hospital stay of five days compared to 11 days in those who did not receive it [12]. It has also been reported that plasma exchange improves outcomes by removing pro-inflammatory markers and cytokines, which further dampens the inflammatory process in HTG-induced AP [7]. Evidence also suggests that the early initiation of plasmapheresis, that is, within 24 to 96 hours after the onset of symptoms, has proven beneficial [13].
Conclusions
This case reinforces the value of considering plasmapheresis as a therapeutic option in carefully selected patients with hypertriglyceridemia-induced acute pancreatitis with serious sequelae. Our experience highlights that timely initiation may help in stabilizing patients with high-risk features such as significant organ dysfunction and extreme triglyceride levels. Additionally, the favorable outcome in our patient underscores the importance of multidisciplinary decision-making and individualized treatment strategies in critical care settings, while also recognizing that recent evidence has questioned its routine use because of cost and potential complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence and clinical characteristics of hypertriglyceridemic acute pancreatitis: a retrospective single-center study World J Gastroenterol Lin XY Zeng Y Zhang ZC Lin ZH Chen LC Ye ZS 394639592820223615755010.3748/wjg.v 28.i 29.3946 PMC 9367230 · doi ↗ · pubmed ↗
- 2Comprehensive review on the pathogenesis of hypertriglyceridaemia-associated acute pancreatitis Ann Med Qiu M Zhou X Zippi M Goyal H Basharat Z Jagielski M Hong W 22659395520233781310810.1080/07853890.2023.2265939 PMC 10563627 · doi ↗ · pubmed ↗
- 3Therapeutic plasma exchange in patients with hyperlipidemic pancreatitis World J Gastroenterol Chen JH Yeh JH Lai HW Liao CS 227222741020041525908010.3748/wjg.v 10.i 15.2272 PMC 4724982 · doi ↗ · pubmed ↗
- 4Assessing the efficacy of modified Marshall scoring system in severity assessment of acute pancreatitis in comparison to Ranson score at tertiary centre Int Surg J Vashistha A Khandelwal RG Om P Rundla Rundla MM 17641770102023
- 5Acute pancreatitis induced by diabetic ketoacidosis with major hypertriglyceridemia: report of four cases Case Rep Crit Care Bouchaala K Bahloul M Bradii S Kallel H Chtara K Bouaziz M 7653730202020203231370510.1155/2020/7653730 PMC 7160714 · doi ↗ · pubmed ↗
- 6Hypertriglyceridemia-induced acute pancreatitis with lipemic samples in a type 2 diabetic patient: a case report in a resource-limited setting Int Med Case Rep J Ahmed HM Osman MH Hassan SA Dirie HM Mohamed MA 64564930202510.2147/IMCRJ.S 516349 PMC 1213446640470378 · doi ↗ · pubmed ↗
- 7Management of hypertriglyceridemia induced acute pancreatitis Biomed Res Int Garg R Rustagi T 472135726201810.1155/2018/4721357 PMC 608353730148167 · doi ↗ · pubmed ↗
- 8Hypertriglyceridemia induced acute pancreatitis: 4 years' experience from a tertiary care institute and quick literature review J Family Med Prim Care Kumar BGV Prasad K Singh D Sethy PC 336033671120223611931210.4103/jfmpc.jfmpc_1426_21PMC 9480712 · doi ↗ · pubmed ↗