A Diagnostic Challenge: Sclerosed Hepatic Haemangioma Mimicking Malignancy
Umar A Lakhani

TL;DR
An elderly patient's liver lesion was initially suspected to be cancerous but was diagnosed as a benign sclerosed haemangioma after a biopsy.
Contribution
This case emphasizes the diagnostic challenge of distinguishing benign sclerosed haemangiomas from liver malignancies in elderly patients.
Findings
Imaging alone can be misleading in diagnosing sclerosed haemangiomas as malignant liver lesions.
Liver biopsy and multidisciplinary discussion are crucial for accurate diagnosis in complex cases.
Conservative management is appropriate for benign lesions with comorbidities.
Abstract
A 75-year-old lady presented to Accident and Emergency (A&E) with acute worsening shortness of breath and new palpitations. On assessment, she was found to have fast atrial fibrillation, signs of heart failure, and bilateral peripheral oedema. Investigations revealed pulmonary embolism and an incidental hepatic lesion on CT imaging, suspicious for malignancy. Multidisciplinary discussion led to liver biopsy, which confirmed a benign sclerosed haemangioma. The patient was managed conservatively for cardiac and thromboembolic complications. This case highlights the difficulty in differentiating sclerosed haemangiomas from malignant liver lesions on imaging alone and underscores the importance of biopsy and multidisciplinary decision-making in elderly patients with comorbidities. Learning points include diagnostic vigilance, safe management of anticoagulation, and avoidance of unnecessary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
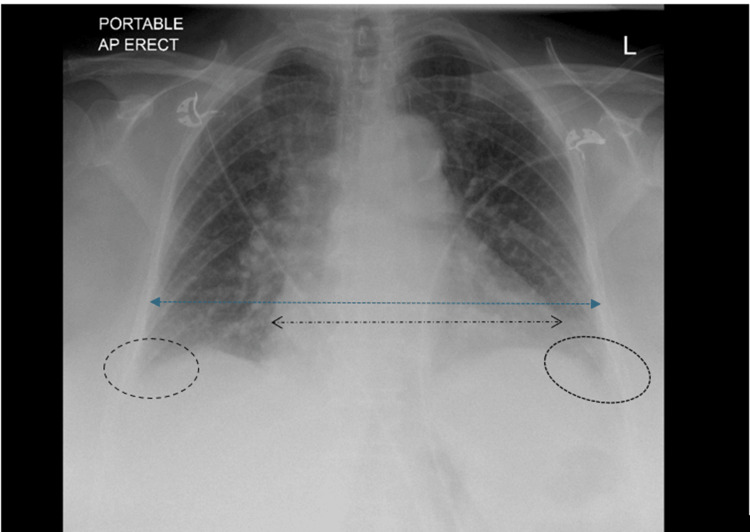 Figure 1
Figure 1 Figure 2
Figure 2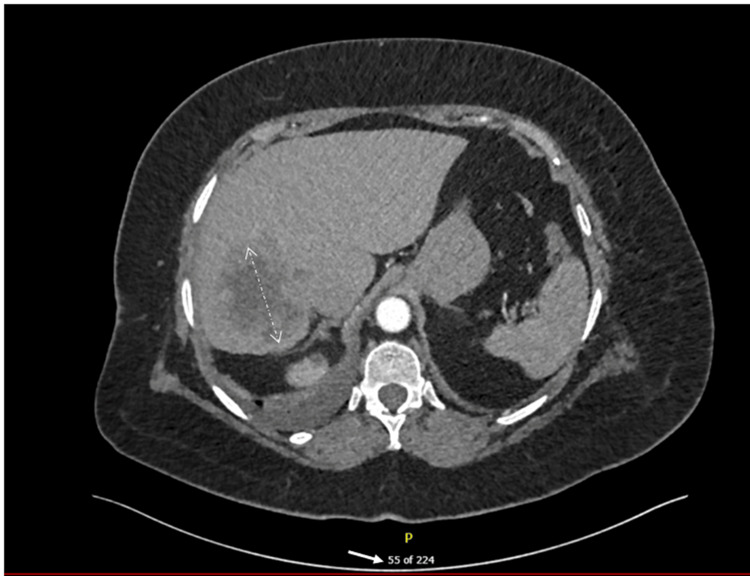 Figure 3
Figure 3 Figure 4
Figure 4| Test | Result | Reference range |
| Haemoglobin | 139 g/L | 115–160 g/L |
| White cell count | 9.6 × 10⁹/L | 4.0–11.0 × 10⁹/L |
| C-reactive protein | 40 mg/L | < 5 mg/L |
| B-type natriuretic peptide | 1946 pg/mL | < 100 pg/mL |
| D-dimer | 4109 µg/L | < 500 µg/L |
| International normalised ratio | 1.1 | 0.9–1.2 |
| Urea and electrolytes | Within normal limits | — |
| Carbohydrate antigen 19-9 | 15 U/mL | < 37 U/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and Kidney Cyst Diseases · Histiocytic Disorders and Treatments · Polyomavirus and related diseases
Introduction
Hepatic haemangiomas are the most common benign liver tumours, accounting for a prevalence of roughly 0.4-20% [1]; but the sclerosed (hyalinised) variant accounts for fewer than 2% of all cases [2]. These lesions develop as cavernous haemangiomas undergo fibrosis, hyalinisation, and vascular thrombosis. In light of these pathological changes, the typical radiological features of haemangiomas-peripheral nodular enhancement with progressive centripetal filling-are often absent. Instead, sclerosed haemangiomas may display irregular peripheral enhancement, central hypodensity, capsular retraction, or calcification, features that closely mimic intrahepatic cholangiocarcinoma or secondary metastases [3,4].
Misinterpretation of imaging can result in unnecessary surgical resections. Histological confirmation is therefore crucial in atypical cases. We present a case in which a large sclerosed hepatic haemangioma was discovered incidentally during investigation for acute cardiopulmonary symptoms. This case is notable for its diagnostic complexity, the impact of comorbidities such as heart failure and pulmonary embolism, and the pivotal role of multidisciplinary decision-making in avoiding major hepatic surgery.
Case presentation
A 75-year-old woman presented with a seven-day history of progressive shortness of breath, palpitations, and ankle swelling. She denied chest pain or fever. On examination, she was found tachycardic with an irregular pulse at 132 beats per minute. Blood pressure was 118/76 mmHg, respiratory rate was 24 breaths per minute, and oxygen saturation was 94% on room air. Clinical examination revealed raised jugular venous pressure, bibasal crackles, and bilateral pitting oedema, consistent with decompensated heart failure.
Investigations
The electrocardiogram demonstrated fast atrial fibrillation with a ventricular rate of approximately 140 beats per minute. A chest radiograph revealed cardiomegaly and bilateral pleural effusions (Figure 1).
Chest X-rayIn this image, the heart borders have been highlighted in comparison to the thoracic borders, which clearly demonstrates a cardiothoracic ratio of >0.5. The costophrenic angles are also blunted, which have been highlighted bilaterally. As can be seen in this patient's chest X-ray, an increased cardiothoracic ratio and blunting of the costophrenic angles are visible, suggesting heart failure with pleural effusion, potentially secondary to heart failure.
The patient's laboratory findings are summarised in Table 1.
Computed tomography pulmonary angiography confirmed right-sided pulmonary emboli. Incidentally, an 8 cm lesion was identified in the dome of the liver. It demonstrated irregular peripheral enhancement, central hypodensity, and calcifications, raising strong suspicion for primary or secondary malignancy (Figure 2).
CTPA image showing hepatic lesionCTPA: Computed tomography pulmonary angiographyThere is a large hepatic dome lesion (white arrow) measuring about 8 cm in diameter, showing peripheral irregular enhancement with central hypodensity. There are multiple flecks of calcifications within the lesion.
A dedicated triple-phase computed tomography of the liver confirmed the lesion, showed two small simple hepatic cysts, but revealed no lymphadenopathy or extrahepatic disease (Figure 3).
CTPA image showing extent of lesionCTPA: Computed tomography pulmonary angiographyBilateral hepatic cysts, measuring 12 mm on the right, with a left interpolar one at 2 cm.
Differential diagnosis
The differential diagnosis included intrahepatic cholangiocarcinoma, hepatocellular carcinoma, metastatic deposits, and sclerosed haemangioma.
Management and clinical course
The patient was treated for acute heart failure and atrial fibrillation with intravenous furosemide, bisoprolol, and digoxin. Anticoagulation with apixaban was initiated for pulmonary embolism. Given the suspicious hepatic lesion, the case was reviewed by both the upper gastrointestinal and hepatobiliary multidisciplinary teams. A percutaneous liver biopsy was performed. Histology demonstrated dense fibrous hyalinised stroma with collapsed vascular channels lined by bland endothelial cells, with no atypia or malignancy. The diagnosis of sclerosed haemangioma was made (Figure 4).
Ultrasound-guided hepatic biopsy imagesThis is an image captured during the ultrasound-guided biopsy process, showing the needle (white arrows) used in an intercostal approach.
Despite this, persistent radiological suspicion as well as a "technically difficult" first biopsy prompted a repeat biopsy at a tertiary centre, which confirmed the same benign pathology. The patient remained asymptomatic from a hepatic perspective, with improved weight and appetite, and was managed conservatively with imaging surveillance.
Discussion
Sclerosed haemangiomas represent a rare but important diagnostic pitfall. In contrast to cavernous haemangiomas, which demonstrate the classic pattern of peripheral nodular enhancement and centripetal fill-in, sclerosed haemangiomas often lack these features. Instead, they present with irregular peripheral enhancement, capsular retraction, and calcification, which mimic malignant lesions [2-4].
Several published case reports and reviews highlight that misdiagnosis is a common occurrence. Lai et al. reported multiple cases where sclerosed haemangiomas were mistaken for intrahepatic cholangiocarcinoma, leading to unnecessary resections [5]. Tanaka et al. described a series in which up to 30% of patients undergoing hepatic resection for presumed malignancy were ultimately diagnosed with benign sclerosed haemangiomas [6]. Our case parallels these findings but adds further complexity given the patient’s acute cardiopulmonary comorbidities and the risks of biopsy under anticoagulation.
Histopathology remains the definitive diagnostic tool. Characteristic findings include fibrous stroma, hyalinisation, and collapsed vascular channels lined by endothelial cells without atypia. In equivocal cases, repeat biopsy may be warranted to ensure diagnostic certainty and avoid resection of benign lesions. Our patient’s case underscores three key points. First, imaging alone cannot reliably distinguish sclerosed haemangiomas from malignancy. Second, in elderly patients with significant comorbidities, histological confirmation is critical to prevent unnecessary major hepatic surgery. Third, a multidisciplinary review was vital in balancing the competing risks of anticoagulation, biopsy, and surgical candidacy.
Conclusions
Sclerosed hepatic haemangiomas are rare benign lesions that frequently mimic hepatic malignancies on imaging. Misdiagnosis can lead to unnecessary hepatic resections. Histological confirmation is essential, particularly in elderly or comorbid patients, where surgery carries a significant risk. This case demonstrates how a multidisciplinary approach, incorporating careful biopsy and repeat histological confirmation, enabled an accurate diagnosis and safe conservative management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The diagnosis and management of benign hepatic tumors J Clin Gastroenterol Choi BY Nguyen MH 4014123920051581520910.1097/01.mcg.0000159226.63037.a 2 · doi ↗ · pubmed ↗
- 2Imaging features of sclerosed hemangioma AJR Am J Roentgenol Doyle DJ Khalili K Guindi M Atri M 677218920071757915410.2214/AJR.06.1076 · doi ↗ · pubmed ↗
- 3Clinical case report: sclerosing hemangioma of the liver, a rare but great mimicker Radiol Case Rep Behbahani S Hoffmann JC Stonebridge R Mahboob S 58611120162725745010.1016/j.radcr.2016.02.015PMC 4878953 · doi ↗ · pubmed ↗
- 4Sclerosed hemangioma of the liver: a diagnostic challenge BMJ Case Rep Yamada N Miyake K Takahashi H 247902152022
- 5Case report: Sclerosed hemangioma of the liver: A diagnostic challenge Front Surg Poras M Katsanos G Agrafiotis AC Demetter P Pezzullo M Lucidi V 985849920223664452810.3389/fsurg.2022.985849 PMC 9834279 · doi ↗ · pubmed ↗
- 6Sclerosed hemangioma of the liver: report of a case and review of the literature Hepatol Res Mori H Ikegami T Imura S 5295333820081806755710.1111/j.1872-034X.2007.00306.x · doi ↗ · pubmed ↗