Unmasking the Great Mimic: An Atypical Presentation of Giant Cell Arteritis With Recurrent and Isolated Diplopia
George Pandarakalam Thomas, Joyita Barua, Ahmet Ubur, Paul Bolaji

TL;DR
A rare case of giant cell arteritis (GCA) presented with only recurring diplopia, highlighting the condition's ability to mimic other disorders and the importance of early detection.
Contribution
This case report highlights the atypical presentation of GCA with isolated diplopia, expanding clinical awareness of its non-classical manifestations.
Findings
GCA was diagnosed in a patient with isolated, recurrent diplopia and no classical symptoms.
High-dose corticosteroid treatment resolved diplopia and normalized inflammatory markers.
The case suggests intracranial vasculitis or ophthalmic artery ischemia as possible mechanisms for diplopia in GCA.
Abstract
Giant cell arteritis (GCA) is a well-recognized vasculitis, typically presenting with headaches, scalp tenderness, jaw claudication, polymyalgia rheumatica, or constitutional symptoms. In stroke and transient ischemic attack (TIA) clinics, GCA is primarily considered in cases of visual loss due to ophthalmic artery involvement. However, diplopia as an isolated manifestation of GCA is exceedingly rare, making early recognition challenging. We present the case of a 75-year-old man who attended our TIA clinic with seven recurrent episodes of transient binocular diplopia. Notably, he lacked the classical features of GCA, including headache, scalp tenderness, jaw claudication, or visual loss. There was no history of fever, night sweats, weight loss, or other systemic symptoms. His neurological examination was unremarkable, and he denied any recent trauma or medication changes. However,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
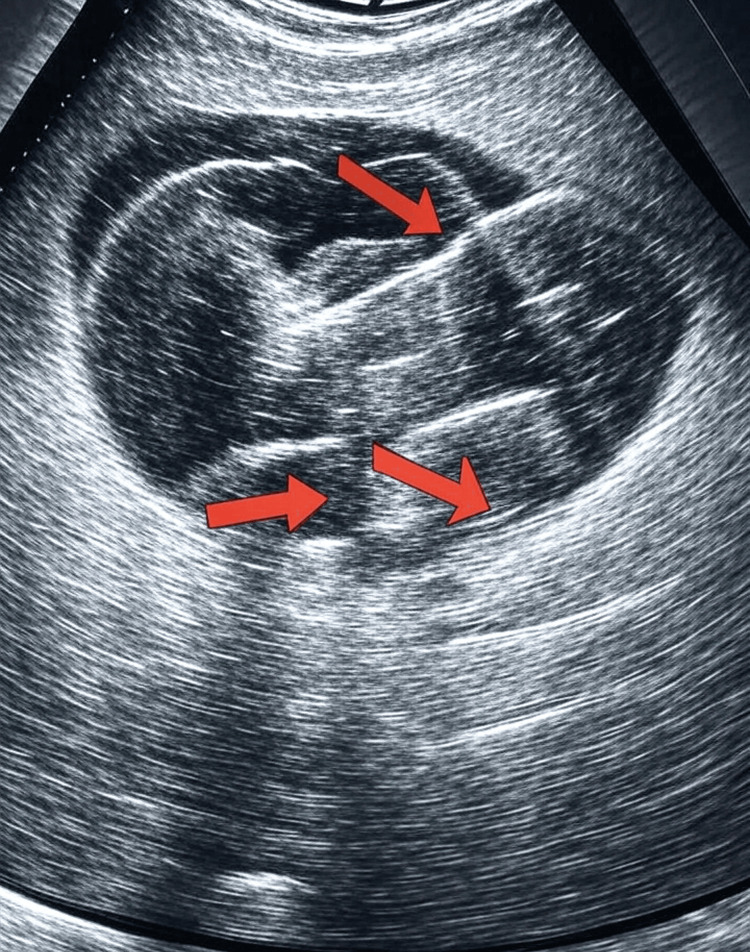 Figure 1
Figure 1| Investigation | Reference range | On presentation | After one month of treatment |
| Hemoglobin | 130-170 g/L | 150 g/L | 123 g/L |
| White cell count | 4-10 × 10⁹/L | 7 × 10⁹/L | 7.9 × 10⁹/L |
| Platelets | 150-410 × 10⁹/L | 182 × 10⁹/L | 383 × 10⁹/L |
| ESR | 1-30 mm/h | 58 mm/h | 1 mm/h |
| CRP | 0-5 mg/L | 77 mg/L | 1 mg/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Otitis Media and Relapsing Polychondritis · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Introduction
Giant cell arteritis (GCA) is a chronic, inflammatory condition primarily affecting medium and large arteries, characterized by granulomatous inflammation and infiltration of arterial walls, which can lead to luminal narrowing and ischemic complications, including permanent visual loss if untreated [1]. It is a critical medical emergency in ophthalmology due to its potential to cause preventable visual loss if diagnosed and treated promptly. GCA is the most common vasculitis in individuals aged 50 years and older, and it does not typically occur in those under 50 years of age. It has a higher prevalence in females, with a female-to-male ratio ranging from 1.4:1 to 2.9:1 [1]. Common symptoms include severe physical and mental fatigue, proximal upper extremity muscle pain, headaches, scalp tenderness, visual loss, and jaw claudication. However, diagnosis is often delayed for several months due to the gradual or insidious onset of symptoms, which can complicate timely intervention [2].
Two forms of GCA are recognized: a cranial form involving the medium-caliber temporal artery, causing temporal arteritis, and an extracranial form affecting large vessels, primarily the thoracic aorta and its branches, including the vertebrobasilar system supplying the midbrain and pons [2]. The variability in affected arteries leads to atypical presentations in some patients, lacking classical features such as headache or temporal artery tenderness [3]. Previous case reports have documented rare presentations, such as transient diplopia without classical symptoms, highlighting the need for heightened clinical suspicion to prevent severe outcomes like permanent visual loss or stroke [4,5]. If untreated, GCA can progress to irreversible ischemic complications, underscoring the urgency of early diagnosis and management.
Standard treatment involves high-dose corticosteroids, typically prednisolone at 1 mg/kg, to rapidly control inflammation and prevent progression to visual loss or other ischemic events [6]. More recently, IL-6 inhibitors, such as tocilizumab, have been introduced as steroid-sparing agents to reduce corticosteroid-related adverse effects and improve long-term outcomes [7]. This case report aims to elucidate a rare clinical presentation of GCA to enhance clinicians’ understanding and support the development of definitive management guidelines.
This article was previously presented as a meeting abstract at the BAPIO YDF Conference in Bristol on May 10, 2025.
Case presentation
A 75-year-old man presented to the emergency department following seven episodes of transient binocular diplopia over one month, each lasting approximately 10-15 minutes. He described seeing images side by side but denied headaches, scalp tenderness, jaw or tongue claudication, visual loss, polymyalgia rheumatica symptoms, or other ischemic symptoms suggestive of a transient ischemic attack (TIA) or stroke. He reported no fever, night sweats, weight loss, recent trauma, new medication use, palpitations, sweating, or diarrhea. He denied ptosis, and the diplopia was not time-dependent. The patient had no significant past medical history, including no history of migraines (with or without aura), atrial fibrillation, antiphospholipid antibody syndrome (APS), systemic lupus erythematosus (SLE), or hematologic disorders such as thrombocytosis or polycythemia. He was not on any regular medications and had no known allergies.
On examination, visual field tests and pursuit eye movements were normal, with no nystagmus or diplopia noted during eye movements. Motor, sensory, coordination, and cranial nerve examinations were unremarkable, and no pathological reflexes were elicited. Auscultation of the heart and major blood vessels, as well as the ECG, yielded normal findings.
Laboratory tests revealed elevated inflammatory markers, as shown in Table 1, including a CRP of 77 mg/L and an erythrocyte sedimentation rate (ESR) of 58 mm/h. Platelet count and WBC count were within normal limits. MRI and CT of the head showed no acute hemorrhage or stroke but noted an incidental arachnoid cyst in the left temporal region. Based on these findings, TIA or infection was deemed unlikely, and GCA was suspected, prompting urgent referral to the ophthalmology and rheumatology departments. Key differentials considered included migrainous auras or ophthalmoplegic/acephalgic brainstem migraines (which can cause transient diplopia without headache), embolic events from intermittent atrial fibrillation or thrombotic disorders (e.g., APS or SLE), and other vasculitides. Similar previous reports have described transient diplopia as a rare initial presentation of GCA due to ischemic involvement of cranial nerves or brainstem vessels, often resolving with treatment but risking progression to visual loss [8,9]. GCA’s pathology involves granulomatous inflammation of arterial walls, leading to occlusion and ischemia; if untreated, it can result in permanent blindness or stroke, emphasizing the need for prompt recognition.
The rheumatology department performed an urgent temporal artery ultrasound the following day. The ultrasound findings are detailed in Figure 1, showing increased intima-media thickness and reduced compressibility in the superficial temporal, frontal, and axillary arteries of both sides, corresponding to the “halo sign” (a hypoechoic rim around the artery lumen indicative of inflammation) and the “compressibility sign” (reduced arterial compressibility due to wall thickening). These findings confirm the diagnosis of GCA. No significant stenosis was observed in the ultrasound, and as the patient did not undergo a temporal artery biopsy, no data on skipped lesions are unfortunately available. The patient was started on high-dose prednisolone (80 mg, 1 mg/kg) with a planned 16.5-month tapering regimen. A CT of the chest, abdomen, and pelvis and a CT aortogram showed no involvement of other major vessels.
Temporal artery ultrasound showing increased intima-media thickness in the superficial temporal arteryThe red arrows indicate areas of thickened intima media, consistent with GCA.GCA, giant cell arteritis
The ophthalmology team found no evidence of relative afferent pupillary defect. Fundoscopy revealed normal optic nerve discs bilaterally and normal visual fields. A follow-up ophthalmology review one month later showed no significant ocular findings.
Discussion
This case report describes a patient with recurrent transient diplopia diagnosed with GCA based on positive ultrasound findings, as detailed in Figure 1. Diplopia may result from intraocular or neuromuscular causes, cerebrovascular accidents, or cranial nerve palsies [4]. Ischemia of the extraocular muscles or their blood supply may contribute to diplopia [5]. The ultrasound findings, showing bilateral increased intima-media thickness and reduced compressibility in the superficial temporal, frontal, and axillary arteries, correspond to the “halo sign” (a hypoechoic rim around the artery lumen indicative of inflammatory edema) and the “compressibility sign” (reduced arterial wall elasticity due to thickening), suggesting ischemia-driven arterial wall narrowing due to granulomatous inflammation, a hallmark of GCA. Clinical examinations and investigations are critical for diagnosis and treatment in such cases, with diplopia serving as a warning sign to investigate vascular causes of ocular manifestations.
Age is a significant factor in older adults with transient ocular symptoms, particularly when risk factors like hypertension or diabetes suggest ischemic causes [6]. This patient had a history of hypertension, which heightened suspicion for GCA as a differential diagnosis. Tamhankar et al. emphasized the importance of thorough history-taking to identify GCA symptoms such as jaw pain or headache, yet this patient lacked these features, underscoring the challenge of atypical presentations [6]. His referral to the stroke clinic for suspected TIA highlights how GCA’s atypical presentations can be mistaken for other conditions.
Historically, CRP and ESR have been key inflammatory markers in GCA diagnosis, with CRP being more sensitive and the combination of both offering high specificity [7,8]. Hayreh et al. noted a significant association between these markers and jaw claudication, which was absent in this case [7]. Additionally, Oh et al. reported thrombocytosis in GCA, though this patient’s platelet count was normal [9]. The elevated CRP (77 mg/L) and ESR (58 mm/h), as shown in Table 1, supported the GCA diagnosis despite the absence of classical symptoms, suggesting a need for further studies on the relationship between inflammatory markers and diplopia.
Temporal artery biopsy is the gold standard for GCA diagnosis but is now less favored due to complications such as insufficient sample size and invasiveness [10]. Ultrasound has become the preferred initial diagnostic modality, with Moiseev et al. advocating that clinical suspicion combined with positive ultrasound findings is sufficient for diagnosis [11]. The ultrasound findings in Figure 1 confirmed arterial wall thickening, enabling early diagnosis and treatment, while a CT aortogram showed no involvement of other major vessels. A digital subtraction angiogram could be considered to further assess vascular patency but was not pursued given the diagnostic clarity from ultrasound and the patient’s stable condition.
Permanent or transient diplopia is a rare GCA presentation and may precede visual loss [12]. Similar reports have documented transient diplopia as an early ischemic manifestation of GCA, often resolving with treatment but with a risk of progression to visual loss if untreated [8,9,12]. Early corticosteroid treatment has been shown to resolve ocular symptoms and prevent progression to visual loss [5,13]. The patient reported no adverse effects from the corticosteroid treatment, and therefore, no such effects were included in the report. This patient’s diplopia resolved following high-dose prednisolone (1 mg/kg) with a 16.5-month tapering regimen, with no recurrence at three- and six-month follow-ups. Differentials for diplopia in this case included migrainous auras or ophthalmoplegic/acephalgic brainstem migraines, embolic events from atrial fibrillation or thrombotic disorders (e.g., APS or SLE), cerebrovascular accidents, cranial nerve palsies, and other vasculitides, all of which were ruled out through clinical and blood investigations and imaging findings. Continued monitoring will provide insights into the long-term effects of treatment.
Conclusions
This case underscores the importance of recognizing transient diplopia as a rare presentation of GCA, particularly in the absence of classical symptoms. This case’s uniformity lies in its consistency with documented atypical presentations and diagnostic approaches for GCA, while its rarity highlights the importance of considering GCA in patients with transient diplopia. The conclusions are supported by the data, including the patient’s resolution of symptoms following treatment, normalization of elevated inflammatory markers after therapy, and ultrasound findings consistent with bilateral arterial wall changes. Early diagnosis and treatment with corticosteroids can prevent irreversible complications and promote recovery. Clinicians should consider GCA as a differential diagnosis in older adults with systemic or ocular symptoms, supported by routine inflammatory marker testing and ultrasound imaging.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The incidence of giant cell arteritis in Jerusalem over a 25-year period: annual and seasonal fluctuations Clin Exp Rheumatol Bas-Lando M Breuer GS Berkun Y Mates M Sonnenblick M Nesher G 07252007 https://pubmed.ncbi.nlm.nih.gov/17428357/17428357 · pubmed ↗
- 2Giant cell arteritis: advances in understanding pathogenesis and implications for clinical practice Cells Paroli M Caccavale R Accapezzato D 2671320243833465910.3390/cells 13030267 PMC 10855045 · doi ↗ · pubmed ↗
- 3Giant cell arteritis: 2018 review Mo Med Winkler A True D 4684701152018 https://pubmed.ncbi.nlm.nih.gov/30385998/30385998 PMC 6205276 · pubmed ↗
- 4Retrospective, multicenter comparison of the clinical presentation of patients presenting with diplopia from giant cell arteritis vs other causes J Neuroophthalmol Ross AG Jivraj I Rodriguez G 8133920192969744110.1097/WNO.0000000000000656 · doi ↗ · pubmed ↗
- 5Diplopia as the presenting symptom in giant cell arteritis Can J Optom Nealon C Canania R 842022
- 6Isolated third, fourth, and sixth cranial nerve palsies from presumed microvascular versus other causes: a prospective study Ophthalmology Tamhankar MA Biousse V Ying GS 2264226912020132374716310.1016/j.ophtha.2013.04.009PMC 3795864 · doi ↗ · pubmed ↗
- 7Giant cell arteritis: validity and reliability of various diagnostic criteria Am J Ophthalmol Hayreh SS Podhajsky PA Raman R Zimmerman B 2852961231997906323710.1016/s 0002-9394(14)70123-0 · doi ↗ · pubmed ↗
- 8Prevalence of a normal C-reactive protein with an elevated erythrocyte sedimentation rate in biopsy-proven giant cell arteritis Ophthalmology Parikh M Miller NR Lee AG 1842184511320061688477810.1016/j.ophtha.2006.05.020 · doi ↗ · pubmed ↗