Human connective tissue - 3D datasets to characterise the material properties
Heiko Stark, Julian Sartori

TL;DR
This paper uses 3D datasets from body donors to study the distribution and material properties of human connective tissue.
Contribution
The study introduces a method to segment and analyze collagen structures in human connective tissue using computational image processing.
Findings
The thigh has the highest percentage of fibrous components in the human body.
Image processing revealed local collagen orientation in tissues.
Individual fascicles and subtendons can be resolved when isolated but not in compact regions.
Abstract
These datasets were aimed at measuring the distribution of human connective tissue and characterising the material properties. We, therefore, used the existing datasets of male and female body donors from the Visible Human Project (VHP). In the first step, collagen-containing structures were segmented and reconstructed using digital image processing. In addition, several properties (i.e. thickness, orientation) were characterised and analysed using computational methods. The percentage of fibrous components within the whole body was highest in the thigh. The results of the image processing provided local collagen orientation within the tissues. They showed that individual fascicles and subtendons can be resolved when isolated, but not within compact regions of connective tissues.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
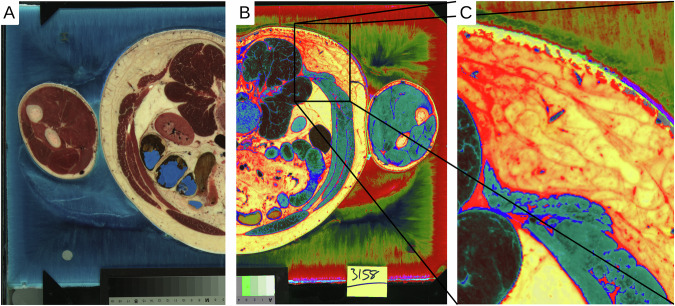 Figure 1
Figure 1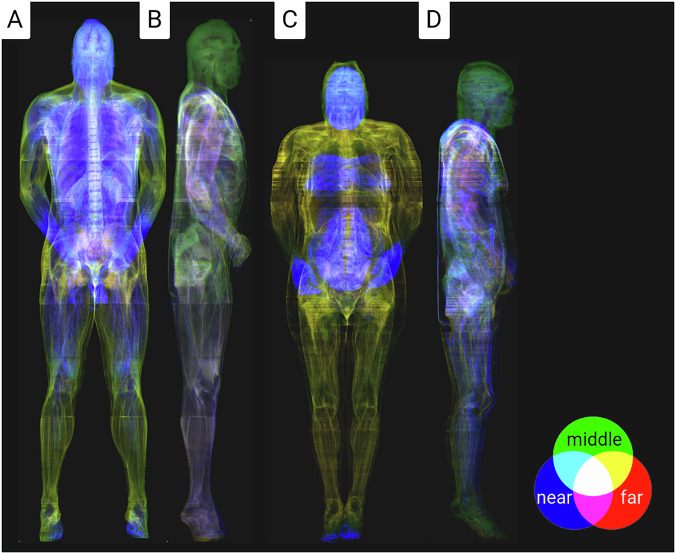 Figure 2
Figure 2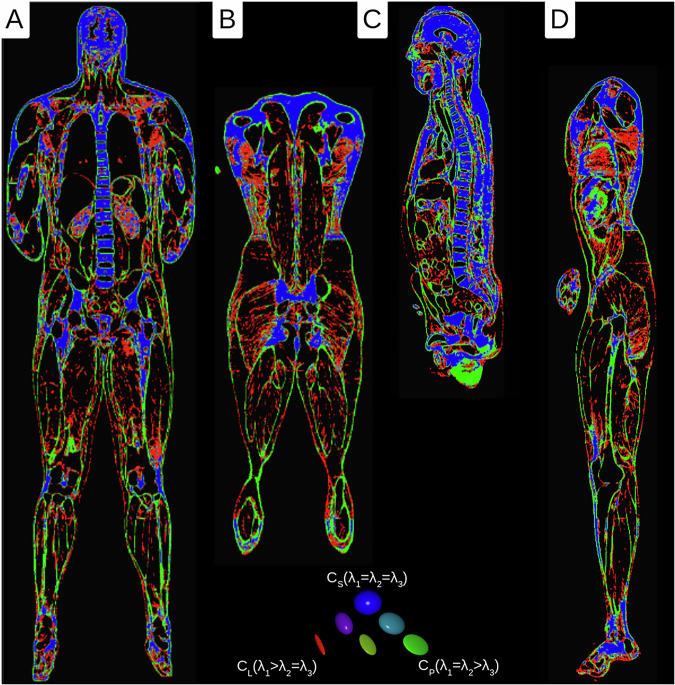 Figure 3
Figure 3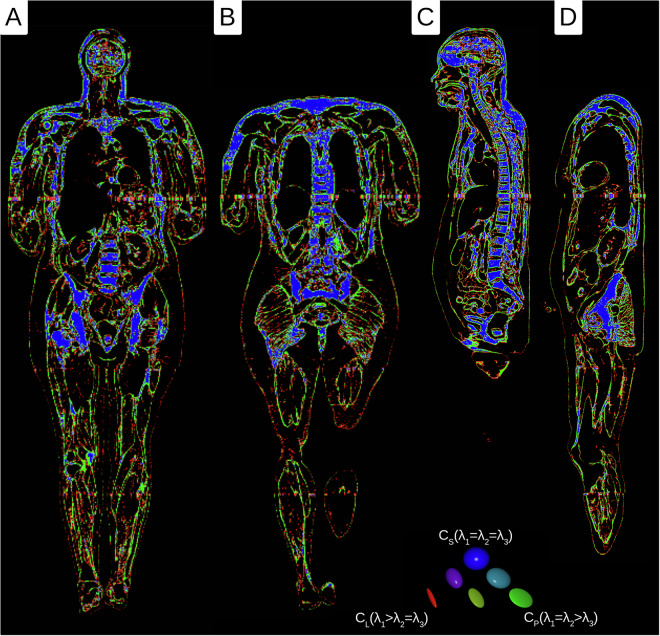 Figure 4
Figure 4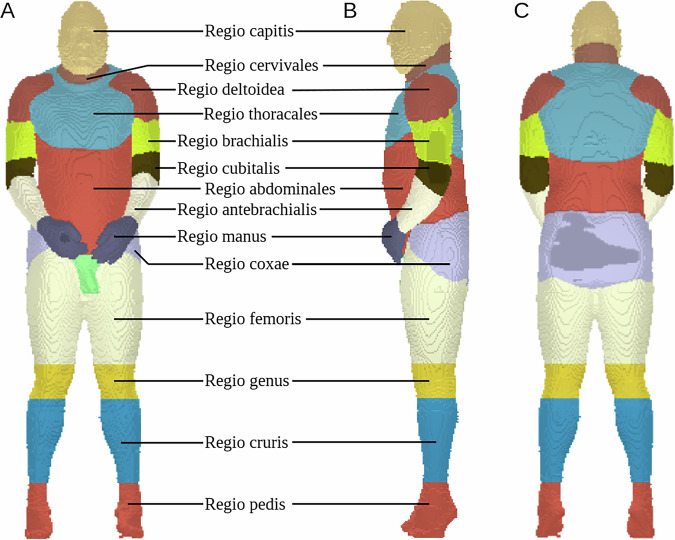 Figure 5
Figure 5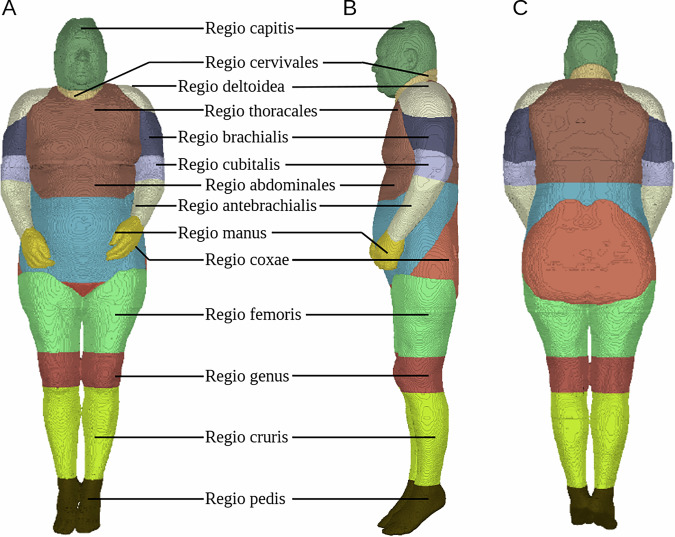 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnatomy and Medical Technology · Breast Implant and Reconstruction · 3D Shape Modeling and Analysis
Background & Summary
Surprisingly, humans consist of 60 to 65% water and still have a stable form. Connective tissue, which holds individual cells, organs, and body parts together, plays a unique role here^1–3^. It contributes a significant proportion of protein mass in the body (primary component collagen, 25 to 35%)^4^. Most of the water in the body is present in liquid form or with a higher viscosity (e.g., through hyaluronic acid). In order to stabilise the body, it is organised into compartments. The smallest compartments are located at the cellular level and ensure the integrity of individual cells through the extracellular matrix (ECM). In addition, connective tissue forms unique substructures and compartments for organs (muscles, brain, intestines, etc.) and connects them. The skin is the largest structure that ultimately separates us from the environment.
Collagen forms the ECM of many tissues, often together with other structural proteins such as elastin or biominerals such as bone apatite. Due to this composite character of the ECM, it is essential to know its composition and the distribution and orientation of the components^5,6^. The analogy of reinforced concrete emphasises this necessity. Here, a pressure-resistant and tension-resistant material were combined, resulting in a new material with both properties. As with steel in reinforced concrete, the orientation of the collagen fibres leads to anisotropy of the tissue and is therefore essential for its biomechanical characterisation^7^. The collagen orientation mainly develops during ontogenesis and is determined by the principal direction of stress^8,9^. This is important because it is challenging to recreate a comparable structure, for example, if it has been injured or was separated in surgery^10^. This must be taken into account in simulations that investigate surgical changes. The stiffness can differ significantly in the fibre direction from that in the directions orthogonal to the fibres^11,12^.
In the datasets presented here, the connective tissue could be reconstructed in all organs. In addition, material structure was characterised and analysed using image processing methods. The datasets obtained in this way can serve as a basis for simulations and as an overview map for studies investigating details of the connective tissue structure. These can include simulations of the musculature and the bone apparatus. For example, it is known that when a muscle contracts, it not only actively shortens but also transmits lateral forces^13,14^. This is shown by bulging the biceps brachii muscle during a contraction. Connective tissue structures largely transmit these lateral forces and must be taken into consideration. However, a detailed description is also necessary for structures with a high proportion of connective tissue. For the knee, for example, Dhaher et al. showed that integrating connective tissue into a model can reveal new biomechanical interactions^15^.
Aim
The aim of these datasets was to measure the distribution of human connective tissue and to characterise the material properties. However, its primary purpose was to create a database to extend existing and future biomechanical models.
Methods
Visible Human Project (VHP)
For this study, we used the existing datasets of a male and female body donor (♂:39 years, 90.26 kg, 1.88 m; ♀:59 years, 88 kg, 1.71 m) from the Visible Human Project® (VHP)^16,17^. The datasets were digitised RGB colour images of cryo-sections with a resolution of 0.144 × 0.144 mm^2^ and a cutting thickness of ♂:1 mm and ♀:0.33 mm^18–20^. Body donors were shock-frozen to prepare the cryo-sectioning and divided into four craniocaudal blocks. The blocks were then removed layer by layer, and the surface was photographed (Fig. 1A). As a result of the quartering, some cross-sections were missing or only contained fragments. This was corrected in a later step.Fig. 1A) Cross-section from the original datasets of the Visible Human Project at the level of L3. (B) The digitally processed image is based on the RGB information of the connective tissue. (C) Closer view from B.
To use the images from the VHP, the cross-sections first had to be correctly aligned with each other. This was done automatically and manually refined using the software ‘Imaris’ (Oxford Instruments, UK). In addition, the aligned images were cleaned of artefacts using the software ‘Imagexd’ (Heiko Stark, Jena, Germany), and the missing cross-sections between the blocks were filled by interpolation.
Image stacks
In the second step, collagen-containing structures were segmented and reconstructed using digital image processing. The approach utilised the fact that collagen-containing connective tissue had unique colour values in the RGB colour space, which could be extracted through a transformation of the colouring (Fig. 1B). Furthermore, the colours of connective tissue surrounding the organs and connective tissue embedded in subcutaneous fatty tissue were slightly different (Fig. 1C). These values were segmented and further processed to create a topographic model using the software ‘Imagexd’ (Fig. 2A–D). Several spectral colours could be considered in the future, which would probably allow an even finer segmentation.Fig. 2. Coloured X-ray visualisation of the connective tissue for the male and female body donor. The colours reflect the depth information of the local connective tissue portions, whereby overlapping colours are averaged.
Scalar field - density & thickness calculation
Connective tissue thickness is crucial in several issues, for example, in determining tissue properties in indentation tests, and in estimating the thickness of fascia (e.g., Fascia renalis) or capsule (e.g., Capsula fibrosa). Based on the data, the thickness of the connective tissue structures was further calculated using the software ‘Imagexd’. First, the image stacks were converted by summing or interpolating voxels into isometric voxels (♂:0.5 × 0.5 × 0.5 mm^3^; ♀:0.33 × 0.33 × 0.33 mm^3^) to simplify the thickness determination. Then, all orientation directions around each voxel with connective tissue content within a 64 voxel range were examined, and the direction with the minimum thickness was determined. These minimum thickness data were stored in a three-dimensional stack and statistically analysed (Table 1).Table 1. Statistics of the thickness measurement for selected body regions of the male and female body donors.RegioMaleFemaleMeanSDMeanSDcapitis5.58 mm3.63 mm2.64 mm2.12 mmcervivales5.04 mm3.66 mm3.09 mm2.49 mmthoracales3.92 mm3.51 mm2.48 mm2.56 mmabdominales2.38 mm2.21 mm1.83 mm1.64 mmperinealis3.83 mm3.21 mm2.02 mm1.71 mmdeltoidea****5.90 mm4.18 mm2.36 mm1.76 mmbrachialis3.68 mm3.10 mm1.89 mm1.60 mmcubitalis****3.52 mm2.60 mm2.66 mm3.06 mmantebrachialis2.92 mm2.41 mm1.27 mm1.00 mmmanus****3.01 mm2.39 mm1.62 mm1.39 mmcoxae****3.71 mm4.03 mm1.78 mm1.63 mmfemoris1.70 mm1.81 mm1.60 mm1.59 mmgenus****2.67 mm2.49 mm1.37 mm1.16 mmcruris2.18 mm1.77 mm1.23 mm1.02 mmpedis****2.77 mm2.18 mm1.17 mm0.91 mmThe mean values of the joint regions in the extremities are highlighted in bold.
Tensor field - orientation calculation
To obtain statistical data on the morphological anisotropy of the material, we used a technique that was previously developed for the determination of the orientations of fascicles. This was originally developed for a muscular study but generally applies to all fibrous structures^21,22^. This technique was modified and applied to the existing isometric voxel dataset using ‘Imagexd’. It takes advantage of the fact that local orientation tensors can be calculated from the spatial density distribution. This is a mathematical description of the local orientation expressed in a symmetrical 3 × 3 matrix. The same method was used by Kupczik et al. (2015) and Dickinson et al. (2018) to determine the local vector from the number of possible orientation directions X^21,22^. In the modified method, the local vectors xi were additionally summarised using the dyadic product in the respective matrix A:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$A=\mathop{\sum }\limits_{i=1}^{\left|x\right|}{x}_{i}\otimes {x}_{i}$$\end{document}This matrix could be used to determine the three main directional axes (eigenvectors) and their anisotropy strength (eigenvalues). The eigenvalues characterise the tissue components in terms of their structure (Table 2). There was only one strongest eigenvector for the fibrous parts and two strong eigenvectors for the planar parts. If all three eigenvectors were equally strong, the structures were classified as a spatially homogeneous collection of connective tissue. This classification could also be colour-coded using the Westin measures cl, cp, and cs (Figs. 3 and 4)^23,24^. This workflow was applied to all voxels with connective tissue. As a result of a scan range of 16 voxels, in each voxel the same number of orientations was taken as a basis.Table 2. Statistics on the distribution of the structural proportions for the connective tissue volume of selected body regions of the male and female body donors.RegioMaleFemaleVolumeFibrousPlanarSphericalVolumeFibrousPlanarSphericalcapitis4.65 dm^3^15.49 %21.43 %**50.95 %**4.93 dm^3^19.81 %26.03 %31.85 %****cervivales0.79 dm^3^10.63 %18.86 %**28.77 %**0.51 dm^3^14.11 %19.51 %25.94 %****thoracales16.50 dm^3^18.03 %17.20 %**26.50 %**25.10 dm^3^10.78 %**13.25 %**12.88 %abdominales21.41 dm^3^16.80 %**17.76 %**12.28 %18.59 dm^3^10.14 %**11.62 %**9.82 %perinealis0.53 dm^3^16.43 %24.48 %**26.57 %**0.36 dm^3^10.03 %**11.18 %**10.34 %deltoidea3.38 dm^3^9.72 %15.69 %**29.89 %**1.83 dm^3^16.14 %23.84 %26.92 %****brachialis3.57 dm^3^10.22 %**17.78 %**17.49 %2.80 dm^3^11.68 %**13.73 %**8.96 %cubitalis1.74 dm^3^14.46 %**20.98 %**18.83 %1.67 dm^3^**15.90 %**14.85 %9.16 %antebrachialis2.26 dm^3^17.32 %**22.80 %**15.85 %2.11 dm^3^**8.60 %**8.47 %3.00 %manus1.24 dm^3^**22.70 %****23.02 %**21.27 %0.93 dm^3^**12.48 %**11.63 %7.11 %coxae12.87 dm^3^**17.82 %**15.99 %16.23 %9.56 dm^3^10.56 %**11.73 %**11.47 %femoris18.98 dm^3^**12.66 %**10.47 %2.96 %13.00 dm^3^**8.02 %**7.82 %4.78 %genus3.40 dm^3^13.76 %**16.47 %**9.59 %3.57 dm^3^7.94 %**8.66 %**3.46 %cruris5.63 dm^3^12.17 %**16.24 %**5.86 %5.53 dm^3^**9.02 %**8.62 %2.88 %pedis2.67 dm^3^**23.06 %****22.82 %**19.47 %1.92 dm^3^**11.25 %**9.51 %4.46 %The highest structural proportions are highlighted in bold.Fig. 3. Westin plots of the tensor data of the male body donor (red = fibrous, green = planar, and blue = spherical parts). (A) medial frontal section (B) dorsal frontal section (C) sagittal section (D) parasagittal section.Fig. 4. Westin plots of the tensor data of the female body donor (red = fibrous, green = planar, and blue = spherical parts). (A) medial frontal section (B) dorsal frontal section (C) sagittal section (D) parasagittal section.
Data Records
All the following datasets were generated using the original datasets from the VHP (see Methods)^16,17^. It is given as a filename in compressed NIFTY format (Neuroimaging Informatics Technology Initiative), which can be downloaded from Mendeley Data^25,26^.
- Male - Mendeley Data: 10.17632/zc53h3dcfg.1
- Female - Mendeley Data: 10.17632/7m9z78jpgs.1
The respective dataset dimensions, data types and resolutions are specified in brackets.
Connective tissue
The segmented datasets for the male and female body donors, taking into account the connective tissue (Fig. 2), consist of the original resolution and reduced bit depth (male & female). Isometric voxel data were created from these datasets by summative binning (male-iso & female-iso). For a quick overview, additional millimetre resolution datasets were calculated from isometric voxel data by summative binning (male-small & female-small).
- male.nii.gz (3753 × 2141 × 1867 unit 8 - 0.144 × 0.144 × 1 mm^3^)
- male-iso.nii.gz (1081 × 617 × 3734 unit 16 - 0.5 × 0.5 × 0.5 mm^3^)
- male-small.nii.gz (540 × 308 × 1867 unit 16 - 1 × 1* × *1 mm^3^)
- female.nii.gz (4096 × 3061 × 5190 unit 8 - 0.144 × 0.144 × 0.33 mm^3^)
- female-iso.nii.gz (1787 × 1336 × 5190 unit 16 - 0.33 × 0.33 × 0.33 mm^3^)
- female-small.nii.gz (590 × 441 × 1713 unit 16 - 1 × 1 × 1 mm^3^)
Body regions
To categorise the available data concerning their distribution in the body, an anatomical classification was used^27^. For this purpose, a mask dataset was created with 3D Slicer (Brigham and Women’s Hospital (BWH), USA)^28^ for both men and women, and individual body regions were assigned (Figs. 5 and 6). We do not expect a loss of accuracy from using the reduced dataset because the anatomical categorisation was carried out at a low level of detail.
- male-small.labels.nii.gz (108 × 62 × 373 unit 16 - 5 × 5 × 5 mm^3^)
- female-small.labels.nii.gz (295 × 220 × 856 unit 16 - 2 × 2 × 2 mm^3^) Fig. 5. Segmentations of the body regions for the male body donor in random colours. (A) Frontal view (B) Lateral view (C) Dorsal view.Fig. 6. Segmentations of the body regions for the female body donor in random colours. (A) Frontal view (B) Lateral view (C) Dorsal view.
Thickness measurement
The thickness measurement showed a very variable distribution of connective tissue in terms of its areal thickness in the body (Fig. 2). For the entire data set, values ranged from 0.5 to 32 mm for men and from 0.33 to 21.12 mm for women. Values outside the range can also occur, but these were neglected here due to the time required. The thickest layers of connective tissue are found in the knees, shoulders, and head (Table 1). The musculature usually shows very thin or fibrous structures (Table 1Regio femoris/cruris). It should be emphasised that the data show a shirt-like distribution of the superficial connective tissue in the thoracic region.
- male-iso.t.nii.gz (1081 × 617 × 3734 unit - 0.5 × 0.5 × 0.5 mm^3^)
- female-iso.t.nii.gz (1787 × 1336 × 5190 unit - 0.33 × 0.33 × 0.33 mm^3^)
Orientation measurement
The result of the local orientation tensors showed that the highest percentage of local orientation tensors within the fibrous parts was found in the thigh (Table 2). The planar portions predominate, except for the head, where the spherical portions predominate. It should be noted that the scan range for determining anisotropy was only 8 mm for men and 5.28 mm for women. Thus, larger structures (for example, the brain) are generally classified as spherical, although they could also be planar when viewed on a larger scale.
- male-iso.c2.nii.gz (540 × 308 × 1867 symmat - 1 × 1 × 1 mm^3^)
- male-iso.c2_e1.nii.gz (540 × 308 × 1867 rgb - 1 × 1 × 1 mm^3^)
- male-iso.c2_e2.nii.gz (540 × 308 × 1867 rgb - 1 × 1 × 1 mm^3^)
- male-iso.c2_westin.nii.gz (540 × 308 × 1867 rgb - 1 × 1 × 1 mm^3^)
- male-iso.c2_westin_rank.nii.gz (540 × 308 × 1867 rgb - 1 × 1 × 1 mm^3^)
- female-iso.c2.nii.gz (893 × 668 × 2595 symmat - 0.66 × 0.66 × 0.66 mm^3^)
- female-iso.c2_e1.nii.gz (893 × 668 × 2595 rgb - 0.66 × 0.66 × 0.66 mm^3^)
- female-iso.c2_e2.nii.gz (893 × 668 × 2595 rgb - 0.66 × 0.66 × 0.66 mm^3^)
- female-iso.c2_westin.nii.gz (893 × 668 × 2595 rgb - 0.66 × 0.66 × 0.66 mm^3^)
- female-iso.c2_westin_rank.nii.gz (893 × 668 × 2595 rgb - 0.66 × 0.66 × 0.66 mm^3^)
Technical Validation
The data for segmented connective tissues are compared to the scientific record to assess the accuracy of the data. First, we compare the Achilles tendon.
The Achilles tendon is largely visualised in the female dataset as a compact strand with little internal structure. Occasional lines of voxels not marked as connective tissue are a vague indicator of fascicle orientation. Only in the proximal tendon close to the myotendinuous junction substrands can it be identified. They fan out towards the proximal end of the tendon. The diameters of these substrands can be narrowed down to 150 μm to 450 μm so that they most probably correspond to fascicles, which have diameters of 50 μm to 400 μm in human Achilles tendon^29^. We conclude that the data resolution is high enough to render individual fascicles and subtendons when isolated. Within the compact regions of the tendon, the thickness of the endotendineum between the fascicles is probably below the dataset resolution. Additionally, fascicles and endotendineum are both collagenous, so that they could have been rendered with insufficient contrast for a distinction. The single fibres (diameters of 10 μm to 50 μm) are below the resolution of the dataset. Tensor analysis renders the Achilles tendon as a connective tissue with a three-dimensional extent. However, tendons and ligaments should be identified as unidirectional tissues^30^. Consequently, the diameter of the tendon seems to exceed the threshold for identification as a tissue of unidirectional extent. However, the fascicle orientation is not resolved with sufficient clarity to contribute to the dimensionality result. In the distal part of the Achilles tendon, the Plantaris tendon runs superficially parallel to it and is pressed against the Achilles tendon along parts of their common course^31^. The distinction of both tendons in this region is difficult. We could not judge whether both tendons run parallel or merge from our dataset.
Collagen fibres are known to be continuous from the tendon proper through the unmineralised fibrocartilage up to the depth of the mineralised fibrocartilage in the Achilles tendon insertion^32,33^. However, our dataset only shows connective tissue up to the mineralisation front. Collagen within the bone and the mineralised fibrocartilage is obscured by the methods used. At the posterior end of the Calcaneus, where the Achilles tendon is pressed against it, periosteal fibrocartilage is known to occur^34^. It is depicted by the methods used here. In conclusion, connective tissues that contain more type II collagen are also rendered^33^.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guimberteau, J. C. & Armstrong, C.Architecture of Human Living Fascia: The Extracellular Matrix and Cells Revealed Through Endoscopy (Handspring Pub Ltd, 2015).
- 2Stecco, C., Hammer, W., Vleeming, A. & De Caro, R.Functional Atlas of the Human Fascial System (Churchill Livingstone, 2015).
- 3Wilke, J., Schleip, R., Yucesoy, C. A. & Banzer, W. Not merely a protective packing organ? A review of fascia and its force transmission capacity, 10.1152/japplphysiol.00565.2017 (2018).10.1152/japplphysiol.00565.201729122963 · doi ↗ · pubmed ↗
- 4NLM Visible Human Project®. Visible-human male images. National Library of Medicinehttps://data.lhncbc.nlm.nih.gov/public/Visible-Human/Male-Images/index.html (1994).
- 5NLM Visible Human Project®. Visible-human female images. National Library of Medicinehttps://data.lhncbc.nlm.nih.gov/public/Visible-Human/Female-Images/index.html (1995).
- 6Leemans, A. Visualization of Diffusion MRI Data. In Diffusion MRI, 354–380, 10.1093/med/9780195369779.003.0021 (Oxford University Press, 2013).
- 7Stark, H. & Sartori, J. The connective tissue of a man. Mendeley Data 10.17632/zc 53h 3dcfg.1 (2025).
- 8Stark, H. & Sartori, J. The connective tissue of a woman. Mendeley Data 10.17632/7m 9z 78jpgs.1 (2025).