Confirming Rupture of Membranes with Intra-Amniotic Fluorescein Dye Test
Katherine Freedy, Sarah K. Dotters-Katz, Bobby May, Sloane Mebane, Virginia Watkins, Matthew R. Grace, Jennifer Gilner

TL;DR
This paper describes using fluorescein dye under UV light to confirm preterm rupture of membranes when traditional methods are unavailable.
Contribution
The study provides visual documentation of fluorescein dye testing as an alternative to indigo carmine for diagnosing PPROM.
Findings
Fluorescein dye emits neon green fluorescence under UV light, confirming PPROM in two patients.
Photographs of tampons under UV light show clear evidence of membrane rupture.
Fluorescein is a viable alternative when indigo carmine is unavailable.
Abstract
We describe two patients presenting with preterm loss of fluid and inconclusive evaluations requiring further assessment. Patient 1 was a 41-year-old G3P1011 at 21 6/7 weeks; Patient 2 was a 22-year-old G2P1001 at 31 5/7 weeks. In both, preterm prelabor rupture of membranes (PPROM) workups yielded mixed results, prompting intra-amniotic dye testing. Due to a national indigo carmine shortage, sodium fluorescein was used. We present photographs of tampons examined under UV light, confirming PPROM in both cases. Under ultrasound guidance, 5 cc of sodium fluorescein was injected into the amniotic cavity. Patients wore a tampon for 15 minutes while ambulating. Both provided consent for publication. On direct visualization, tampons appeared normal. Under UV light (Wood's lamp), the fluorescein emitted a bright neon green fluorescence. Both specimens demonstrated photoluminescence,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
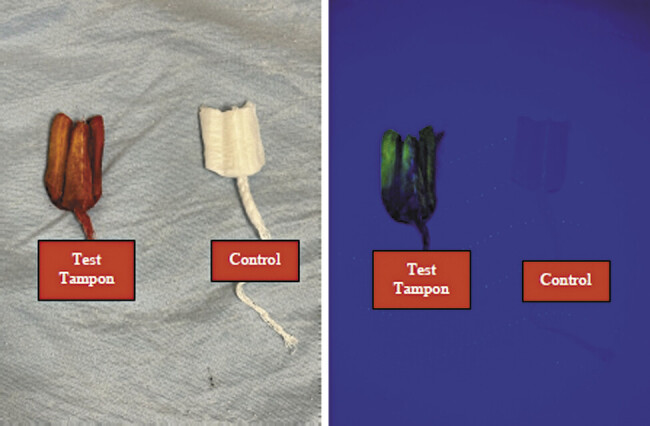 Fig. 1
Fig. 1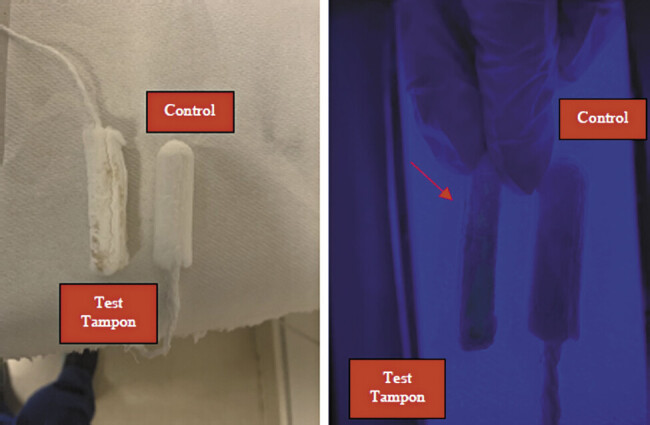 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrenatal Screening and Diagnostics · Congenital Anomalies and Fetal Surgery · Esophageal and GI Pathology
Introduction
The diagnosis of membrane rupture is typically made using nitrazine paper, visualization of fluid within the vagina or “pooling” on speculum exam, and examination of vaginal fluid for ferning under a microscope. The preterm period is arguably the most imperative time frame to confirm preterm prelabor rupture of membranes (PPROM), as it increases the risk of intra-amniotic infection (IAI), preterm labor, and neonatal sepsis. 1 2 In cases where the diagnosis is unclear based on an inconclusive work-up, the instillation of intra-amniotic dye can be used for confirmation of membrane rupture. This test is usually performed with indigo carmine, but a shortage of this drug has led to the identification of alternatives. 3 Reference images of results are lacking in those cases. 4 We present two cases of confirmed PPROM using fluorescein dye.
Patient 1
Patient 1 is a 41-year-old G3P1011 female, presented to a regional hospital at 21 ^6/7^ weeks with loss of fluid and persistent leaking. Her pregnancy was otherwise complicated by GERD, anxiety/depression, asthma, AMA, and two first-degree relatives with malignant hyperthermia. At presentation, she denied fevers, chills, contractions, or vaginal bleeding. Her vital signs were unremarkable.
Nitrazine test and amnisure were positive, so betamethasone and antibiotics were administered for PPROM, and the patient was transferred to a tertiary care facility. Upon arrival, she began experiencing vaginal bleeding. Speculum exam was notable for bright red blood with no clear source, cervix was closed, and a nonbleeding cervical polyp was observed. There was no ferning visualized on microscopic examination. Interpretation of a positive nitrazine test was confounded in the setting of bleeding. Ultrasound showed amniotic fluid pockets smaller than expected for gestational age (2.1 × 2.4 and 5.7 × 2.6 cm), but no amniotic fluid leak was confirmed. The patient was admitted for presumed PPROM, continued ampicillin and azithromycin, given a second dose of betamethasone, and given magnesium, anticipating a prolonged admission to the antepartum service. Given the discordant findings since transferring from the outside hospital and gestational age, instillation of intra-amniotic dye was recommended.
Patient 2
The patient, a 22-year-old G2P1001 female, presented to a regional hospital at 31 ^5/7^ weeks with loss of fluid without persistent leaking. Her pregnancy was otherwise complicated by a prior cesarean delivery. At presentation, she denied fevers or chills and endorsed mild lower back pain. Her vital signs were unremarkable.
Her speculum exam was negative for pooling, but microscopic examination of her vaginal swab demonstrated “copious ferning.” Nitrazine paper was unavailable. The patient was admitted with PPROM, started on ampicillin and azithromycin, given betamethasone given magnesium, and transferred to a tertiary center, anticipating a prolonged admission. On arrival, she lacked evidence of labor or intra-amniotic IAI and continued to deny any vaginal leakage. Subsequent ultrasound revealed a normal AFI of 10 cm, and an additional sterile speculum exam was negative the following day. Given discordant exams and the patient's desire to leave the hospital, the patient opted for the instillation of intra-amniotic dye.
Methods
In both cases, due to a shortage of indigo carmine, 5 cc of sodium fluorescein was injected into the amniotic cavity under ultrasound guidance. The patients were instructed to wear a tampon for 30 minutes while ambulating. The tampon appeared normal on direct visualization ( Figs. 1 and 2 ). However, under UV light, the tampon exhibited photoluminescence, confirming the presence of fluorescein and the diagnosis of PPROM ( Figs. 1 and 2 ).
Tampons by naked eye (right) and under fluorescent light (left), dye test tampon on right, unused tampon on right from patient case 1.
Tampons by naked eye (right) and under fluorescent light (left), dye test tampon on right, unused tampon on right from patient case 2.
Discussion
Patient 1
The patient remained on the antepartum service until hospital day 49, at which point she developed contractions, abdominal pain, and malaise, concerning for IAI. She underwent cesarean delivery at 28 ^6/7^ weeks and was treated with ampicillin and gentamycin. Ultimately, the patient's postpartum course was uncomplicated, and she was discharged postpartum day 3. The neonate was admitted to the intensive care nursery (ICN) and was discharged home after 67 days.
Patient 2
The patient remained on the antepartum service until hospital day 5, at which point she developed fevers and fetal tachycardia, concerning for IAI. She underwent repeat cesarean delivery and was treated for presumed endometritis due to continued fevers after delivery. Ultimately, the patient did well and was discharged postpartum day 3. The neonate was admitted to the ICN and was discharged home after 48 days.
Conclusion
In an intraamniotic indigo-carmine dye test, the tampon is visibly blue. In contrast, fluorescein requires the use of a UV light (in our case, a Wood's lamp) and displays a bright yellow appearance ( Fig. 2 ). Though the technique is well described in the literature, images of positive results are limited. These images may provide guidance in confirming PPROM diagnoses in similar cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hoffman M K Prediction and prevention of spontaneous preterm birth: ACOG practice bulletin, number 234Obstet Gynecol 20211380694594610.1097/AOG.0000000000004612 PMC 860775434794160 · doi ↗ · pubmed ↗
- 2Committee Opinion No Committee opinion no. 797: prevention of group B streptococcal early-onset disease in newborns: correction Obstet Gynecol 20201350497897910.1097/AOG.000000000000382432217968 · doi ↗ · pubmed ↗
- 3American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics Practice bulletin no. 172: premature rupture of membranes Obstet Gynecol 201612804 e 165e 17727661655 10.1097/AOG.0000000000001712 · doi ↗ · pubmed ↗
- 4Ireland K E Rodriguez E I Acosta O M Ramsey P S Intra-amniotic dye alternatives for the diagnosis of preterm prelabor rupture of membranes Obstet Gynecol 2017129061040104528486367 10.1097/AOG.0000000000002056 · doi ↗ · pubmed ↗