Trends in lifetime controlled drug use and associated risk factors among Japanese Junior High School Students: Findings from Nationwide Surveys, 2016–2024
Satomi Mizuno, Satoshi Inoura, Toshihiko Matsumoto, Kunihiko Kitagaki, Akihiro Koide, Kenji Takehara, Takuya Shimane

TL;DR
Drug use among Japanese junior high students has decreased from 2016 to 2024, but remains linked to social and behavioral risk factors.
Contribution
This study identifies specific sociodemographic and behavioral risk factors associated with controlled drug use in Japanese adolescents using nationwide survey data.
Findings
Lifetime controlled drug use prevalence dropped from 0.5% in 2016 to 0.2% in 2024.
Risk factors include male sex, alcohol use, permissive attitudes, and poor family communication.
School dissatisfaction and social isolation significantly increase drug use likelihood.
Abstract
To examine trends in the lifetime prevalence of controlled drug use among Japanese junior high school students (aged 12–15 years) between 2016 and 2024 and to identify associated sociodemographic, behavioral, and psychosocial factors. We analyzed data from 214,011 students across four nationwide surveys. The outcome was lifetime use of controlled drugs, including marijuana, solvents, methamphetamine, and new psychoactive substances. Predictors included demographic characteristics, substance‐related behaviors and attitudes, daily routines, and social relationships. Design‐weighted logistic regression was used to estimate the prevalence and assess associated risk factors. The lifetime prevalence of controlled drug use showed a clear decreasing trend over the study period, declining from 0.5% (95% confidence interval [CI]: 0.4–0.5) in 2016 to 0.2% (95% CI: 0.1–0.2) in 2024. Similar…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
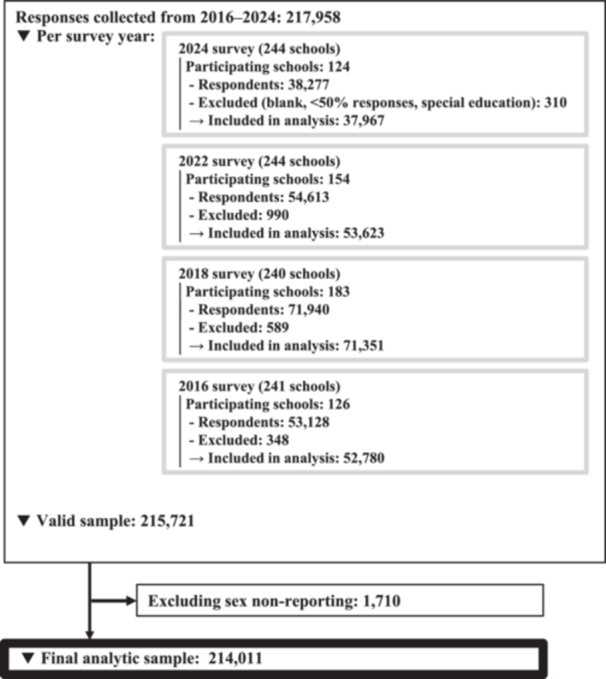 Figure 1
Figure 1| Overall | Missing value | ||
|---|---|---|---|
| Variable |
| (%) | (%) |
| Sex | 0.0 | ||
| Male | 108,051 | (50.5) | |
| Female | 105,960 | (49.5) | |
| Survey year | 0.0 | ||
| 2016 | 52,681 | (24.6) | |
| 2018 | 71,191 | (33.3) | |
| 2022 | 52,670 | (24.6) | |
| 2024 | 37,469 | (17.5) | |
| Grade | 0.0 | ||
| First (12–13‐year‐old students) | 69,237 | (32.4) | |
| Second (13–14‐year‐old students) | 71,847 | (33.6) | |
| Third (14–15‐year‐old students) | 72,927 | (34.1) | |
| Ever consumed substances | |||
| Alcohol | 41,784 | (19.7) | 0.9 |
| Tobacco | 3763 | (1.8) | 1.0 |
| Any Controlled drugs | 832 | (0.4) | 0.7 |
| Marijuana | 475 | (0.2) | 1.0 |
| Inhalants | 715 | (0.3) | 0.9 |
| Methamphetamine | 431 | (0.2) | 0.9 |
| NPS | 421 | (0.2) | 1.1 |
| Positive attitude toward underage substance use | |||
| Drinking | 32,894 | (15.5) | 1.1 |
| Smoking | 7973 | (3.8) | 1.0 |
| Any Controlled drugs | 4905 | (2.3) | 0.8 |
| Marijuana | 3564 | (1.7) | 0.8 |
| Inhalant | 3361 | (1.6) | 0.9 |
| Methamphetamine | 2952 | (1.4) | 0.9 |
| NPS | 2497 | (1.2) | 0.9 |
| Perceived ease of access to controlled drugs | |||
| Any Controlled drugs | 23,808 | (11.3) | 1.9 |
| Marijuana | 16,108 | (7.7) | 1.8 |
| Inhalant | 20,652 | (9.8) | 1.8 |
| Methamphetamine | 16,048 | (7.6) | 1.8 |
| NPS | 15,561 | (7.4) | 1.9 |
| Invited to use controlled drugs | |||
| Any controlled drugs | 1476 | (0.7) | 1.6 |
| Marijuana | 1072 | (0.5) | 0.9 |
| Inhalant | 996 | (0.5) | 0.9 |
| Methamphetamine | 1016 | (0.5) | 1.5 |
| NPS | 955 | (0.5) | 1.5 |
| Daily routine and social relationship disruptions | |||
| Irregular or late wake‐up time | 37,528 | (17.6) | 0.1 |
| Irregular or late bedtime | 85,323 | (39.9) | 0.2 |
| Skipping breakfast frequently | 8940 | (4.2) | 0.1 |
| Spending alone time without adult supervision | 26,253 | (12.3) | 0.7 |
| Dissatisfaction with school life | 22,160 | (10.4) | 0.4 |
| Lack of casual friends | 6570 | (3.1) | 0.3 |
| Lack of friends to confide in | 20,681 | (9.7) | 0.6 |
| Rarely consults with parents | 98,410 | (46.3) | 0.7 |
| Standardized prevalence (%) | OR | 95% CI |
| ||||
|---|---|---|---|---|---|---|---|
| Variables | 2016 | 2018 | 2022 | 2024 | |||
| Ever consumed substances | |||||||
| Alcohol | 27.7 (27.2–28.3) | 21.6 (21.2–22.0) | 14.5 (14.1–14.9) | 14.7 (14.2–15.3) | 0.89 | 0.89–0.89 | <0.001 |
| Tobacco | 2.2 (2.0–2.4) | 2.2 (2.1–2.3) | 1.2 (1.0–1.3) | 1.3 (1.1–1.5) | 0.91 | 0.90–0.93 | <0.001 |
| Controlled drugs | 0.5 (0.4–0.5) | 0.5 (0.5–0.6) | 0.2 (0.2–0.3) | 0.2 (0.1–0.2) | 0.87 | 0.85–0.90 | <0.001 |
| Marijuana | 0.3 (0.2–0.3) | 0.3 (0.3–0.4) | 0.1 (0.1–0.1) | 0.1 (0.0–0.1) | 0.85 | 0.82–0.88 | <0.001 |
| Inhalants | 0.4 (0.3–0.5) | 0.5 (0.4–0.5) | 0.2 (0.1–0.2) | 0.1 (0.1–0.2) | 0.86 | 0.83–0.89 | <0.001 |
| Methamphetamine | 0.2 (0.2–0.3) | 0.3 (0.3–0.4) | 0.1 (0.1–0.1) | 0.0 (0.0–0.1) | 0.84 | 0.81–0.87 | <0.001 |
| NPS | 0.2 (0.2–0.3) | 0.3 (0.2–0.4) | 0.1 (0.1–0.1) | 0.0 (0.0–0.1) | 0.86 | 0.83–0.89 | <0.001 |
| Positive attitude toward substance use | |||||||
| Drinking | 18.4 (17.9–18.9) | 16.3 (16–16.7) | 14.8 (14.4–15.2) | 11.7 (11.3–12.2) | 0.95 | 0.94–0.96 | <0.001 |
| Smoking | 3.6 (3.4–3.8) | 3.3 (3.2–3.5) | 4.0 (3.8–4.2) | 4.2 (4.0–4.5) | 1.03 | 1.02–1.04 | <0.001 |
| Controlled drugs | 2.0 (1.9–2.2) | 2.4 (2.2–2.5) | 2.1 (2.0–2.3) | 2.4 (2.2–2.6) | 1.01 | 0.99–1.02 | 0.352 |
| Marijuana | 1.4 (1.3–1.5) | 1.6 (1.5–1.7) | 1.8 (1.6–1.9) | 1.8 (1.6–2.0) | 1.04 | 1.02–1.05 | <0.001 |
| Inhalant | 1.5 (1.4–1.6) | 1.9 (1.8–2.0) | 1.2 (1.1–1.3) | 1.3 (1.2–1.5) | 0.96 | 0.95–0.98 | <0.001 |
| Methamphetamine | 1.2 (1.1–1.3) | 1.4 (1.3–1.5) | 1.2 (1.1–1.3) | 1.5 (1.3–1.7) | 1.01 | 0.99–1.02 | 0.27 |
| NPS | 1.1 (1.0–1.2) | 1.3 (1.2–1.4) | 1.0 (0.9–1.1) | 1.1 (1.0–1.3) | 0.99 | 0.97–1.00 | 0.09 |
| Perceived ease of access to controlled drugs | |||||||
| Controlled drugs | 13.9 (13.5–14.3) | 12.5 (12.2–12.8) | 9.1 (8.8–9.4) | 8.6 (8.1–9.0) | 0.93 | 0.92–0.93 | <0.001 |
| Marijuana | 8.9 (8.6–9.2) | 8.5 (8.2–8.7) | 6.6 (6.3–6.9) | 6.0 (5.6–6.4) | 0.94 | 0.94–0.95 | <0.001 |
| Inhalant | 12.3 (11.9–12.7) | 11.0 (10.7–11.3) | 7.5 (7.2–7.8) | 7.0 (6.6–7.4) | 0.92 | 0.91–0.92 | <0.001 |
| Methamphetamine | 9.2 (8.9–9.5) | 8.6 (8.3–8.8) | 6.2 (6.0–6.5) | 5.7 (5.3–6.1) | 0.93 | 0.92–0.94 | <0.001 |
| NPS | 9.4 (9.1–9.8) | 8.4 (8.1–8.7) | 5.6 (5.3–5.8) | 5.3 (4.9–5.7) | 0.91 | 0.91–0.92 | <0.001 |
| Invited to use controlled drugs | |||||||
| Any controlled drugs | 0.5 (0.4–0.6) | 0.5 (0.4–0.6) | 0.9 (0.8–1) | 0.9 (0.7–1.0) | 1.09 | 1.07–1.12 | <0.001 |
| Marijuana | 0.3 (0.2–0.3) | 0.3 (0.3–0.4) | 0.7 (0.6–0.8) | 0.7 (0.6–0.8) | 1.15 | 1.12–1.18 | <0.001 |
| Inhalant | 0.3 (0.3–0.4) | 0.3 (0.3–0.4) | 0.6 (0.5–0.7) | 0.6 (0.5–0.8) | 1.12 | 1.09–1.15 | <0.001 |
| Methamphetamine | 0.3 (0.2–0.3) | 0.3 (0.3–0.4) | 0.7 (0.6–0.7) | 0.7 (0.5–0.8) | 1.13 | 1.10–1.16 | <0.001 |
| NPS | 0.3 (0.2–0.3) | 0.3 (0.2–0.3) | 0.6 (0.5–0.7) | 0.6 (0.5–0.7) | 1.13 | 1.10–1.16 | <0.001 |
| Daily routine and social relationship disruptions | |||||||
| Irregular wake‐up time | 16.9 (16.5–17.4) | 17.4 (17.1–17.8) | 18.2 (17.7–18.6) | 17.3 (16.8–17.9) | 1.01 | 1.00–1.01 | 0.003 |
| Irregular bedtime | 40.5 (40.0–41.1) | 40.8 (40.3–41.2) | 38.7 (38.2–39.3) | 38.6 (37.8–39.3) | 0.99 | 0.98–0.99 | <0.001 |
| Skipping breakfast frequently | 3.7 (3.4–3.9) | 4.0 (3.9–4.2) | 4.7 (4.5–5.0) | 5.0 (4.7–5.3) | 1.04 | 1.03–1.05 | <0.001 |
| Spending alone time without adult supervision | 11.2 (10.8–11.5) | 12.7 (12.4–13) | 13.5 (13.1–13.9) | 11.5 (11.0–12.0) | 1.01 | 1.01–1.02 | <0.001 |
| Dissatisfaction with school life | 10.8 (10.4–11.1) | 10.4 (10.1–10.7) | 10.3 (10.0–10.6) | 9.3 (8.8–9.7) | 0.99 | 0.98–0.99 | <0.001 |
| Lack of casual friends | 3.4 (3.2–3.7) | 3.1 (2.9–3.2) | 3.2 (3.0–3.4) | 2.8 (2.6–3.0) | 0.99 | 0.98–1.00 | 0.025 |
| Lacks friends to confide in | 10.3 (9.9–10.7) | 9.2 (9.0–9.5) | 10.6 (10.2–10.9) | 9.4 (8.9–9.8) | 1.00 | 1.00–1.01 | 0.285 |
| Rarely consults with parents | 49.2 (48.7–49.8) | 46.4 (46–46.9) | 45.3 (44.7–45.8) | 43.5 (42.7–44.2) | 0.98 | 0.97–0.98 | <0.001 |
| Variable | Model A | Model B | Model B simpler | Model C | Model C simpler | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) |
| OR (95% CI) |
| OR (95% CI) |
| OR (95% CI) |
| OR (95% CI) |
| |
| Survey Year | 0.87 (0.84–0.91) | <0.001 | 0.86 (0.83–0.90) | <0.001 | 0.86 (0.83–0.90) | <0.001 | 0.86 (0.83–0.90) | <0.001 | 0.86 (0.83–0.90) | <0.001 |
| Sex | 0.77 (0.62–0.95) | 0.014 | 0.56 (0.46–0.69) | <0.001 | 0.56 (0.46–0.69) | <0.001 | 0.56 (0.46–0.69) | <0.001 | 0.56 (0.46–0.69) | <0.001 |
| Grade | 0.97 (0.85–1.10) | 0.614 | 1.11 (0.982–1.254) | 0.095 | 1.11 (0.98–1.26) | 0.090 | 1.12 (0.99–1.27) | 0.067 | 1.12 (0.99–1.27) | 0.068 |
| Ever consumed alcohol | 1.40 (1.08–1.82) | 0.011 | ||||||||
| Ever used tobacco | 3.31 (2.42–4.51) | <0.001 | ||||||||
| Positive attitude toward drinking | 0.91 (0.69–1.20) | 0.503 | ||||||||
| Positive attitude toward smoking | 0.90 (0.63–1.30) | 0.586 | ||||||||
| Positive attitude toward controlled drugs | 7.05 (5.08–9.78) | <0.001 | ||||||||
| Perceived ease of access to controlled drugs | 4.80 (3.70–6.21) | <0.001 | ||||||||
| Invited to use controlled drugs | 11.18 (8.31–15.03) | <0.001 | ||||||||
| Irregular wake‐up time | 1.55 (1.25–1.92) | <0.001 | 1.55 (1.25–1.92) | <0.001 | 1.56 (1.26–1.93) | <0.001 | 1.56 (1.26–1.92) | <0.001 | ||
| Irregular bedtime | 1.02 (0.83–1.26) | 0.854 | 1.01 (0.82–1.25) | 0.895 | 1.01 (0.82–1.25) | 0.919 | 1.01 (0.82–1.24) | 0.957 | ||
| Skipping breakfast frequently | 2.45 (1.83–3.28) | <0.001 | 2.47 (1.85–3.31) | <0.001 | 2.46 (1.84–3.29) | <0.001 | 2.49 (1.86–3.32) | <0.001 | ||
| Spending alone time without adult supervision | 1.68 (1.36–2.07) | <0.001 | 1.71 (1.39–2.10) | <0.001 | 1.71 (1.39–2.10) | <0.001 | 1.73 (1.40–2.12) | <0.001 | ||
| Dissatisfaction with school life | 1.16 (0.69–1.94) | 0.581 | 1.47 (1.17–1.86) | 0.001 | 1.20 (0.69–2.07) | 0.524 | 1.54 (1.21–1.95) | <0.001 | ||
| Lack of casual friends | 1.81 (0.81–4.05) | 0.152 | 2.39 (1.84–3.11) | <0.001 | ||||||
| Lack of friends to confide In | 1.07 (0.60–1.89) | 0.823 | 1.59 (1.25–2.01) | <0.001 | ||||||
| Rarely consults with parents | 1.29 (1.03–1.61) | 0.025 | 1.39 (1.14–1.70) | 0.001 | 1.20 (0.95–1.51) | 0.128 | 1.36 (1.11–1.66) | 0.003 | ||
| Dissatisfaction with School Life * Lack of casual friends | 0.26 (0.05–1.41) | 0.117 | ||||||||
| Dissatisfaction with School Life * Lack of Friends to confide in | 0.51 (0.17–1.56) | 0.235 | ||||||||
| Dissatisfaction with School Life * Rarely consults with parents | 1.21 (0.66–2.21) | 0.531 | 1.35 (0.71–2.58) | 0.364 | ||||||
| Lack of casual friends * Rarely consults with parents | 0.85 (0.32–2.26) | 0.737 | ||||||||
| Lack of friends to confide in * Rarely consults with parents | 1.58 (0.77–3.24) | 0.212 | ||||||||
| Dissatisfaction with School Life *Lack of casual friends *Rarely consults with parents | 9.63 (1.60–57.93) | 0.014 | ||||||||
| Dissatisfaction with School Life *Lack of Friends to confide in *Rarely consults with parents | 2.31 (0.66–8.11) | 0.190 | ||||||||
- —Health and Labour Sciences Research Grant from the Ministry of Health, Labour, and Welfare of Japan (Research Program on Regulatory Science of Pharmaceuticals and Medical Devices), under the project t
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSubstance Abuse Treatment and Outcomes · Smoking Behavior and Cessation · Attention Deficit Hyperactivity Disorder
INTRODUCTION
Adolescent use of controlled substances, including cannabis, inhalants, methamphetamine, and new psychoactive substances (NPS), is a well‐documented risk factor1, 2, 3, 4, 5, 6, 7, 8, 9, 10 for physical and mental health problems,11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24 academic disruption,14, 25, 26, 27, 28 and social isolation.12, 13, 29, 30 In response to growing global concern over these risks,31, 32 many countries have implemented nationwide, school‐based surveys to monitor youth drug use. Prominent examples include the Monitoring the Future study in the United States,33, 34 the European School Survey Project on Alcohol and Other Drugs,35 and the Global School‐based Student Health Survey conducted by the World Health Organization.36, 37 These surveys typically report a lifetime prevalence of several percent or more among adolescents aged 13–17 years.
In contrast, countries such as South Korea, Kuwait, Iraq, Mongolia, Vietnam, Malaysia, and Japan report markedly lower prevalence rates.38, 39 In these nations, the lifetime prevalence of adolescent drug use is approximately 0.9%–1.0%, considered exceptionally low by global standards. In Japan, national surveys have consistently reported a lifetime prevalence of controlled drug use below 1% among junior high school students (ages 12–15) over the past decade.40 Despite its low level, this prevalence has often been regarded as a public health concern.
Although adolescent drug use in Japan remains rare, its low prevalence presents unique challenges for research and policy. Even small numerical shifts may appear exaggerated, complicating trend analysis. Moreover, most national surveys use repeated cross‐sectional designs with limited adjustment for confounders, making it difficult to determine whether the observed year‐to‐year fluctuations reflect true behavioral changes or sampling variability. Another limitation is the lack of detailed analysis of psychosocial factors, such as drug‐related attitudes, perceived accessibility, and exposure to drug offers, which are often overlooked in low‐prevalence settings. Additionally, the small number of drug‐experienced adolescents limits statistical power, impeding the detection of meaningful risk patterns. As a result, vulnerable high‐risk subgroups may go unidentified.
Japanese studies from the 1990s identified individual‐level risk factors, such as male sex, substance co‐use, and irregular routines41, 42, 43, 44, 45, 46, 47; however, these do not reflect recent societal changes, including the rise of social media35 and evolving family dynamics.48 International research has pointed to additional risks, such as family stress,45, 49, 50, 51, 52 school difficulties,51, 53, 54 and peer disconnection5, 49, 50, 51, 55, 56, 57; however, few studies have explored how these factors interact or manifest in low‐prevalence countries such as Japan.58, 59
To address these gaps, this study analyzed nationally representative data from 2016 to 2024 to estimate the standardized lifetime prevalence of controlled drug use among Japanese junior high school students and to examine temporal changes in key psychosocial factors. Using design‐weighted logistic regression, we identified sociodemographic, behavioral, and psychosocial risk factors associated with drug use. These findings aim to inform targeted prevention strategies in Japan and offer insights relevant to other low‐prevalence settings.
METHODS
Survey design and target population
This study analyzed data from four repeated cross‐sectional, school‐based surveys conducted biennially in 2016, 2018, 2022, and 2024. The 2020 survey was not conducted due to the coronavirus disease 2019 (COVID‐19) pandemic.
Each wave employed a self‐administered, anonymous questionnaire distributed to junior high school students aged 12–15 years from a nationally representative sample of schools.
Stratified cluster sampling methodology
All students enrolled in randomly selected junior high schools in Japan were eligible to participate. According to the national school database used for sampling, between 3,269,341–3,486,807 students were enrolled in 10,111–10,533 public, private, and national junior high schools during each survey year.
A stratified one‐stage cluster sampling design was employed, using Japan's 47 prefectures as strata and individual schools as clusters. Within each prefecture, schools were selected using the probability‐proportional‐to‐size method based on student enrollment numbers. This approach ensured proportional representation of schools of varying sizes across all regions.
Each year, 236–244 schools were randomly selected from the national school database.
Survey implementation procedures
Surveys were administered from September to December in each respective survey year. Prior to implementation, explanatory materials, including cooperation requests, sample questionnaires, study overviews, and response forms, were distributed to selected schools and relevant administrative bodies.
Data were collected via self‐administered paper questionnaires in 2016, 2018, and 2022. In 2024, web‐based questionnaires were also introduced at the request of some schools, in addition to the paper format.
To ensure consistency across survey years and protect student privacy, questionnaires were completed in classrooms during regular school hours (e.g., homeroom or health education). Smartphones and personal devices were not permitted; students using the online format accessed the survey only through school‐issued devices.
Teachers provided instructions based on a standardized protocol and explained the study's purpose and procedures. Students were informed that participation was voluntary and anonymous, and that they could skip any questions or withdraw at any time without penalty. Consent was obtained by checking a box at the beginning of the questionnaire. Completed paper surveys were sealed in pre‐glued opaque envelopes that could not be reopened without breaking the seal. Online responses were submitted by closing the browser window.
Data entry and initial processing were outsourced to a third‐party organization to ensure consistency and efficiency. To maintain confidentiality, school names were not collected; only anonymized school IDs were used.
Ethical considerations
The survey protocols for all the years were approved by the Ethics Committee (A2022‐027, A2016‐022, and A2015‐128), and informed consent was obtained from all students in accordance with the Declaration of Helsinki.
Study population
The analytical sample was defined using pre‐specified criteria. Students were excluded if their responses were largely incomplete (e.g., <50% of items answered), if they were enrolled in special education programs, or if information on their sex was missing or recorded as non‐binary. The analysis focused on students in general education programs, who comprise most Japanese adolescents and attend relatively standardized schools.
Survey items and variables
Each survey included 32–35 items with minor variations across years. This study analyzed only the items common to all survey waves.40, 60, 61, 62, 63 The exact Japanese item wording is provided in a previous national report.40
The dependent variable was lifetime use of any controlled drug—self‐reported use of cannabis, inhalants, methamphetamine, or NPS. Although non‐medical use of over‐the‐counter (OTC) medications has become a growing concern in Japan,57 the survey included an OTC‐related item only in 2024 (not in 2016/2018/2022); therefore, OTC misuse was not included in the primary longitudinal analyses. Accordingly, the focus of this study was the use of regulated drugs.
Independent variables were selected based on previously published literature and theoretical relevance, and grouped into four domains: demographics, substance‐related attitudes and behaviors, lifestyle, and social relationships.14, 41, 42, 43, 44, 45, 46, 47, 56, 57, 58, 59, 64, 65, 66, 67, 68 Demographic variables (sex, grade, and survey year) were used as control variables. Substance‐related variables included lifetime alcohol and tobacco use, permissive attitudes toward controlled drug use, perceived ease of access to controlled drugs, and having received an invitation to use controlled drugs. Lifestyle variables included disruptions to daily routines (irregular sleep, skipping breakfast) and time without adult supervision. Based on prior Japanese research,57 we pre‐specified a dichotomous indicator (≥3 h vs <3 h) to proxy reduced supervision time—an “opportunity” window rather than family dysfunction—while improving model stability for rare outcomes. Social relationships were assessed with four items on peer interaction and emotional support. Social relationships were assessed using four items capturing everyday peer interaction and emotional support. These included dissatisfaction with school life, lack of casual friends to interact with, and occasionally, absence of friends to confide in, and rarely consulting parents.57, 68
Data cleaning procedures
To ensure data quality, responses related to lifetime‐controlled drug use were cleaned using predefined consistency rules. Students were asked about their use of four specific substances—marijuana, inhalants, methamphetamine, and NPS using the following response options: (1) never used, (2) used in the past year, and (3) used more than a year ago. These responses were cross‐checked with answers to general questions on drug use. In cases of inconsistency—for example, indicating “never used” for all substances while reporting general drug use—responses were adjusted to ensure logical consistency. Approximately 0.1% of the responses were revised based on these checks.
Statistical analyses
All statistical analyses were conducted using R (version 4.4.3) and IBM SPSS Statistics (version 29). We performed complete‐case analysis without imputation. The complex survey design accounted for stratification by prefecture, clustering by school, and post‐stratification weights based on school‐ and student‐level response rates.
We estimated both crude and standardized prevalence rates of lifetime‐controlled drug use, along with other drug‐related and psychosocial variables, for each survey year. Standardization was based on the sex and grade distribution from the 2024 survey. All analyses accounted for the complex survey design features mentioned above. Temporal trends were assessed using design‐weighted logistic regression, with survey year treated as a continuous variable.
To examine associated factors, we conducted multivariate design‐weighted logistic regression analyses using pooled data from all survey years. The outcome variable was the lifetime experience of controlled drug use (yes/no). Explanatory variables were grouped into three domains: (1) demographics, (2) attitudinal and behavioral factors, and (3) lifestyle and social relationships. Analyses were performed using the svyglm() function in R.
Three models were developed to assess the relationship between psychosocial factors and lifetime drug use. Model A included basic demographic and behavioral/attitudinal variables. Model B built upon this by adding lifestyle and social relationship variables. It also evaluated whether the combination of multiple social disconnection indicators—specifically school dissatisfaction, lack of casual friends, and infrequent parental consultation was associated with a greater risk than individual factors alone. Two‐ and three‐way interaction terms were included to assess this. Model C replaced “lack of casual friends” with “lack of friends to confide in,” to compare the impact of casual peer relationships versus emotionally supportive ones. These two friendship indicators were analyzed in separate models to avoid multicollinearity. Additionally, we conducted sensitivity analyses using simplified versions of Models B and C without interaction terms.
RESULTS
A total of 217,958 students participated in the survey between 2016 and 2024. After excluding 2,237 students with insufficient responses and 1,710 with missing or non‐binary sex data, the final analytical sample comprised 214,011 students (Figure 1). Participant characteristics are summarized in Table 1 and Table S1. The crude prevalence estimates were comparable to the standardized values, indicating minimal impact from standardization (Table S2).
Participant Flow from National Surveys (2016–2024).
The standardized lifetime prevalence of controlled drug use declined from 0.5% in 2016 to 0.2% in 2024 (odds ratio [OR] = 0.87), reflecting similar trends observed for alcohol and tobacco use (Table 2). The use of marijuana, inhalants, methamphetamine, and NPS also decreased. While permissive attitudes toward drug use generally declined, tolerance toward marijuana increased slightly (OR = 1.04). Perceived ease of access to drugs decreased (OR = 0.93), whereas reports of being offered drugs increased marginally (OR = 1.09). Risk‐related behaviors, such as irregular sleep, skipping breakfast, and extended unsupervised time, showed modest increases. In contrast, indicators of social disconnection school dissatisfaction, lack of casual friends, and limited communication with parents, declined gradually.
Multivariate logistic regression analysis indicated that more recent survey years (OR = 0.87) and female sex (OR = 0.77) were consistently associated with lower odds of drug use (Table 3). In Model A, significant associations were observed for lifetime alcohol use (OR = 1.40), tobacco use (OR = 3.31), permissive attitudes (OR = 7.05), perceived ease of access (OR = 4.08), and prior drug use (OR = 11.18). Model B incorporated lifestyle variables, including irregular wake‐up time (OR = 1.55), skipping breakfast (OR = 2.45), and extended unsupervised time (OR = 1.68). A notable three‐way interaction was observed between school dissatisfaction, lack of casual friends, and rare consultations with parents (OR = 9.63). Model C, which replaced “lack of confidants” instead of “lack of casual friends” with “lack of friends to confide in” yielded similar results for lifestyle variables, although interaction terms were not significant. In the simplified versions of Models B and C (excluding interaction terms), all six psychosocial variables remained significantly associated with drug use. Sensitivity analyses supported these findings, with consistent effect estimates and similar Akaike Information Criterion values across models (Table 3).
DISCUSSION
Between 2016 and 2024, despite increases in tolerant attitudes toward cannabis and experiences of being offered drugs, the lifetime prevalence of controlled drug use among Japanese adolescents declined, reaching 0.2% in 2024. Key risk factors included permissive attitudes, perceived ease of access, lifestyle disruptions, and social isolation, particularly when multiple risk factors overlapped.
During the study period, the lifetime prevalence of controlled drug use among Japanese adolescents aged 12–15 years declined from 0.5% to 0.2%. This trend was consistent across all major substances and remained robust after adjusting for grade and sex. Over the same period, permissive attitudes toward drug use generally declined, although tolerance toward cannabis increased slightly. The proportion of students who perceived drugs as easily accessible decreased, whereas reports of being offered drugs showed a modest increase.
Even though the risk of being offered drugs increased,14, 41, 42, 43, 44, 45, 46, 47, 56, 58, 59, 64, 65, 66, 67, 68 actual drug use continued to decline. This seemingly paradoxical trend may reflect the growing influence of protective factors, such as strong internalized norms against drug use, increased health awareness, and early preventive education. The low prevalence may be attributed to a combination of strict drug control laws (e.g., criminalization of drug use), sustained school‐based prevention programs, societal disapproval, and pervasive social stigma, all of which likely act as deterrents to adolescent drug use.57, 69, 70, 71 In other words, even when adolescents are exposed to interpersonal risks, they may resist drug use due to reinforced personal values and strong societal norms. In our survey, more than 97% of students expressed opposition to drug use (Table 2), suggesting that abstinence may reflect not only behavioral restraint but also deeply rooted personal convictions and socially reinforced norms. It is also plausible that reduced peer interaction during the COVID‐19 pandemic contributed to the sharp decline observed in 2024, although this remains speculative.
While overall exposure to drugs appears to be declining, several concerns warrant attention. The slight increase in reports of drug offers suggests that some adolescents remain in high‐risk social environments. Simultaneously, the modest rise in cannabis tolerance may be influenced by global legalization trends and increased online exposure to cannabis‐related content.16, 24, 67, 72, 73, 74 These findings highlight that despite general improvements, specific subgroups may continue to face elevated risks due to their social context and evolving perceptions of certain substances.
Additionally, minor increases were observed in lifestyle disruptions, such as irregular sleep, skipping breakfast, and spending unsupervised time, all of which were significantly associated with drug use in this and prior studies.36, 75, 76, 77, 78, 79 These behavioral changes may reflect broader societal shifts, including the rise in dual‐income and single‐parent households,48 potentially resulting in reduced parental oversight.
Drug use among adolescents was associated with male sex, prior alcohol or tobacco use, permissive attitudes toward drug use, perceived ease of access, and experiences of being offered drugs. Lifestyle disruptions and weak connections with family and school were also identified as key risk factors. These findings align with those of previous studies conducted in Japan and internationally,14, 41, 42, 43, 44, 45, 46, 47, 56, 58, 59, 64, 65, 66, 67, 68 suggesting that adolescent drug use may be driven more by psychosocial vulnerabilities than by individual choice alone.
This study highlights the importance of weak family and school connections as significant contributors to adolescent drug use. Consistent with earlier findings, being offered drugs was strongly associated with actual use. While past research has emphasized the role of delinquent peers in promoting drug use,49, 50, 80, 81 the present findings—emphasizing both social isolation and drug offers—may appear somewhat inconsistent with the existing literature.
Several factors may help explain this discrepancy. In addition to the conventional pressure exerted by delinquent peer groups, socially isolated adolescents may be drawn to deviant groups as a means of seeking emotional connection or belonging.82, 83 Prior studies have shown that involvement in such groups can offer a sense of acceptance or a place to “fit in.”51, 55, 84 Moreover, in contexts where adolescents lack supportive family or social relationships, psychological vulnerabilities, such as low self‐esteem or anxiety, may play a role. Under such conditions, being offered drugs may not only present a behavioral opportunity but also be perceived as a temporary source of comfort or escape.
This study observed that the co‐occurrence of three social disconnection factors—school dissatisfaction, lack of casual friends, and limited communication with parents—was associated with a substantially higher likelihood of drug use. Specifically, the odds ratio for students experiencing all three conditions was 9.63. Table S3 indicates that the prevalence of drug use among this subgroup was 3.34%, compared to 0.25% among students without any of these risk factors a more than tenfold difference. These findings suggest that multiple forms of social isolation may have a cumulative impact on vulnerability to drug use. Furthermore, the results from Model B and its simplified version indicated that having at least one positive connection with school, peers, or parents was associated with lower odds of drug use. It is important to note, however, that the number of students reporting all three disconnection factors was relatively small (n = 68), and the 95% confidence interval for the corresponding interaction term was wide (1.60–57.93). This limits the precision of the OR estimate; thus, the findings should be interpreted with caution. Nonetheless, identifying such high‐risk subgroups remains important from a public health perspective, underscoring the value of targeted interventions for adolescents facing multiple psychosocial vulnerabilities.
Furthermore, the findings from Models B and C suggest that both emotionally close relationships and relatively casual social ties may offer protective effects. These observations underscore the importance of promoting diverse opportunities for social engagement as a strategy to prevent adolescent drug use.
Between 2016 and 2024, improvements were observed in school satisfaction, peer relationships, and parent–child communication among Japanese adolescents. Despite these positive trends, difficulties in interpersonal relationships remained significantly associated with drug use. This suggests that enhancements in the overall social environment may not be sufficient to protect all adolescents, particularly those experiencing persistent social disconnection. One possible explanation is that such individuals may not fully engage with or benefit from existing support systems if these are perceived as emotionally unsafe, inaccessible, or untrustworthy. In this study, students who rarely or never consulted their parents or friends were significantly more likely to report drug use. This suggests that at‐risk adolescents may be less inclined or less able to seek help or initiate communication during times of difficulty. Although these perceptions were not directly assessed in this study, previous research has emphasized the importance of adolescents' subjective experiences in shaping the effectiveness of school‐ and family‐based interventions.85, 86, 87 Taken together, these findings imply that preventive strategies should not only address peer norms and provide structural support but also foster a sense of belonging and emotional safety within school and family environments.58, 85, 88, 89 Moreover, the provision of alternative drug‐free environments, such as community‐based settings that facilitate non‐judgmental peer interactions, may offer critical support for socially isolated adolescents and reduce their susceptibility to drug use.
This study was a design‐based cross‐sectional analysis; therefore, its conclusions are limited to individual‐level associations. Even with that caveat, patterns observed in Japan may be informative for other low‐prevalence settings (e.g., South Korea and parts of the Middle East).38, 39 In such contexts, stringent drug laws, strong social disapproval, and internalized anti‐drug norms may contribute to lower prevalence.90 In Japan, conservative cultural norms alongside institutional prevention efforts may also deter initiation.91 By contrast, higher‐prevalence countries (e.g., the United States and parts of Europe) often report greater adolescent use in tandem with sensation‐seeking, peer normalization, and more permissive attitudes toward cannabis, trends shaped in part by legalization and media narratives that may weaken traditional deterrents.92, 93, 94
At the same time, our findings suggest that structural protections are not sufficient for all adolescents. Youth with weak connections to family, school, or peers, particularly those who rarely communicate with their parents or report low school satisfaction, are more likely to report drug use. Similar patterns have been observed in the United Arab Emirates, where socially isolated adolescents face increased risks despite strong legal and cultural controls.95 These findings underscore the need to complement legal frameworks with interventions that foster emotional connection and support.13, 51, 85, 96, 97, 98, 99
Overall, the findings suggest that strategies in low‐prevalence countries should not only focus on maintaining structural and legal deterrents but also prioritize the betterment of adolescents' emotional well‐being and sense of connectedness within family and school environments. Complementary measures, such as the provision of community‐based, drug‐free settings where adolescents can form meaningful relationships, may support those less likely to be reached through traditional prevention programs.
Finally, as this is a cross‐sectional study, causal inference is not possible, and structural factors were not directly measured. Future research should test these hypotheses using designs that incorporate contextual indicators (e.g., enforcement, availability, socioeconomic conditions).
This study has some limitations. All data were self‐reported and may be subject to recall or social desirability bias. Key confounders, such as parental substance use, mental health status, and family background, were not assessed. The cross‐sectional design precludes causal interpretation, and some subgroup analyses may have lacked statistical power. Selection bias is also possible, as non‐participating students may differ systematically from those included in the sample. Finally, the 2024 wave was administered in mixed modes (paper and a secure web platform). Potential response‐mode effects on self‐reports cannot be fully ruled out.
Although this study focused on illicit drugs, the increasing misuse of legal substances among Japanese adolescents, such as over‐the‐counter and prescription medications, has become a growing concern with increasing rates of overdose and addiction.57, 100, 101 These trends, observed in other countries as well,102, 103, 104 highlight the need for broader surveillance systems that capture both legal and illegal substance use to protect at‐risk youth.
Controlled drug use declined among Japanese junior high school students between 2016 and 2024, but remained concentrated among those with disrupted daily routines and indicators of social isolation. These findings underscore the need for targeted prevention interventions, even in low‐prevalence settings.
AUTHOR CONTRIBUTIONS
Takuya Shimane, Kunihiko Kitagaki, Akihiro Koide, and Satoshi Inoura designed the preliminary experiments and established the participant database. Takuya Shimane, Kunihiko Kitagaki, Akihiro Koide, and Satoshi Inoura recruited the participants and collected the data. Takuya Shimane secured funding. Takuya Shimane and Satoshi Inoura designed the study and performed the statistical analyses. Satomi Mizuno drafted the manuscript. Takuya Shimane, Satoshi Inoura, Toshihiko Matsumoto, Kunihiko Kitagaki, Akihiro Koide, and Kenji Takehara supervised manuscript preparation. All authors have revised, reviewed, revised, and approved the final version of the manuscript for publication.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS APPROVAL STATEMENT
This study was approved by the Ethics Committee of the National Centre of Neurology and Psychiatry, Japan (approval number: A2022‐027, A2016‐022, and A2015‐128). This study was conducted in accordance with the principles of the Declaration of Helsinki and the STROBE reporting guidelines.
PATIENT CONSENT STATEMENT
Participants were informed of the purpose of the study, and those who expressed interest were invited to participate after providing written informed consent. Written informed consent was obtained from all study participants in both original studies.
CLINICAL TRIAL REGISTRATION
This observational study did not qualify as a clinical trial according to the guidelines established by the International Committee of Medical Journal Editors.
Supporting information
Supporting information 20250825.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Azofeifa A , Mattson ME , Fogarty K , Lyerla R. Characterizing marijuana use disorders (DSM‐5)—National survey on drug use and health, United States, 2020. Int J Ment Health Addict. 2023;23:790–810. 10.1007/S 11469-023-01137-4 · doi ↗
- 2Degenhardt L , Bharat C , Glantz MD , Sampson NA , Al‐Hamzawi A , Alonso J , et al. Association of cohort and individual substance use with risk of transitioning to drug use, drug use disorder, and remission from disorder: findings from the world mental health surveys. JAMA Psychiatry. 2019;76:708–720. 10.1001/JAMAPSYCHIATRY.2019.0163 30865282 PMC 6583659 · doi ↗ · pubmed ↗
- 3Hall W , Degenhardt L . Prevalence and correlates of cannabis use in developed and developing countries. Curr Opin Psychiatry. 2007;20:393–397. 10.1097/YCO.0B 013E 32812144 CC 17551355 · doi ↗ · pubmed ↗
- 4Calabria B , Degenhardt L , Hall W , Lynskey M . Does cannabis use increase the risk of death? Systematic review of epidemiological evidence on adverse effects of cannabis use. Drug Alcohol Rev. 2010;29:318–330. 10.1111/J.1465-3362.2009.00149.X 20565525 · doi ↗ · pubmed ↗
- 5Kandel DB . On processes of peer influences in adolescent drug use: a developmental perspective. Adv Alcohol Subst Abuse. 1985;4:139–162. 10.1300/J 251V 04N 03_07 3874527 · doi ↗ · pubmed ↗
- 6Moore TH , Zammit S , Lingford‐Hughes A , Barnes TR , Jones PB , Burke M , et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. The Lancet. 2007;370:319–328. 10.1016/S 0140-6736(07)61162-3 17662880 · doi ↗ · pubmed ↗
- 7Moore KE , Oberleitner LMS , Zonana HV , Buchanan AW , Pittman BP , Verplaetse TL , et al. Psychiatric disorders and crime in the US population: results from the National Epidemiologic Survey on alcohol and related conditions wave i II. J Clin Psychiatry. 2019;80 (2):18m 12317. 10.4088/JCP.18m 12317 PMC 782620130758921 · doi ↗ · pubmed ↗
- 8Nkansah‐Amankra S , Minelli M . “Gateway hypothesis” and early drug use: additional findings from tracking a population‐based sample of adolescents to adulthood. Prev Med Rep. 2016;4:134–141. 10.1016/j.pmedr.2016.05.003 27413674 PMC 4929049 · doi ↗ · pubmed ↗