Regional Burden of Urinary Tract Infection, Its Aetiologies, and Antibiotic Resistance Patterns, 2020–2023: A Retrospective Study
Solomon Wireko, Gifty Ngmaakan, Doreen Dwomoh, Charlotte Hansen, Sampson Nartey, Ebenezer Senu

TL;DR
This study examines the causes and antibiotic resistance of urinary tract infections in Ghana's Ashanti Region from 2020 to 2023, highlighting the rise of drug-resistant bacteria.
Contribution
The study provides recent regional data on UTI pathogens and their resistance patterns, emphasizing the growing threat of multidrug-resistant strains.
Findings
Escherichia coli was the most common UTI pathogen (47.8%), with high resistance to Nalidixic acid and Ofloxacin.
Klebsiella pneumoniae showed significant resistance to Cefotaxime, Ciprofloxacin, and Trimethoprim/Sulfamethoxazole.
Multidrug-resistant gram-negative isolates, including ESBL-producing strains, are a major concern for UTI treatment.
Abstract
The emergence of antibiotic‐resistant strains of urinary tract infections (UTI) pathogens poses a significant challenge to the effective treatment of this condition. This study aimed to conduct a retrospective study to analyze the etiology and antibiotic resistance patterns of common urinary tract pathogens in the Ashanti Region of Ghana. The study employed a standardized data collection form to extract information on age, sex, urine culture results, antibiotic susceptibility test results, and antibiotic treatment regimens from 2020 to 2023. The primary agent responsible for UTIs was Escherichia coli, identified in 47.8% of cases, followed by Klebsiella pneumoniae at 15.8%, Staphylococcus aureus at 9.2%, and Pseudomonas aeruginosa at 6.5%. Candida species were detected in 12% of cases, while coagulase‐negative Staphylococci constituted 3.8%. Proteus and Providencia species were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
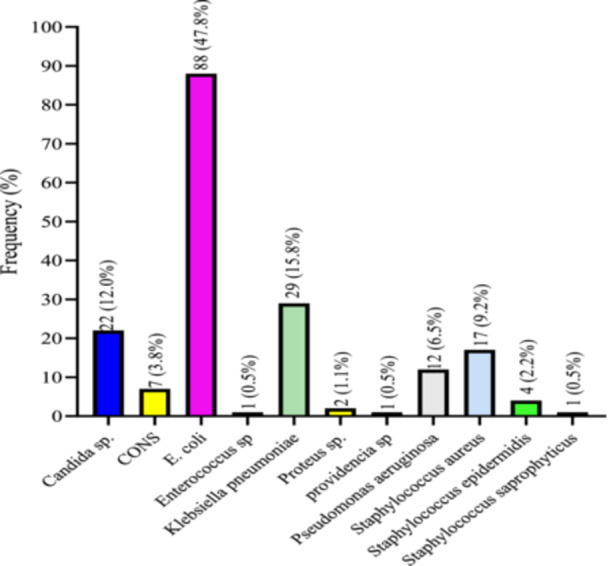 Figure 1
Figure 1| Variable | Total ( | Percentage (%) |
|---|---|---|
| Age | ||
| 1–20 | 22 | 12 |
| 21–40 | 75 | 40.8 |
| 41–60 | 47 | 25.5 |
| 61–80 | 32 | 17.4 |
| 81–100 | 8 | 4.3 |
| Gender | ||
| Females | 129 | 70.1 |
| Males | 55 | 29.9 |
| Age (years) | |||||||
|---|---|---|---|---|---|---|---|
| Total ( | 1–20 ( | 21–40 ( | 41–60 ( | 61–80 ( | 81–100 ( |
| |
| Isolates | 0.453 | ||||||
|
| 22 (12.0) | 5 (22.7) | 11 (14.7) | 4 (8.5) | 2 (6.3) | 0 (0.0) | |
| CONS | 7 (3.8) | 2 (9.1) | 3 (4.0) | 2 (4.3) | 0 (0.0) | 0 (0.0) | |
|
| 88 (47.8) | 5 (22.7) | 32 (42.7) | 27 (57.4) | 20 (62.5) | 4 (50.0) | |
|
| 1 (0.5) | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
|
| 29 (15.8) | 5 (22.7) | 9 (12.0) | 7 (14.9) | 7 (21.9) | 1 (12.5) | |
|
| 2 (1.1) | 0 (0.0) | 1 (1.3) | 1 (2.1) | 0 (0.0) | 0 (0.0) | |
|
| 1 (0.5) | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
|
| 12 (6.5) | 0 (0.0) | 4 (5.3) | 4 (6.5) | 2 (6.3) | 2 (25.0) | |
|
| 17 (9.2) | 4 (18.2) | 10 (13.3) | 2 (4.3) | 1 (3.1) | 0 (0.0) | |
|
| 4 (2.2) | 1 (4.5) | 2 (2.7) | 0 (0.0) | 0 (0.0) | 1 (12.5) | |
|
| 1 (0.5) | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Total ( | Females ( | Male ( |
| |
|---|---|---|---|---|
| Isolates |
| |||
|
| 22 (12.0) | 22 (17.1) | 0 (0.0) | |
| CONS | 7 (3.8) | 6 (4.7) | 1 (1.8) | |
|
| 88 (47.8) | 66 (51.2) | 22 (40.0) | |
|
| 1 (0.5) | 1 (0.8) | 0 (0.0) | |
|
| 29 (15.8) | 18 (14.0) | 11 (20.0) | |
|
| 2 (1.1) | 1 (0.8) | 1 (1.8) | |
|
| 1 (0.5) | 1 (0.8) | 0 (0.0) | |
|
| 12 (6.5) | 3 (2.3) | 9 (16.4) | |
|
| 17 (9.2) | 10 (7.8) | 7 (12.7) | |
|
| 4 (2.2) | 0 (0.0) | 4 (7.3) | |
|
| 1 (0.5) | 1 (0.8) | 0 (0.0) |
| CONS ( |
|
|
|
| ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Antibiotics | S | R | S | R | S | R | S | R | S | R |
| GEN | 1 (100.0) | 0 (0.0) | 15 (51.7) | 14 (48.3) | 1 (100) | 0 (0.0) | 5 (62.5) | 3 (37.5) | — | — |
| CIP | 2 (100.0) | 0 (0.0) | 12 (24.5) | 37 (75.5) | 0 (0.0) | 1 (100.0) | 3 (18.8) | 13 (81.3) | 0 (0.0) | 1 (100.0) |
| SXT | 1 (100.0) | 0 (0.0) | 16 (32.0) | 34 (68.0) | — | — | 3 (20.0) | 12 (80.0) | 1 (100.0) | 0 (0.0) |
| CTR | 10 (31.3) | 22 (68.8) | — | — | 2 (20.0) | 8 (80.0) | 1 (50.0) | 1 (50.0) | ||
| CTZ | 1 (100.0) | 0 (0.0) | 20 (52.6) | 18 (47.4) | — | — | 8 (61.5) | 5 (38.5) | — | — |
| MEM | 8 (80.0) | 2 (20.0) | — | — | 4 (100.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | ||
| AMI | 1 (100.0) | 0 (0.00) | 10 (52.6) | 9 (47.4) | — | — | 6 (60.4) | 4 (40.0) | 0 (0.0) | 1 (100.0) |
| NAL | 0 (0.0) | 1 (100.0) | 0 (0.0) | 12 (100.0) | — | — | 3 (75.0) | 1 (25.0) | — | — |
| DOX | 1 (14.3) | 6 (85.7) | — | — | — | — | — | — | ||
| AMO | 6 (30.0) | 14 (70.0) | — | — | 4 (33.3) | 8 (66.7) | 1 (100.0) | 0 (0.0) | ||
| AZI | 2 (66.7) | 1 (33.3) | 13 (61.9) | 8 (38.1) | 0 (0.0) | 1 (100.0) | 6 (85.7) | 1 (14.3) | 0 (0.0) | 1 (100.0) |
| OFL | 0 (0.0) | 4 (100.0) | — | — | — | — | 1 (100.0) | 0 (0.0) | ||
| ERY | 1 (100.0) | 0 (0.0) | 2 (66.7) | 1 (33.3) | — | — | 0 (0.0) | 2 (100.0) | — | — |
| CTX | 1 (100.0) | 0 (0.0) | 12 (48.0) | 13 (52.0) | — | — | 1 (10.0) | 9 (90.0) | — | — |
| CMP | 0 (0.0) | 1 (100.0) | 11 (50.0) | 11 (50.0) | — | — | 5 (50.0) | 5 (50.0) | — | — |
| TET | 1 (100.0) | 0 (0.0) | 10 (37.0) | 17 (63.0) | 0 (0.0) | 1 (100.0) | 3 (33.3) | 6 (66.7) | — | — |
| VAN | 1 (100.0) | — | — | — | — | — | — | — | ||
| CRX | 7 (38.9) | 11 (61.1) | — | — | 2 (22.2) | 7 (77.8) | — | — | ||
| AMP | 2 (33.3) | 4 (66.7) | — | — | 1 (50.0) | 1 (50.0) | — | — | ||
| MDR | — | + | + | + | + | |||||
|
|
|
|
|
| ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Antibiotics | S | R | S | R | S | R | S | R | S | R |
| GEN | — | — | 5 (71.4) | 2 (28.6) | 4 (57.1) | 3 (42.9) | 2 (100.0) | 0 (0.0) | — | — |
| CIP | 0 (0.0) | 1 (100.0) | 6 (60.0) | 4 (40.0) | 5 (55.6) | 4 (44.4) | 0 (0.0) | 1 (100.0) | — | — |
| SXT | — | — | 2 (28.6) | 5 (71.4) | 4 (33.3) | 8 (66.7) | 2 (100.0) | 0 (0.0) | 1 (100.0) | 0 (0.0) |
| CTR | — | — | 2 (28.6) | 5 (71.4) | — | — | — | — | — | — |
| CTZ | 1 (100.0) | 0 (0.0) | 5 (83.3) | 1 (16.7) | 0 (0.0) | 2 (100.0) | 1 (100.0) | 0 (0.0) | — | — |
| MEM | 1 (100.0) | 0 (0.0) | 3 (100.0) | 0 (0.0) | — | — | — | — | — | — |
| AMI | — | — | 1 (33.3) | 2 (67.7) | — | — | — | — | — | — |
| NAL | — | — | 0 (0.0) | 1 (100.0) | — | — | — | — | — | — |
| DOX | — | — | 0 (0.0) | 1 (100.0) | 2 (66.7) | 1 (33.3) | — | — | — | — |
| AMO | — | — | 3 (75.0) | 1 (25.0) | 1 (100.0) | 0 (0.0) | — | — | — | — |
| AZI | 1 (100.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | 8 (72.7) | 3 (27.3) | 0 (0.0) | 1 (100.0) | 1 (100.0) | 0 (0.0) |
| OFL | — | — | — | — | 2 (66.7) | 1 (33.3) | — | — | — | — |
| ERY | — | — | 1 (100.0) | 0 (0.0) | 7 (70.0) | 3 (30.0) | — | — | 0 (0.0) | 1 (100.0) |
| CTX | — | — | 0 (0.0) | 3 (100.0) | — | — | — | — | 0 (0.0) | 1 (100.0) |
| CMP | — | — | — | — | 2 (50.0) | 2 (50.0) | — | — | 1 (100.0) | 0 (0.0) |
| TET | — | — | — | — | 1 (12.5) | 7 (87.5) | 1 (50.0) | 1 (50.0) | — | — |
| VAN | — | — | — | — | — | — | — | — | — | — |
| CRX | — | — | 0 (0.0) | 1 (100.0) | — | — | — | — | — | — |
| AMP | — | — | — | — | — | — | 0 (0.0) | 1 (100.0) | — | — |
| MDR | — | + | + | + | — | |||||
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Antibiotic Resistance in Bacteria · Escherichia coli research studies
Introduction
1
Urinary tract infections (UTIs) represent a prevalent global health concern, affecting millions of individuals annually and posing a substantial burden on healthcare systems [1, 2, 3]. Defined by the presence of pathogenic microorganisms in the urinary system, UTIs encompass a spectrum of conditions ranging from asymptomatic bacteriuria to severe, recurrent infections [4, 5, 6]. Common microbial agents of UTI include Escherichia coli, Klebsiella pneumoniae, Enterococcus faecalis, and Pseudomonas aeruginosa. Among the diverse demographic groups affected, individuals with compromised immune systems or underlying medical conditions, such as type 2 diabetes mellitus (T2DM) patients, are particularly vulnerable to urinary tract complications [7, 8, 9]. Aging, immunosuppressive therapy, chronic kidney disease, and malignancies are additional causes of immune compromise, alongside T2DM.
Although there is limited data on the overall national occurrence of UTIs in Ghana, two investigations have indicated a prevalence of 42.75% in pregnant women [10] and 86% in hospitalized adults [11]. Reports suggest that the percentage of multidrug‐resistant (MDR) UTIs in Ghana can be as high as 93.6% [12, 13].
Understanding the regional variations in UTI prevalence, causative agents, and antibiotic resistance patterns is crucial for informed public health interventions. This retrospective study aims to analyze the antibiotic resistance patterns of common urinary tract pathogens spanning the years 2020 to 2023. By examining a comprehensive data set, we seek to elucidate the magnitude of the UTI burden, identify the prevalent aetiologies, and unravel the evolving patterns of antibiotic resistance within our defined geographical scope.
Several studies have shed light on the global impact of UTIs, emphasizing the need for context‐specific investigations to address regional subtle variations or differences [14, 15]. Moreover, the intersectionality of UTIs with chronic conditions like T2DM adds layers of complexity, demanding the ability to grasp and appreciate the fine details, exceptions, and context‐specific elements that contribute to a more comprehensive and insightful perspective on the interplay between host factors, regional epidemiology, and microbial characteristics [4, 16]. This study is motivated by the need to fill gaps in the existing literature, providing a detailed analysis of the regional dynamics surrounding UTIs.
Materials and Methods
2
Study Design and Site
2.1
The study adopted a retrospective design, encompassing data collected over the period from 2020 to 2023. This design involved the analysis of historical patient records, laboratory reports, and relevant documentation to investigate UTIs within the specified timeframe. The data were collected from five healthcare facilities, including one tertiary hospital and four district hospitals within the Ashanti Region. The retrospective approach allows for the examination of trends, prevalence rates, causative agents, and antibiotic resistance patterns over the 3‐year period. The study was focused on the Ashanti region of Ghana, and the analysis is tailored to understand the dynamics of UTIs within this defined area. The study included both inpatient and outpatient cases. Approximately 34.8% (64/184) of the samples were from outpatient departments, and 65.2% (120/184) were from hospitalized patients.
Data Collection
2.2
The primary sources of data for this study included electronic health records (EHRs), laboratory reports detailing diagnostic findings related to UTIs, and patient charts containing relevant clinical details.
Information extracted from EHRs encompassed demographic data, medical history, laboratory test results, and prescribed treatments. This comprehensive data set allowed for a thorough analysis of patient profiles and UTI‐related information. Laboratory reports contributed essential microbiological data, identifying causative agents of UTIs, and offered insights into bacterial isolates, antibiotic susceptibility patterns, and any additional relevant diagnostic information.
Detailed patient charts also provided clinicians' notes, treatment regimens, and any pertinent clinical observations. These records contributed to a holistic understanding of individual patient cases.
Antimicrobial Susceptibility Testing
2.3
Information on antimicrobial susceptibility patterns was extracted from laboratory records of urine culture reports between 2020 and 2023. According to standard protocol at the participating laboratories, susceptibility testing was performed using the Kirby‐Bauer disk diffusion method, and results were interpreted following the Clinical and Laboratory Standards Institute (CLSI) 2020 guidelines. Only isolates with complete susceptibility data were included in the analysis. ESBL production was detected using the phenotypic confirmatory combination disk method, following CLSI guidelines.
MDR was defined according to the international consensus by Magiorakos et al. [17] as resistance to at least one agent in three or more antimicrobial categories.
Inclusion and Exclusion Criteria
2.4
Patients included in the study were those with a documented diagnosis of UTI during the specified period from 2020 to 2023. This timeframe ensures a contemporary representation of UTI cases and allows for the exploration of potential temporal trends. Emphasis was placed on capturing a diverse range of UTI cases, considering variations in severity, recurrence, and comorbidities.
Patients with incomplete or insufficient data (records missing key clinical information such as urine culture results, antibiotic susceptibility profiles, or patient demographic details) hindering a comprehensive analysis were excluded, as well as cases involving UTIs with known alternative aetiologies, such as urinary tract abnormalities or malignancies, to maintain the specificity of the study.
Ethical Considerations
2.5
The study received ethical approval (IRID/EC2022/HS003) from the Institute of Research Innovation and Development (IRID) of Kumasi Technical University, and the committee waived the requirement for informed consent due to the retrospective and anonymized nature of the study. Permission was granted by the Ghana Health Service Ashanti Regional Health Directorate (Ref. No. GHS/ASH/INTRO).
Data Access and Usage
2.6
The study strictly adhered to ethical standards regarding data access and usage. Access to patient records and related information was granted only to authorized personnel involved in the research by the Ashanti Regional Health Directorate of the Ghana Health Service, and all data was handled in compliance with institutional and legal regulations. All data collected, including EHRs, laboratory reports, and patient charts, were treated with the utmost confidentiality. Personal identifiers were appropriately anonymized to prevent the disclosure of individual identities.
Data Analysis
2.7
Data was cleaned and exported to the Statistical Package for the Social Sciences (IBM SPSS Statistics version 26). The data were expressed in percentages and frequencies, and the Chi‐square test was used to determine significant differences between the variables. Statistical significance was accepted in all comparisons at a *p‐*value less than 0.05.
Results
3
Age and Gender Distribution of Study Participants With Positive Bacterial Infection
3.1
Of the 184 individuals diagnosed with positive bacterial infections, the preponderance consisted of females, comprising 70.1% (129/184) of the total, with males representing 29.9% (74/184). Most participants were distributed across the age brackets of 21–40 and 41–60 years, constituting 40.8% (75/184) and 25.5% (46/184) of the overall participant count, respectively. The age range of 1–20 years constituted 12% (22/184) of the participants, while individuals aged 61–80 and 81–100 years comprised 17.4% (32/184) and 4.3% (8/184) of the study cohort (see Table 1).
Prevalence of Organisms Causing UTI Among Study Participants
3.2
E. coli was the most frequently isolated organism, accounting for 47.8% (88/155) of cases, followed by K. pneumoniae 15.8% (24/155), Staphylococcus aureus 9.2% (14/155), and P. aeruginosa 6.5% (10/155). Candida species were identified in 12% (19/155) of cases. Among the coagulase‐negative Staphylococci (CONS), Staphylococcus epidermidis accounted for 2.2%, while other CONS (excluding Staphylococcus saprophyticus) constituted 3.8% of isolates. Proteus and Providencia species were detected in 1.1% and 0.5% of cases, respectively. Both Enterococcus spp. and S. saprophyticus each represented 0.5% of the total isolates (Figure 1).
Prevalence of Organisms causing UTI among study participants.
Age Distribution of Isolated Organisms Causing UTI Among Study Participants
3.3
This study did not identify any statistically significant association between the distribution of isolates and age groups. Notably, E. coli emerged as the predominant pathogen, particularly prevalent in the 41–60 years age group, constituting 57.4% of cases. Candida spp. cases were predominantly observed in the 1–20 age group, accounting for 22.7%. Candida isolates were reported only when found in significant colony counts (> 10⁵ CFU/mL) and in symptomatic patients, following standard diagnostic criteria for fungal UTIs. CONS and Enterococcus spp. were distributed across age groups, with CONS being most prevalent in the 1–20 age group at 9.1%. Providencia spp. was isolated exclusively in the 21–40‐year‐old age group. K. pneumoniae displayed varied prevalence, with the highest proportion in the 61–80 years age group at 21.9%. Proteus sp. and P. aeruginosa were primarily present in the 21–40 and 41–60 years age groups, with P. aeruginosa having the highest occurrence in the 81–100 age group at 25.0%. Additionally, S. aureus was detected across all age groups, with the highest proportion in the 1–20 years age group at 18.2%. S. epidermidis was mainly isolated in the 1–20 and 21–40 years age groups. Furthermore, S. saprophyticus was most commonly found in the 1–20 and 21–40 age groups (refer to Table 2).
Gender Distribution of Isolated Organisms Causing UTI Among Study Participants
3.4
This study identified a notable correlation between isolated organisms and gender (p < 0.0001). Candida sp. was predominantly found in females, constituting 17.1%, with no occurrences in males. E. coli, the most prevalent pathogen, was observed in both genders, with a majority of cases in females (51.2%) compared to males (40.0%). Similarly, CONS were more frequently isolated in females (4.7%) than in males (1.8%). P. aeruginosa exhibited a marked gender difference, with a minority of cases in females (2.3%) but a considerably higher prevalence in males (16.4%). K. pneumoniae was present in both genders, with a slightly higher proportion in males (20.0%) compared to females (14.0%). Additionally, Proteus sp. and Providencia sp. were identified in both genders, with a minor gender‐based variation. Proteus sp. was slightly more prevalent in males (1.8%) than in females (0.8%), while Providencia sp. was isolated in females (0.8%) but not in males. Furthermore, S. aureus was detected in both genders, with a slightly higher prevalence in males (12.7%) compared to females (7.8%). S. epidermidis exclusively appeared in males (7.3%), while S. saprophyticus was identified in females (0.8%) and absent in males (see Table 3).
Antibiogram of Bacteria Isolated in This Study
3.5
A total of 19 antibiotics were assessed against various bacterial isolates, encompassing Aminoglycosides (Amikacin [AMI], Gentamicin [GEN]), Fluoroquinolones (Ciprofloxacin [CIP], Ofloxacin [OFL]), Sulfonamides (Trimethoprim/Sulfamethoxazole [SXT]), First Generation Cephalosporins (Cefuroxime [CRX]), Second Generation Cephalosporins (Cefotaxime [CTX]), Third Generation Cephalosporins (Ceftriaxone [CTR], Ceftazidime [CTZ]), Carbapenems (Meropenem [MEM]), Quinolones (Nalidixic Acid [NAL]), Tetracyclines (Doxycycline [DOX], Tetracycline [TET]), Penicillins (Amoxicillin [AMO], Ampicillin [AMP]), Macrolides (Azithromycin [AZI], Erythromycin [ERY]), Vancomycin (VAN), and Chloramphenicol (CMP).
For the seven CONS isolates, 100% resistance was noted against NAL and CMP, followed by a 33.3% resistance against AZI. E. coli exhibited 100% resistance against NAL and OFL, with varying proportions of resistance observed across all other antibiotics, while VAN was the only drug to which E. coli showed 100% sensitivity. Additionally, the single Enterococcus spp. isolate demonstrated 100% resistance to CIP.
Among the 29 K. pneumoniae isolates, substantial proportions were resistant to ERY (100.0%), CTX (90.0%), CIP (81.3%), SXT (80%), CRX (77.8%), AMO (66.7%), TET (66.7%), CMP (50%), and AMP (50%). The two Proteus sp. isolates exhibited 100% resistance to CIP, AZT, AMI, and MEM, and 50% resistance to CTR. However, Proteus sp. showed no resistance to SXT, AMO, and AZI (refer to Table 4).
The single Providencia sp. isolated in this study displayed high resistance against CIP (100.0%), while no resistance was observed against CTZ (0.0%), MEM (0.0%), and AZT (0.0%). Among the 12 P. aeruginosa isolates, significant resistance was observed against NAL (100.0%), DOX (100.0%), AZI (100.0%), CTX (100.0%), CRX (100.0%), SXT (71.4%), CTR (71.4%), and AMI (67.7%). Lower resistance was observed against GEN (28.6%), CIP (40.0%), CTZ (16.7%), MEM (0.0%), AMO (25.0%), and ERY (0.0%). Furthermore, SXT (66.7%), CTZ (100.0%), and TET (87.5%) showed no susceptibility against S. aureus. Among the four S. epidermidis isolates, high resistance was noted against CIP (100.0%), AZI (100.0%), AMP (100.0%), and TET (50.0%). However, no resistance was observed against GEN (0.0%), SXT (0.0%), and CTZ (0.0%). The single S. saprophyticus isolate was 100% resistant to ERY and CTX, but no resistance was observed against SXT (0.0%), AZI (0.0%), and CMP (0.0%) (see Table 5).
Discussion
4
The findings of this study provide important insights into the antibiotic resistance patterns of urinary tract pathogens, highlighting the need for continued monitoring and surveillance of antimicrobial resistance (AMR) in this population. The study analyzed data from 2020 to 2023.
Prevalence of AMR
4.1
One notable finding of this study is the high prevalence of antibiotic resistance among urinary tract pathogens. The results revealed that E. coli exhibited 100% resistance against NAL and OFL, with varying proportions of resistance observed across all other antibiotics, which is consistent with previous studies in the literature [18, 19]. This high rate of antibiotic resistance raises concerns about the effectiveness of commonly used antibiotics for treating UTIs and highlights the need for prudent antibiotic use and appropriate antibiotic stewardship practices in clinical settings.
Another important finding of this study is the emergence of multidrug resistance among urinary tract pathogens. The study identified E. coli, K. pneumoniae, P. aeruginosa, Proteus sp., S. aureus, Enterococcus spp., and S. epidemidis as resistant to three or more classes of antibiotics, indicating a worrisome trend of multidrug resistance. This finding is in line with global concerns about the spread of MDR bacteria, which pose significant challenges for the management of UTIs and other infectious diseases [20, 21].
The study also found variations in antibiotic resistance patterns among different pathogens and over time. For instance, K. pneumoniae showed higher resistance rates to GEN, CIP, and SXT compared to P. aeruginosa (Tables 4 and 5), suggesting differences in the mechanisms and dynamics of antibiotic resistance among different urinary tract pathogens. Moreover, the study revealed changes in antibiotic resistance patterns over time, with some pathogens showing increasing resistance rates during the study period. These findings highlight the dynamic nature of antibiotic resistance and the need for ongoing monitoring and surveillance to detect and respond to changes in resistance patterns.
Several factors may contribute to the high rates of antibiotic resistance observed in this study. These factors may include inappropriate antibiotic prescribing practices, overuse of antibiotics, patient noncompliance with antibiotic regimens, and inadequate infection control measures in healthcare settings. Strategies to address these factors may include implementing antimicrobial stewardship programs, promoting appropriate antibiotic use, educating healthcare providers and patients on antibiotic resistance and prudent antibiotic use, and improving infection control practices in healthcare facilities.
Candida species accounted for 12% of isolates and were included only when laboratory records indicated significant colony counts (> 10⁵ CFU/mL) and associated urinary symptoms, in line with standard diagnostic criteria for fungal UTIs. However, given the retrospective nature of the study and limited clinical details, the possibility of contamination or colonization cannot be excluded. This limitation should be considered when interpreting the prevalence of fungal UTIs in our findings.
Limitations
4.2
There are limitations to this study that should be considered when interpreting the results. First, the study was retrospective in nature and relied on data from medical records, which may be subject to incomplete or inaccurate documentation. Second, the study was conducted in a specific population and setting, which may limit the generalizability of the findings to other populations or settings. Third, the study only focused on antibiotic resistance patterns and did not assess other factors that may contribute to the development of antibiotic resistance, such as antibiotic usage patterns, patient demographics, or environmental factors. We were also unable to perform the year‐by‐year trend analysis. Additionally, important confounding variables, such as prior antibiotic exposure, the presence of urinary catheters, and comorbid conditions (especially T2DM), could not be adequately assessed due to missing or incomplete clinical data. These factors are known to influence both the occurrence of UTIs and the emergence of resistant organisms, and their absence may have affected the interpretation of our findings.
Conclusion
5
This study provides valuable insights into the antibiotic resistance patterns of urinary tract pathogens. The findings highlight the need for continued monitoring and surveillance of AMR, prudent antibiotic use, and appropriate infection control practices in clinical settings. Further research is warranted to better understand the factors contributing to antibiotic resistance and to develop effective strategies to mitigate the spread of antibiotic‐resistant bacteria in UTIs and other healthcare settings.
Author Contributions
Solomon Wireko: conceptualization, investigation, funding acquisition, writing – original draft, methodology, validation, visualization, writing – review and editing, project administration, supervision, resources, data curation. Gifty Ngmaakan: investigation, writing – original draft, methodology, validation, visualization, writing – review and editing, software, data curation, resources. Doreen Dwomoh: investigation, writing – original draft, methodology, validation, visualization, writing – review and editing, software, data curation, resources. Charlotte Hansen: conceptualization, investigation, methodology, validation, visualization, writing – review and editing, project administration, supervision, resources. Sampson Nartey: investigation, writing – original draft, methodology, validation, visualization, writing – review and editing, project administration, supervision, resources. Ebenezer Senu: validation, visualization, writing – review and editing, software, formal analysis, data curation, resources, writing – original draft.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author, Solomon Wireko, affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Z. Zeng , J. Zhan , K. Zhang , H. Chen , and S. Cheng , “Global, Regional, and National Burden of Urinary Tract Infections From 1990 to 2019: An Analysis of the Global Burden of Disease Study 2019,” World Journal of Urology 40, no. 3 (2022): 755–763.35066637 10.1007/s 00345-021-03913-0 · doi ↗ · pubmed ↗
- 2S. Von Vietinghoff , O. Shevchuk , U. Dobrindt , et al., “The Global Burden of Antimicrobial Resistance–Urinary Tract Infections,” Nephrology Dialysis Transplantation 39 (2023): 581–588.10.1093/ndt/gfad 23337891013 · doi ↗ · pubmed ↗
- 3G. Mancuso , A. Midiri , E. Gerace , M. Marra , S. Zummo , and C. Biondo , “Urinary Tract Infections: The Current Scenario and Future Prospects,” Pathogens 12, no. 4 (2023): 623.37111509 10.3390/pathogens 12040623 PMC 10145414 · doi ↗ · pubmed ↗
- 4F. M. E. Wagenlehner , T. E. Bjerklund Johansen , T. Cai , et al., “Epidemiology, Definition and Treatment of Complicated Urinary Tract Infections,” Nature Reviews Urology 17, no. 10 (2020): 586–600.32843751 10.1038/s 41585-020-0362-4 · doi ↗ · pubmed ↗
- 5P. Behzadi , E. Urbán , M. Matuz , R. Benkő , and M. Gajdács , “The Role of Gram‐Negative Bacteria in Urinary Tract Infections: Current Concepts and Therapeutic Options,” Advances in Experimental Medicine and Biology 1323 (2021): 35–69.32596751 10.1007/5584_2020_566 · doi ↗ · pubmed ↗
- 6C. C. Y. Chieng , Q. Kong , N. S. Y. Liou , R. Khasriya , and H. Horsley , “The Clinical Implications of Bacterial Pathogenesis and Mucosal Immunity in Chronic Urinary Tract Infection,” Mucosal Immunology 16 (2023): 61–71.36642381 10.1016/j.mucimm.2022.12.003 · doi ↗ · pubmed ↗
- 7I. Ambite , D. Butler , M. L. Y. Wan , et al., “Molecular Determinants of Disease Severity in Urinary Tract Infection,” Nature Reviews Urology 18, no. 8 (2021): 468–486.34131331 10.1038/s 41585-021-00477-x PMC 8204302 · doi ↗ · pubmed ↗
- 8G. Daryabor , M. R. Atashzar , D. Kabelitz , S. Meri , and K. Kalantar , “The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System,” Frontiers in Immunology 11 (2020): 1582.32793223 10.3389/fimmu.2020.01582 PMC 7387426 · doi ↗ · pubmed ↗