Rapid evaporative ionization mass spectrometry in surgery: a systematic review
Angus R J Barber, Alexander Dottore, James Leigh, Mark Fear, Fiona Wood

TL;DR
This paper reviews the use of a new mass spectrometry technique in surgery for real-time tissue identification, highlighting its potential and current limitations.
Contribution
A systematic review of 26 studies on REIMS applications in surgery, summarizing outcomes and identifying research gaps.
Findings
REIMS shows promising accuracy, sensitivity, and specificity for cancerous tissue identification.
Most studies used ex vivo applications, with limited in vivo data reported.
Logistical challenges and data interpretation complexity remain significant barriers to widespread use.
Abstract
Rapid evaporative ionization mass spectrometry (REIMS) is an emerging technology facilitating real-time intraoperative tissue identification during surgery. This review aims to discuss the applications and reported outcomes of REIMS technology in a surgical context. A systematic review was performed using four electronic databases that were searched in August 2025: MEDLINE, Emcare, Embase, and Web of Science. Eligible studies were peer-reviewed, included five or more patients, and evaluated REIMS technology in the context of a surgical specialty or pathology. Two independent reviewers screened studies, extracted data, and assessed risk of bias using the QUADAS-2 tool. The study protocol was registered in the PROSPERO international prospective register of systematic reviews before commencing the review (CRD42024546741). A total of 344 records underwent initial screening, with 26…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
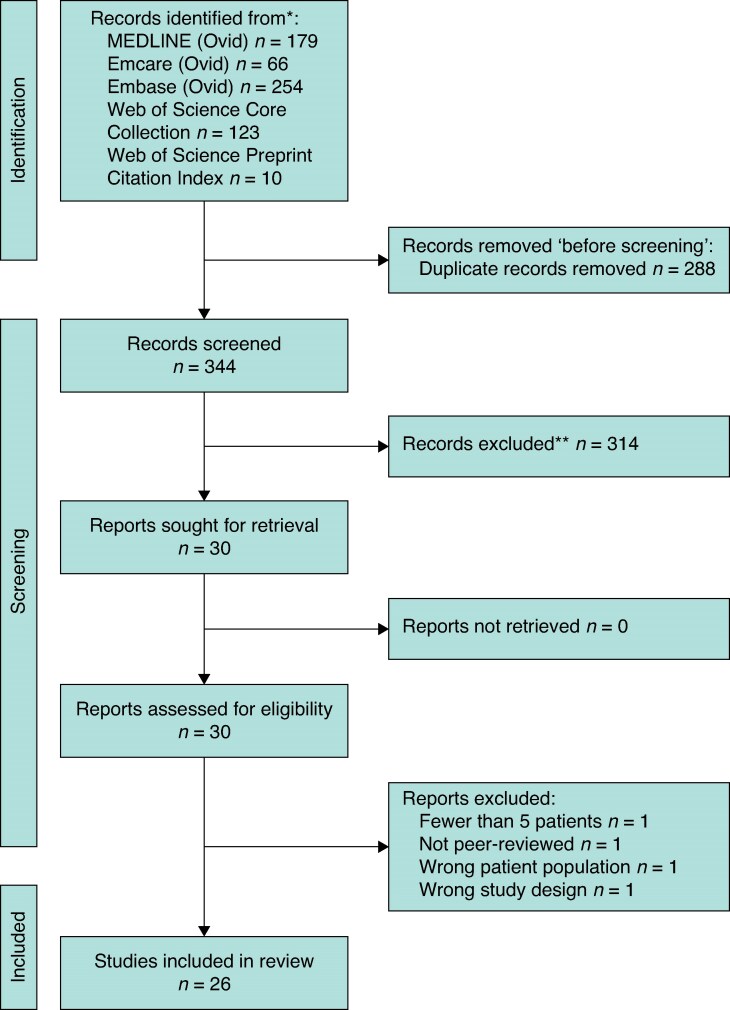 Fig. 1
Fig. 1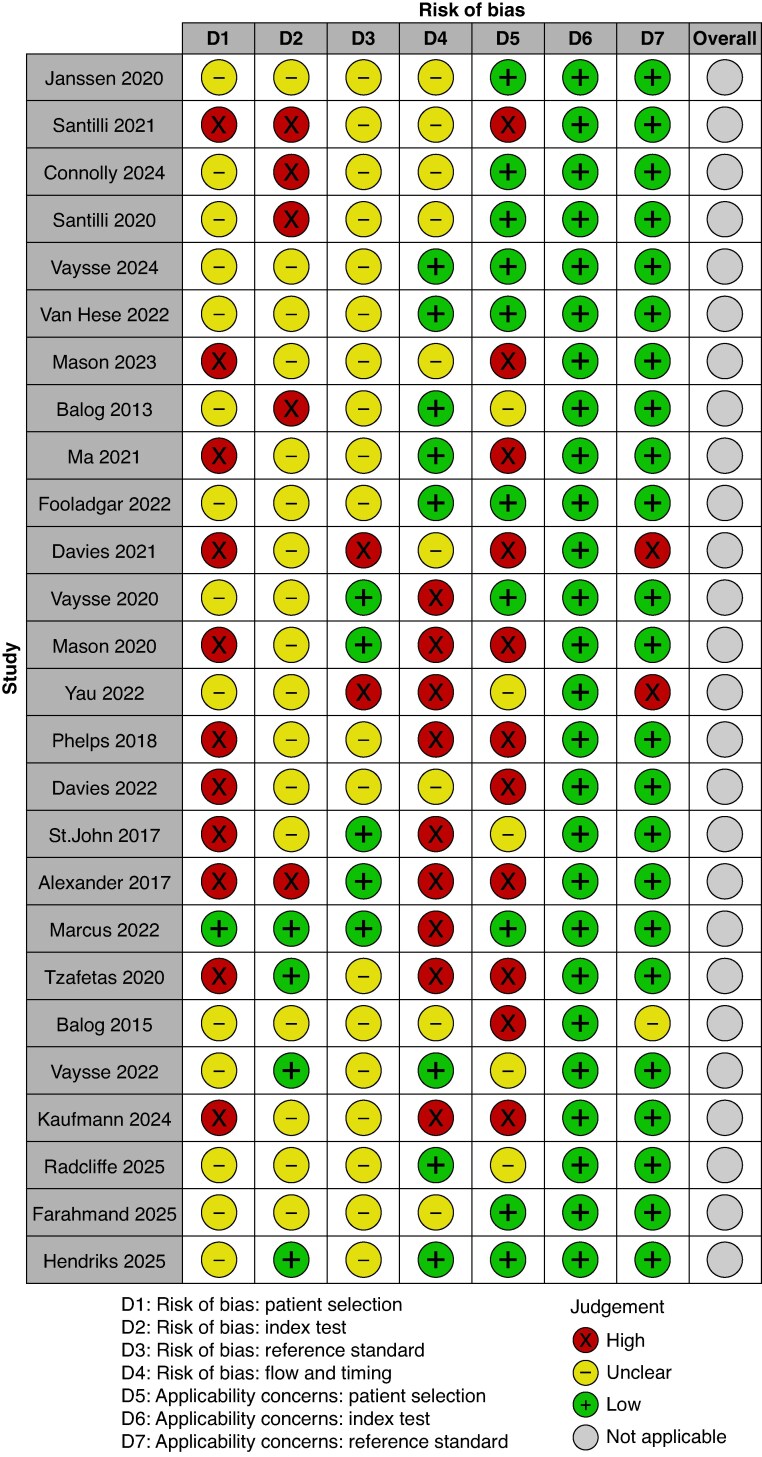 Fig. 2
Fig. 2| Screening reviewer A | Screening reviewer B | Cohen’s κ coefficient | |
|---|---|---|---|
| Title and abstract screening | Full-text screening | ||
| A.R.J.B. | A.D. | 0.94604 | 1.0 |
| Reference and year | Surgical specialty | Disease process | Study design | Data interpretation model | Data set size | Model validation | Reported qualitative outcomes | Reported quantitative outcomes |
|---|---|---|---|---|---|---|---|---|
| Janssen | Plastic surgery | BCC |
| PCA-LDA | 596 spectra | Five-fold cross-validation | Intraoperative ( |
|
| Santilli | Plastic surgeryGeneral surgery | BCCBreast cancer |
| SSL using ‘relative patch algorithm’ | 464 spectra | Four-fold cross-validation | An SSL task (learning from BCC data and applying this to breast cancer data) suggests shared features between skin and breast data | For the model trained with skin data and validated on breast cancer data, accuracy was 92.7%, sensitivity 88.5%, specificity 96.4%, AUC 92.7% |
| Connolly | Plastic surgery | BCC |
|
- MLP- PCA-LDA- BNN- Experimental model (involving GADF, GASF, MTF) | 11 100 spectra | Five-fold cross-validation | Of the non-experimental models used to analyse data, BNN was the highest performing modelTransforming iKnife signals into images and using self-supervision may outperform traditional modelsFatty acids and glycerophospholipids showed differential abundance between cancerous and benign tissue |
|
| Santilli | Plastic surgery | BCC |
|
- PCA-LDA- Experimental model (deep learning network with modified symmetrical autoencoder architecture) | 190 spectra | Four-fold cross-validation | Insufficient smoke or low-intensity signals make it more difficult to predict sample classVariations in mass spectra can occur due to depth of burn or body site of tissueIf sub-band analysis is applied, the range of 500–900 m/z yields the best accuracy differentiating normal | PCA-LDA model:- Accuracy 85.1%, sensitivity 72.9%, specificity 91.0%Augmentation of PCA-LDA model data improved mean performanceDeep learning model means: accuracy 96.6%, sensitivity 100%, specificity 95% |
| Vaysse | Surgical oncology | Soft tissue sarcoma |
| PCA-LDA | 1200 spectra | Leave-one-patient-out cross-validation | Fatty acids, phospholipids, and cardiolipin were predominant in cut mode; triacylglycerols were predominant in coagulate mode | With cut and coagulate mode data combined, sarcoma tissue was correctly classified 98.2% of the time, normal tissue correctly classified 98.6% of the time, overall classification rate 95.5% |
| Van Hese | Neurosurgery | Glioma |
| PCA-LDA | 124 spectra | Five-fold cross-validation | Glycophospholipids, phosphatidic acids, sphingolipids, and fatty acids were identified as contributing to class separationDifferences between classes due to different mass peak ratios, rather than the presence or absence of specific lipid speciesA monopolar model was applicable to bipolar electrocautery | Overall accuracy of 87.9% for a model including classes: normal, astrocytoma grade 2, astrocytoma grade 3, glioblastoma, oligodendroglioma grade 2, oligodendroglioma grade 3In high-grade gliomas, overall correct classification rate 97.0%, with 99.3% sensitivity and 100% specificity. For margin detection, bulk glioblastoma tumour was identified as 100% glioblastoma, normal brain as 0% glioblastoma, and the invasive region (margin) was detected as 10% glioblastoma via REIMS, which was histopathologically quantified as 10.7% glioblastoma cells |
| Mason | General surgery | Colorectal cancer |
|
- PCA-LDA- OPLS-DAUnivariate method:- ANOVA | 1013 spectra | Leave-one-patient-out cross-validation | No single lipid metabolite is capable of acting as a biomarker of disease and comparisons require multivariate modelling to assess differences in relative abundanceRelative abundance of lipids by subclass increases at initiation of adenoma formation (except phosphatidylcholines, which decrease). Abundance of phosphatidylglycerols increases throughout carcinogenesisBased on the mucosal lipidome, REIMS was able to predict the presence of nodal metastasis with the same NPV as preoperative cross-sectional imaging (78.0% with REIMS | REIMS identified colorectal carcinoma with accuracy of 91.1%, sensitivity 86.4%, specificity 95.4%, PPV 90.7%, NPV 93.1%One source of misclassifications were adenomas predicted to be carcinomas. Clinically both adenomas and carcinomas require excision, so if considered as one group accuracy increases to 93.5%, sensitivity 91.2%, specificity 96.7%, PPV 97.5%, NPV 88.6% |
| Balog | Surgery in general | Various subtypes of cancer |
| PCA-LDAUnivariate method:- Kruskal–Wallis test | 2933 spectra | Leave-one-patient-out cross-validation | It is the profile of lipid species rather than any specific biomarker that accounts for histological specificityREIMS was able to identify the origin of metastatic tumours both |
|
| Ma | Neurosurgery | Glioblastoma multiforme |
|
- PCA- PLS-DA | Not stated | Not stated | A difference in lipid composition between tumour and control samples was identified. Most lipids showed higher intensities in tumour group, which is consistent with increased lipogenesis in tumour cells | REIMS showed overall accuracy of 94.7%, sensitivity of 95.4%, specificity 93.3%, and AUC 0.968 |
| Fooladgar | Plastic surgery | BCC |
|
- PCA-LDA- BNN model- A deep model (similar to BNN, but without Bayesian output and uncertainty estimation) | 693 spectra | Not stated | A model with higher sensitivity that detects all cancer at margins is preferredPCA-LDA is not improved by uncertainty filtering, but applying uncertainty filtering to BNN models improves model accuracy | PCA-LDA:Accuracy 69.7%, sensitivity 66.0%, specificity 73.5%, AUC 73.9%BNN model with uncertainty filtering: 75.2% balanced accuracy, 74.1% sensitivity, 77.3% specificity, 82.1% AUCExcluding highly uncertain samples from decision-making can improve decisions and overall sensitivity (88.2% sensitivity if 20% of highly uncertain spectra rejected) |
| Davies | Vascular surgery | Aortic aneurysm |
| PLS-DA | Not stated | Two-fold cross-validation | Patient sex and source of normal tissue (cadaveric | REIMS was able to discriminate between normal and aneurysmic aortic tissue with 88.7% mean accuracy and 85.1% mean precision using a second generation model |
| Vaysse | General surgery | Breast cancer |
| PCA-LDA | 689 spectra | Leave-one-patient-out cross-validation | The main discriminators of class were triglycerides for adipose tissue and fatty acids, palmitic acid, and oleic acid for stroma |
|
| Mason | General surgery | Rectal cancer |
|
- PCA- OPLS-DAUnivariate method:- ANOVA | 266 spectra | Leave-one-patient-out cross-validation | PCA demonstrated no clustering based on sex, age, or resection type (radical |
|
| Yau | Plastic surgery | Burns |
|
- PCA- OPLS-DA | 109 spectra | Not stated | Excised burn tissue showed significantly lower concentrations of free fatty acids, monoacylglyceride, lysophosphatidylglycerol, and lysophosphatidylethanolamineConcentrations of lactosylceramide and cholesterol esters were significantly higher in excised burn tissue compared with control tissueThere is a difference in lipid profiles between excised burn skin and control skin | REIMS showed distinct separation between burn tissue and control tissue, with AUC 1.0, sensitivity 100%, and specificity 100% |
| Phelps | Gynaecology | Ovarian cancer |
| PCA-LDAUnivariate methods:- Wilcoxon’s rank-sum- Kruskal–Wallis test | 3387 spectra | Leave-one-patient-out cross-validation | The three most significant MS peaks contributing to separation of ovarian cancer from normal samples were various forms of phosphatidic acid and phosphatidylethanolamine. These peaks were higher in ovarian cancer tissue | Ovarian cancer |
| Davies | Cardiothoracic and vascular surgery | Type A aortic dissection |
|
- PCA- PLS-DAUnivariate method:- Dunn Kruskal–Wallis test | Not stated | Two-fold cross-validation | PCA analysis showed separation between true lumen wall | REIMS was able to discriminate false lumen wall tissue from other tissue types with 72.4% accuracy and 69.3% precision |
| St John | General surgery | Breast cancer |
| PCA-LDAUnivariate method:- Mann–Whitney | 359 spectra | Leave-one-patient-out cross-validation | Normal tissue demonstrated high-intensity spectra in the phospholipid and triglyceride range using cut mode and predominantly in triglyceride range when using coagulate modeTumour tissue has increase in phospholipid and decrease in triglyceride range in both cut and coagulate modesPhospholipid species elevated in cancer ( |
|
| Alexander | General surgery | Colorectal cancer |
| PCA-LDAUnivariate method:- ANOVA | 104 spectra | Leave-one-patient-out cross-validation | Cancerous tissue overexpressed long-chain phosphatidylserines and bacterial phosphatidylglycerolsWhen data were modelled against age and sex, it was not possible to build a strong predictive model for these factors (that is these factors did not significantly influence REIMS). However, males and patients >70 years old did demonstrate clusteringAnatomically, rectal samples were distinctly clustered from remaining colonic specimens, suggesting a discrete mucosal lipidome | Normal mucosa |
| Marcus | Gynaecology | Endometrial cancer |
| PCA-LDAUnivariate method:- Kruskal–Wallis test | 453 spectra | Leave-one-patient-out cross-validation | Larger sample size PCA-LDA improved diagnostic accuracyEndometrial cancer had up-regulated ceramides and phospholipids (phosphatidic acid, phosphatidylethanolamines, and phosphatidylserines) | Endometrial cancer |
| Tzafetas | Gynaecology | Cervical cancer |
|
- LASSO- LDAUnivariate method:- ANOVA | 209 spectra | Leave-one-patient-out cross-validation | MS peaks contributing to separation of cancer | A REIMS model classifying normal |
| Balog | General surgery | Gastrointestinal cancer |
| PCAUnivariate method:- Kruskal–Wallis test | 186 spectra | Leave-one-patient-out cross-validation | Gastric mucosa (both healthy and adenocarcinoma) featured phospholipids in 600–900 m/z range, whilst submucosa featured triglyceride and phosphatidylinositol species in 850–1000 m/z range |
|
| Vaysse | Ear, nose, and throat | Oral squamous cell carcinoma |
| PCA-LDA | 185 spectra | Leave-one-patient-out cross-validation | Metabolic profiles for soft tissue and tumour showed distinctive profiles | REIMS was capable of detecting 10% tumour cells in a sample with 83% sensitivity and 82% specificity. By detecting a small proportion of tumour cells in a sample, REIMS may assist with tumour margin recognition in highly infiltrative malignancy |
| Kaufmann | General surgery | Breast cancer |
| PCA-LDA | 260 spectra |
- Leave-one-patient-out cross-validation- Leave-one-site-out cross-validation- Five-fold cross-validation | Triglycerides dominated the spectra acquired from normal tissue, but were mostly absent from tumour tissue spectra. Tumour spectra had a relatively high abundance of phospholipidsCosine similarities between cancerous tissue tested was lower than normal adipose tissue, especially in coagulate modeCertain triglycerides are distinctly elevated in coagulate modeMetabolism of linoleic acid was enhanced in triple-negative breast cancer compared with ER/PR-positive cancer | Model using a training set from two sites and testing it on a third site, with leave-one-patient-out cross-validation: 98.6% correct classification rate, 2.8% false negative, 0.7% false positiveIf a more targeted model based on 11 selected metabolites is applied, correct classification rate is 98%. This may decrease the impact of spectral variability on classification |
| Radcliffe | General surgery | Breast cancer |
|
- iForest- OC-PCA- GODS- KGODS | 2149 spectra | Four-fold cross-validation | Incorporating healthy | For models trained on intraoperative data only:- iForest: balanced accuracy 70.2%, sensitivity 90.9%, specificity 49.4%- OC-PCA: balanced accuracy 81.0%, sensitivity 90.9%, specificity 71.0%- GODS: balanced accuracy 77.1%, sensitivity 67.9%, specificity 86.4%- KGODS: balanced accuracy 80.6%, sensitivity 79.4%, specificity 81.8%For models trained on intraoperative and healthy |
| Farahmand | Plastic surgery | BCC |
|
- PCA-LDA- MLP- Foundation model for assessing cancer tissue margins (FACT) | 11 100 spectra | Three-fold cross-validation | There is correlation between misclassified specimens and sample noise | PCA-LDA model: balanced accuracy 69.7%, sensitivity 66.0%, specificity 73.5%MLP model: balanced accuracy 73.9%, sensitivity 67.8%, specificity 79.9%FACT model: balanced accuracy 77.5%, sensitivity 72.2%, specificity 82.8% |
| Hendriks | Neurosurgery | Glioblastoma multiforme |
| PCA-LDA | 87 spectra | Five-fold cross-validation | Metabolite patterns differed between patients with short-term survival | PCA-LDA model correctly classified 97.7% of samples into short term (0–12 months) |
| Reference | Year | Substances contributing to class separation |
|---|---|---|
| Connolly | 2024 | Fatty acids and glycerophospholipids |
| Van Hese | 2022 | Glycophospholipids, phosphatidic acids, sphingolipids, and fatty acids |
| Mason | 2023 | Relative abundance of lipids by subclass increases at initiation of adenoma formation (except phosphatidylcholines, which decrease). Abundance of phosphatidylglycerols increases throughout carcinogenesis |
| Vaysse | 2020 | Triglycerides for adipose tissue. Fatty acids, palmitic acid, and oleic acid for stroma |
| Yau | 2022 | Burn tissue showed higher concentrations of lactosylceramide and cholesterol esters compared with control tissue, and lower concentrations of free fatty acids, monoacylglyceride, lysophosphatidylglycerol, and lysophosphatidylethanolamine |
| Phelps | 2018 | Various forms of phosphatidic acid and phosphatidylethanolamine were higher in ovarian cancer tissue |
| Davies | 2022 | Glycosaminoglycans |
| St John | 2017 | Tumour tissue has increase in phospholipid (specifically glycerophospholipids) and decrease in triglyceride range in both cut and coagulate modes |
| Alexander | 2017 | Cancerous tissue overexpressed long-chain phosphatidylserines and bacterial phosphatidylglycerols |
| Marcus | 2022 | Endometrial cancer had up-regulated ceramides and phospholipids (phosphatidic acid, phosphatidylethanolamines, and phosphatidylserines) |
| Tzafetas | 2020 | Sphingomyelins, phosphatidic acids, phosphatidylethanolamines, phosphatidylglycerols, phosphatidylcholine, and phosphatidylinositols |
| Kaufmann | 2024 | Triglycerides dominated spectra acquired from normal tissue, but were mostly absent from tumour spectra. Tumour had high abundance of phospholipidsMetabolism of linoleic acid was enhanced in triple-negative breast cancer compared with oestrogen receptor/progesterone receptor-positive breast cancer |
| Hendriks | 2025 | Short-term survival patients: more abundant oleic acid and palmitic acidProlonged survival patients: more abundant linoleic acid and stearic acid |
| Reference | Year | Setting of data | Accuracy | Sensitivity | Specificity |
|---|---|---|---|---|---|
| Janssen | 2020 |
| PCA-LDA model: 92% | PCA-LDA model: 86% | PCA-LDA model: 97% |
|
| PCA-LDA model: 50% | ||||
| Santilli | 2021 |
| SSL model: 92.7% | SSL model: 88.5% | SSL model: 96.4% |
| Connolly | 2024 |
|
- MLP model: 73.8%- PCA-LDA model: 69.7%- BNN model: 72.1%- Experimental model: 73.5% |
- MLP model: 59.4%- PCA-LDA model: 66.0%- BNN model: 60.5%- Experimental model: 63.1% |
- MLP model: 83.7%- PCA-LDA model: 73.5%- BNN model: 83.7%- Experimental model: 83.9% |
| Santilli | 2020 |
|
- PCA-LDA model: 85.1%- Experimental model: 96.6% |
- PCA-LDA model: 72.9%- Experimental model: 100% |
- PCA-LDA model: 91%- Experimental model: 95% |
| Vaysse | 2024 | Not specified | PCA-LDA model: 95.5% | ||
| Van Hese | 2022 |
| PCA-LDA model: 87.9% for all classes, 97.0% for high-grade gliomas | PCA-LDA model: 99.3% for high-grade gliomas | PCA-LDA model: 100% for high-grade gliomas |
| Mason | 2023 |
| PCA-LDA + OPLS-DA model: 91.1% | PCA-LDA + OPLS-DA model: 86.4% | PCA-LDA + OPLS-DA model: 95.4% |
| Balog | 2013 |
| PCA-LDA model: 96.2% | PCA-LDA model: 97.7% | PCA-LDA model: 96.5% |
| Ma | 2021 |
| PCA + PLS-DA model: 94.7% | PCA + PLS-DA model: 95.4% | PCA + PLS-DA model: 93.3% |
| Fooladgar | 2022 |
|
- PCA-LDA model: 69.7%- BNN model: 75.2% |
- PCA-LDA model: 66.0%- BNN model: 74.1% |
- PCA-LDA model: 73.5%- BNN model: 77.3% |
| Davies | 2021 |
| PLS-DA model: 88.7% | ||
| Vaysse | 2020 |
| PCA-LDA model: 92.6% | ||
| Mason | 2020 |
| PCA + OPLS-DA model: 86.8% for all classes, 91.4% for normal | PCA + OPLS-DA model: 94.2% for all classes, 89.7% for normal | PCA + OPLS-DA model: 91.7% for all classes, 93.4% for normal |
|
| PCA + OPLS-DA model: 90% accuracy identifying involved margins | ||||
| Yau | 2022 |
| PCA + OPLS-DA model: 100% | PCA + OPLS-DA model: 100% | |
| Phelps | 2018 |
| PCA-LDA model: 97.6% | PCA-LDA model: 97.4% | PCA-LDA model: 100% |
| Davies | 2022 |
| PCA + PLS-DA model: 72.4% | ||
| St John | 2017 |
| PCA-LDA model: 95.8% | PCA-LDA model: 90.9% | PCA-LDA model: 98.8% |
| Alexander | 2017 |
| PCA-LDA model: 90.5% for normal mucosa | PCA-LDA model: 86.7% for normal mucosa | PCA-LDA model: 92.4% for normal mucosa |
| Marcus | 2022 |
| PCA-LDA model: 86% | PCA-LDA model: 81% | PCA-LDA model: 91% |
| Tzafetas | 2020 | Not specified | LASSO + LDA model: 100% | LASSO + LDA model: 100% | LASSO + LDA model: 100% |
| Balog | 2015 |
| PCA model: 88.5% | PCA model: 95% | |
| Vaysse | 2022 |
| PCA-LDA model: 96.8% | PCA-LDA model: 83% for detecting 10% tumour cells in a sample | PCA-LDA model: 82% for detecting 10% tumour cells in a sample |
| Kaufmann | 2024 |
| PCA-LDA model: 98.6% with leave-one-patient-out cross-validation | ||
| Radcliffe | 2025 |
| Models trained on intraoperative and healthy | Models trained on intraoperative and healthy | Models trained on intraoperative and healthy |
| Farahmand | 2025 |
| PCA-LDA model: 69.7%MLP model: 73.9%FACT model: 77.5% | PCA-LDA model: 66.0%MLP model: 67.8%FACT model: 72.2% | PCA-LDA model: 73.5%MLP model: 79.9%FACT model: 82.8% |
| Hendriks | 2025 |
| PCA-LDA model: 97.7% |
- —Fiona Wood Foundation10.13039/501100022218
- —Ian Potter Foundation10.13039/501100001047
- —Fire Protection Australia
- —Australian Government Research Training Programme
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMass Spectrometry Techniques and Applications · Ion-surface interactions and analysis · X-ray Spectroscopy and Fluorescence Analysis
Introduction
Many surgical specialties and procedures aim to remove abnormal or damaged tissue and leave behind healthy residual tissue. Identification of abnormal or damaged tissue is usually obtained by histopathological examination. This process takes somewhere from hours to days and results are prone to subjective interpretation^1^. If tissue identification is required intraoperatively, modalities such as squash smear cytology, frozen sections, and fluid cytology may be employed to provide a preliminary diagnosis^2^. This preliminary diagnosis can then inform further surgical decision-making intraoperatively. Although frozen sections shorten the timeframe for a preliminary diagnosis, taking 20–30 min^1^, they are prone to errors that can have an adverse impact on intraoperative management^3^. Ideally, intraoperative tissue identification methods should be rapid, standardized, and diagnostically accurate^4^. Rapid evaporative ionization mass spectrometry (REIMS) is a relatively new technology that poses as a potential solution to many of the current problems with intraoperative tissue identification^1^.
Diathermy is a common surgical tool used to cut, coagulate, and achieve haemostasis^5^. It functions by passing electrical current, in different waveforms, through tissues. The resistance of the tissues results in heat production^6^ and heat vaporizes the tissue to produce surgical smoke^7^. The evaporation of biological tissues produced by diathermy heat is rich in molecular ions, such as phospholipids, which can then be analysed with a mass spectrometer^8^. The mass spectrometric profile produced by using diathermy on tissue allows for tissue identification data comparable to histopathological analysis^1^. Coupling of the electrosurgical unit (diathermy) with REIMS technology is termed the ‘intelligent knife’ (iKnife)^9^.
REIMS technology has a growing body of evidence demonstrating successful applications in the surgical field. This systematic review aims to discuss the uses, advantages, disadvantages, and reported outcomes of REIMS technology for intraoperative tissue identification in surgical practice. In doing so, it will identify areas that would benefit from further research and improve awareness among the surgical community.
Methods
The study protocol was designed with reference to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols Statement (PRISMA-P)^10^ and the associated explanation document^11^. The protocol was registered in the PROSPERO international prospective register of systematic reviews before commencing the review (CRD42024546741)^12^. The manuscript has been developed in line with the PRISMA statement, with the PRISMA checklist included in the Supplementary material^13^.
Search strategy and inclusion criteria
A robust search strategy (see the Supplementary material) was designed in collaboration with an experienced research librarian (Cheryl Hamill) and peer-reviewed by another (Glynis Jones). A search of MEDLINE (Ovid) 1946 to current, Emcare (Ovid) 1995 to current, Embase (Ovid) 1974 to current, and Web of Science (Clarivate) 1997 to current was performed on 7 August 2025. The start date for each database search is based on the commencement date of the database itself. The search strategy prioritized sensitivity for maximum retrieval of relevant records, using a combination of free-text (keyword) and thesaurus terms. No grey literature searching was performed and no limits were applied to the search. After deduplication of references, 344 citations were identified, to which the inclusion and exclusion criteria were applied.
Inclusion criteria
Studies published in peer-reviewed journals ANDFull texts available in any language, but with adequate English translation ANDThe study design is RCT OR non-randomized study of intervention OR observational studies (case-control study OR cohort study) OR case series with ≥5 patients ANDThe study evaluates the use of REIMS/iKnife technology in surgery/a surgical environment or application to a surgical pathology ANDREIMS is used on humans or human tissue (both in vivo and ex vivo)
Exclusion criteria
Studies that were case reports OR case series with <5 patients OR literature reviews OR conference abstracts ORStudies without adequate full-text English translation ORStudies evaluating REIMS/iKnife technology in a non-surgical environment and application to a non-surgical pathology ORAnimal studies
Data extraction and variables
After completion of the literature search, studies were uploaded to Covidence systematic review software^14^ for title/abstract and full-text screening. A data extraction template (see the Supplementary material) was designed and piloted by the authors before the extraction process. For both title/abstract and full-text screening, two authors (A.R.J.B. and A.D.) screened studies independently in duplicate, with a third author (J.L.) arbitrating the decision if disagreement occurred. The level of inter-reviewer agreement during title/abstract and full-text screening is summarized using Cohen’s κ coefficient. Data extraction was also performed in duplicate by two of A.R.J.B., A.D., and J.L., with arbitration by the third author in cases of disagreement.
Study risk-of-bias assessment
Included studies were all assessed for risk of bias. This assessment occurred at the study level, by two independent reviewers, and in the case of disagreement was arbitrated by discussion amongst authors. The QUADAS-2 tool^15^ was used to assess risk of bias, given the included articles evaluated the diagnostic accuracy of REIMS analysis.
Synthesis methods
Given the variety of pathologies, surgical specialties, study designs, and data interpretation models applied to REIMS, studies were not deemed homogenous enough to conduct a meta-analysis. Indeed, pooling data from diverse non-randomized studies into a meta-analysis is not recommended^16^. As such, a systematic, qualitative narrative synthesis has been performed. Information from included studies has been presented in tables, as well as within the manuscript text, to explain their characteristics and findings.
Results
Study screening
- illustrates the process of screening using a PRISMA flow diagram^13^. The screening process was performed using Covidence software. A total of 344 records were identified after deduplication and underwent title and abstract screening, of which 30 articles progressed to full-text screening. A total of 26 studies then met the inclusion criteria and were included in this systematic review.
PRISMA flow diagram detailing the literature search process used to identify included studies
The level of agreement between investigators during title/abstract and full-text screening (assessed using Cohen’s κ coefficient) is shown in Table 1. This process demonstrated almost perfect agreement^17^ in both title/abstract and full-text screening.
Study characteristics and results of individual studies
A total of 26 studies met the inclusion criteria and were included in the review. Studies originated from seven countries (Canada^18–25^, the Netherlands^26–29^, Belgium^30^, the UK^31–39^, Hungary^9^, China^40^, and Australia^41^). One study did not specify the country of origin^42^. Included studies were published between 2013 and 2025. REIMS was applied to eight surgical specialties, of which the most common was general surgery (9 studies), followed by plastic surgery (7 studies). Twenty-three of the included studies discussed REIMS in the context of cancer, with the most frequently studied pathology being basal cell carcinoma (BCC), which was the subject of six papers.
Of the 26 included studies, 14 used both ex vivo and in vivo data, whilst the remaining 12 used ex vivo data only. Twenty-two studies prospectively collected data, whilst one was both retrospective and prospective, and three studies were retrospective.
As a ‘gold standard’ comparator for REIMS analysis, 23 studies relied on histopathological analysis to determine the performance of REIMS. Davies et al.^32^ used previously reported biomechanical and biochemical variables for comparison. Yau et al.^41^ compared REIMS analysis of burn tissue with the intraoperative judgement of a burns surgeon. Hendriks et al.^29^ used confirmed overall survival data for included patients.
Among included studies, a total of 1825 patients contributed to the analysis. Two included studies^40,41^ did not specify the number of patients, but instead reported the number of samples, which contributed an additional 78 tissue samples. One included study^25^ reported patient numbers for the ex vivo component of the study (91 patients), but reported sample numbers for the in vivo data (43 resections). Of the 23 studies reporting complete patient numbers, 1302 patients were analysed ex vivo, 54 were analysed in vivo, and for 484 patients it was not specified if their analysis occurred ex vivo or in vivo. A number of studies analysed a large number of ex vivo patients and then applied this data set to analyse a smaller number of in vivo patients as a proof of concept.
Of the 26 included studies, two articles^39,41^ made their data available via a public repository and a further five articles^24,27–29^ ^,31^ had data attached in the Supplementary material of the paper. Eight papers^9,26,32,34–36,38,40^ made data available on request by contacting the corresponding author. There were ten articles without any data availability statement, which also did not include any data in the Supplementary material. One article stated data from the study were not available.
Study characteristics and findings are summarized in Table 2.
Risk of bias in included studies
The 26 included studies were assessed for risk of bias using the QUADAS-2 tool^15^ by two independent reviewers and in the case of disagreement was arbitrated by discussion amongst authors. QUADAS-2 was chosen because the vast majority of included studies commented on the diagnostic accuracy of REIMS in identifying tissue types. Among artificial intelligence (AI)-based diagnostic accuracy studies, QUADAS-2 is the most commonly used risk-of-bias assessment tool^43^. It is acknowledged that there are significant limitations with this tool when applied to AI diagnostic studies. AI diagnostic accuracy studies can cause issues within all four domains of QUADAS-2^43^, but, specifically in the case of REIMS, reporting on the ‘flow and timing’ category may unfairly determine a high risk of bias. A common methodology amongst REIMS analyses is to perform cross-validation, where a proportion of available data is intentionally left out from the model-training process and left available for model testing/validation at a later stage. As such, there is scope for this to be interpreted as all patients not being included in the analysis, which would contribute to a high risk of bias in the ‘flow and timing’ category. Consequently, in this study, a concerted effort was made to not penalize studies for this, so when studies excluded patients from model training, but later included them in model testing, this was not considered to be a high risk of bias. An AI-specific extension to QUADAS-2 has been recommended^44^, but is not yet available, limiting quality assessment to existing tools.
The robvis tool^45^ was used to create a visual representation of study risk of bias and this is presented in Fig. 2. This assessment demonstrated significant risk of bias among most of the included studies, suggesting the need for further high-quality research into REIMS technology. A number of studies did not comment on how their patient cohort was selected (for example, consecutive or random patients), making the patient selection domain unclear. Many studies did not include all recruited patients in the final analysis, resulting in a high risk of bias in the ‘flow and timing’ category. This was often on account of poor spectral quality or high background noise, leading to exclusion of the affected spectra from analysis.
QUADAS-2 risk-of-bias assessment for included studies
Results of synthesesReported qualitative outcomes
Statistical methods used for REIMS analysis
REIMS analysis generates a large amount of molecular data, which must then be classified using predictive statistical methods. This allows for allocation of the data points to a particular class, for example normal or cancerous tissue. Both univariate and multivariate statistical methods can be employed to analyse REIMS data. A univariate analysis looks at each variable in isolation and, in the context of mass spectrometry, univariate models are often applied to determine relevant ‘information-rich’ features of the data set^46^. A common application for univariate methods in REIMS is to determine metabolites responsible for class discrimination^33,34^, for example determining peaks that differ between normal and cancerous tissue^36^. Univariate analyses may work to reduce the number of features considered in a subsequent multivariate model, by focusing on those showing statistical significance in initial univariate tests^46^.
Multivariate analysis incorporates all variables simultaneously and assesses relationships among them^47^. A multivariate classification method may be supervised or unsupervised. Unsupervised methods uncover general structural patterns and relationships within a data set, helping develop hypotheses and explore data sets without predefined data labelling^48^. Supervised methods require data to be labelled and summarize variables in a way that explains their relationship with another variable^49^. In the context of REIMS, unsupervised analyses such as principal component analysis (PCA) are often initially applied for data reduction, to obtain an overview of the variance of metabolic profiles^28^. PCA reduces the number of observed variables into a smaller number of principal components, which account for the majority of variance in the data set^37^. This helps interpret a large complex metabolomic data set^50^. Subsequent supervised analyses such as linear discriminate analysis (LDA) are then used to maximize the separation between different classes, allowing classification of the data^37,51^. Implementing both univariate and multivariate analysis methods in mass spectrometry is recommended to optimize the relevant data extracted from a data set^46^.
Ten studies reported using univariate statistical methods for data analysis. These were primarily implemented to identify differential peaks between normal and pathological tissue. The most commonly implemented methods were the Kruskal–Wallis test and ANOVA. ANOVA is used to compare the means of three of more independent data sets that meet the parametric assumptions, whilst the Kruskal–Wallis test is the equivalent test for data sets that do not meet parametric assumptions^52^. The decision to apply parametric or non-parametric methods to REIMS data should be made after considering if the data set meets the parametric assumptions or not^46^.
Among included articles, 17 different multivariate statistical methods were applied for REIMS analysis. Seventeen studies utilized a PCA-LDA model of analysis and a further five articles used PCA without LDA as a component of their model. Although PCA-LDA analysis is generally considered best practice in multivariate REIMS analysis^21^, the optimal algorithm for REIMS analysis is likely dependent on the classification problem^53^ and, as such, evaluation of multiple algorithms is recommended during model development. Many included studies trained their models for binary classification tasks (for example, healthy versus malignant tissue)^22^, whilst others trained a subcategory classification model (for example, different types and grades of malignancy)^30^. PCA-LDA analysis appeared to perform well in both binary and subcategory analyses, for example Mason et al.^33^ applied PCA-LDA to both binary (no disease versus disease) and subcategory (cancer versus adenoma versus normal tissue) classifiers. Despite this strong performance, a number of studies tested experimental statistical methods that outperformed PCA-LDA for their specific classification task. PCA-LDA performs well for classification of groups that tend to show large differences in the molecular profiles of the samples^53^. However, when the molecular profiles of groups are less distinct, alternative machine learning methods may perform more favourably. Another common model used for analysis is partial least squares discriminant analysis (PLS-DA). PLS-DA is a ‘supervised’ version of PCA, meaning it reduces dimensionality, but has an awareness of the class labels^54^. Due to the variety of pathologies, models tested, and settings among included studies, there is insufficient data to determine the overall best performing model. However, with further research, larger sample sizes, and a consideration for the classification task required (binary versus subcategory), model performance may improve as the model itself is tailored to the specific pathology.
Data set size and model validation
Among the included articles, data set size ranges from 87 to 11 100 spectra and multiple model validation methods are implemented. Cross-validation is an essential step when developing AI algorithms, such as those used to interpret REIMS data. Cross-validation partitions the data set into independent cohorts for training and testing, allowing model performance to be evaluated, whilst minimizing bias and overfitting^55^. The most common cross-validation method applied is leave-one-patient-out cross-validation, seen in 13 of the included articles. This method leaves out all spectra from an individual patient and rebuilds the model without them. It then tests the removed spectra against the new model to determine the diagnostic accuracy of the model. This is repeated with each individual patient sample^38^. This has the benefit of providing more data available for use in training, but requires significant computational demands to calculate. An alternative methodology employed by 11 articles is k-fold cross-validation, during which the data set is divided into ‘k’ subsets, with the majority applied during model training and a subset reserved for model testing^55^. For example, in five-fold cross-validation, the data set is divided into five ‘folds’. One fold (20% of the spectra) is randomly excluded from the training set and the model is built with the remaining 80% of spectra. The 20% is used to test the model and this process is repeated five times to include all spectra^29^. Anywhere from two to five folds have been applied among included articles. A disadvantage of this approach is that the ‘test’ data set may not be truly representative of the population^55^. Three included studies did not explicitly specify their method of cross-validation. The significant range of data set sizes, along with different cross-validation models applied to available data, may account for some of the differences in model performance, despite similar pathology and experimental methodology.
Metabolite patterns
Overall, 18 of the 26 included studies commented on substances contributing to class separation between normal and pathological tissue analysis using REIMS. Sixteen of these studies involved lipids, one study^35^ found glycosaminoglycans to be the main class separator between true and false lumen wall tissue in type A aortic dissection, and another^28^ commented on ‘metabolic profiles’ separating tumour and soft tissue without specifying the metabolites contributing to this. Of the 16 studies commenting on lipids, 15 of these used lipid markers to distinguish cancerous tissue from normal tissue and one study^41^ used lipid markers to distinguish burnt tissue from non-burnt tissue. The ability of lipid markers to differentiate cancerous from normal tissue aligns with the understanding that tumour cells demonstrate altered phospholipid metabolism^56,57^. Specific metabolites contributing to class separation are summarized in Table 3.
With respect to lipid biomarkers in cancer, Van Hese et al.^30^ found that differences between classes were due to different mass peak ratios, rather than the presence or absence of specific lipid species. Mason et al.^31^ supported this conclusion, suggesting no single lipid metabolite is capable of acting as a disease biomarker, with multivariate modelling required to assess differences in relative abundance. Balog et al.^9^ also found that the profiles of lipid species, rather than specific biomarkers, account for histological specificity. These conclusions are supported by existing oncological research, which demonstrates that changes in lipid metabolism in tumour cells are not common to all cancer types; indeed, there can even be lipid heterogeneity within a single tumour^58^. This heterogeneity also validates the role of REIMS and the subsequent univariate and multivariate statistical analysis process in tissue detection, which allows a vast array of lipids and their relative abundance to be considered in the analysis, rather than looking for a finite number of ‘biomarkers’.
Safety profile
The safety profile of REIMS is largely based on the commonplace use of diathermy technology in operating theatres worldwide. Janssen et al.^18^ reported no breach of the surgical sterile field during in vivo use of REIMS. Mason et al.^33^ reported no patient safety concerns when REIMS was coupled with transanal minimally invasive surgery (TAMIS).
Diathermy settings
Surgical diathermy units convert electrical energy into heat, which creates diathermy ‘smoke’. This smoke contains 95% steam and 5% cellular debris^59^ and, as such, can be analysed with REIMS to allow tissue identification. Surgical diathermy can either involve a monopolar or bipolar circuit. Monopolar diathermy creates current flow from the diathermy device, through the body, and back to the electrosurgical unit via a dispersive electrode. Bipolar diathermy creates current flow from an active electrode to the return electrode on the opposite blade of a pair of forceps. The diathermy effect can be altered based on machine settings, with common options being ‘cut’ (uses a pure continuous sine wave of low voltage to vapourize tissue) and ‘coagulate’ (uses an intermittent sine wave at higher voltage to reduce the rate of heat rise and coagulate tissue)^59^. Santilli et al.^21^ determined that insufficient smoke or low-intensity signals make prediction of sample class difficult. Using diathermy in the cut mode generates significantly more surgical smoke compared with the coagulate mode^7^, which would suggest the cut mode is more appropriate for REIMS use. Interestingly, Vaysse et al.^26^ identified different lipid patterns generated by the cut and coagulate modes, with fatty acids, phospholipids, and cardiolipin predominant in the cut mode, whilst triacylglycerols predominated in the coagulate mode. Kaufmann et al.^24^ noted that certain triglycerides were distinctly elevated in the coagulate mode, suggesting that the electrosurgical mode impacts the spectral fingerprint of the tissue being analysed. This difference was more pronounced in breast cancer tissue compared with normal adipose tissue. Van Hese et al.^30^ determined that a monopolar REIMS model was applicable to bipolar diathermy applications.
Reported quantitative outcomes
All included studies made some quantitative comment on the performance of REIMS technology for tissue identification, as summarized in Table 4. However, despite 14 studies using both ex vivo and in vivo data, only 3^9,18,33^ explicitly reported in vivo quantitative data. Two studies^26,39^ did not specify if their quantitative outcomes were derived from ex vivo or in vivo data (or a combination). One study^25^ used a data set containing both in vivo and ex vivo data. Across a variety of statistical methods used to interpret data, accuracy was the most commonly reported quantitative measure, with 24 studies discussing this. Ex vivo accuracy ranged from 69.7% to 98.6% (median 87.4%) and in vivo accuracy ranged from 50% to 96.2% (median 90%). Sensitivity ranged from 59.4% to 100% (median 86.4%) in an ex vivo setting, with one in vivo sensitivity value reported at 97.7%. Specificity ranged from 73.5% to 100% (median 91.0%) in an ex vivo setting, with one in vivo specificity value reported at 96.5%.
Discussion
To the best of the authors’ knowledge, this is the first systematic review investigating the role of REIMS and iKnife technology in surgery. This systematic review captured 26 studies exploring the role of REIMS technology in a surgical environment. A robust assortment of both qualitative and quantitative outcomes was reported and a systematic narrative synthesis of data was performed.
Intraoperative tissue identification using REIMS has the potential to provide a significant step forwards for the surgical field. Incomplete excision of cancerous lesions increases both patient morbidity and healthcare costs^60^. For BCC, the most common pathology involved among included studies, a widely accepted target for incomplete excision rates is <5%^61^. In reality, this figure varies widely^62–64^, with many centers reporting higher rates of incomplete excision. Incomplete BCC excision margins are associated with 31–41% recurrence, compared with 1% recurrence where margins are clear^60^. The rates of incomplete excision and recurrence will vary in comparison with other types of tumour. Intraoperative sampling of margins has the potential to decrease the rate of incomplete tumour excision. Emergency burns surgery aims to debride burnt skin until healthy tissue is reached, at which point skin grafts or dressings can be applied^65^. Of the available debridement methods, tangential excision is the ‘gold standard’, which sequentially shaves off burn eschar until a viable wound bed is exposed^66^. This process is heavily reliant on surgeon experience. In tangential excision, both excessive and inadequate debridement have significant consequences for the patient. Conservation of the deep dermis limits the area to be subsequently grafted, results in less scar tissue formation, and improves the texture of the graft^67^. Conservation of underlying subcutaneous fat also results in better cosmetic outcomes^68^. However, adequate removal of non-viable tissue leaves a wound bed that is less prone to infection and reduces the generation of systemic inflammatory mediators^68^. Even with advanced diagnostic methods to guide the assessment of burn depth (such as infrared photography, ultrasonography, and laser Doppler imaging), determining the ideal extent of debridement remains a difficult task^69^. The potential to guide burns debridement, by providing an intraoperative assessment of tissue viability, is another promising application of REIMS.
In addition to the applications in cancer, burns, and aortic surgery described in the included articles, there are numerous other surgical disciplines that have the potential to benefit from REIMS. Orthopaedic and spinal surgery has identified a role for intraoperative tissue classification, to guide surgical navigation and alleviate malpositioning of hardware^70^, but REIMS has not yet been explored in this field. There has also been research into the coupling of REIMS technology with robotic surgery platforms, which can further increase the accuracy of dissection^71^. REIMS can also rapidly classify bacterial species with high accuracy^72^, suggesting potential benefits during surgical debridement of infection, where identification of causative pathogens may facilitate earlier treatment with appropriate antimicrobial agents.
With 23 of the included 26 studies focusing on REIMS in the context of cancer detection, there are implications of this pathology on the quantitative outcomes required of any new diagnostic tool. Sensitivity relates to a test correctly diagnosing a patient with disease as positive, whilst specificity is the ability of a test to correctly diagnose a patient without disease as negative^73^. A sensitive test is important in cancer, to ensure that, if residual disease is present, the surgeon is alerted to this so further tissue can be resected. This may reduce the re-excision rate due to incomplete margins, which have implications such as delaying adjuvant treatment, poor cosmetic outcomes, and increased risk of local and distant disease recurrence^74^. The cost of false negatives is also much higher than false positives when applied to cancer margin detection^22^, favouring a highly sensitive test. The quantitative outcomes of REIMS have largely been determined compared with ‘gold standard’ histopathology in the included studies and it is important to remember that REIMS is providing intraoperative information on tissue type to guide decision-making, but is not replacing the role of postoperative histopathology for definitive diagnosis.
Another promising feature of REIMS analysis in the context of malignancy is the potential to identify features that may assist with disease prognostication. Early research into REIMS suggested it could provide information on the grade and possible necrosis of tumour tissue^8^. Mason et al.^31^ found that REIMS was able to predict the presence of histological features associated with prognosis in colorectal cancer. REIMS predicted nodal micrometastasis with the same negative predictive value as preoperative cross-sectional imaging (78.0% with REIMS versus 78.8% with imaging). However, the accuracy of distinction of tumour stage (52.6%), lymphovascular invasion (57.6%), and tumour subtype (49.7%) was relatively low in this study. Balog et al.^9^ found that metastatic deposits showed clear metabolic separation from surrounding tissue, in contrast to primary tumours with a transition zone, meaning REIMS may help determine if a tumour is of primary or metastatic origin. Vaysse et al.^28^ found that REIMS was capable of detecting 10% tumour cells in a sample with 83% sensitivity and 82% specificity, which points to a role for REIMS in margin recognition in highly infiltrative malignancies. Kaufmann et al.^24^ identified that fatty acid metabolism was altered in triple-negative breast cancer compared with oestrogen receptor/progesterone receptor-positive breast cancers, which has important treatment implications for patients^75^. Hendriks et al.^29^ found that metabolite patterns differ between patients with short-term versus prolonged survival in the context of glioblastoma multiforme. This has the potential to enhance survival predictions and help personalize treatment plans.
One issue identified with the included studies is the lack of in vivo quantitative data. Of the 14 studies including in vivo data, only 3^9,18,33^ of these reported separate quantitative in vivo information on the performance of REIMS. For these three papers combined, 89 in vivo patients contributed to the available data, significantly less than the number of ex vivo patients. This is especially relevant, as larger sample sizes are known to improve the diagnostic accuracy of PCA-LDA models^38^, suggesting that further research involving larger patient cohorts has the potential to generate even more accurate REIMS classifications. In vivo validation relies on ex vivo histopathological analysis as the ‘gold standard’ comparator, which introduces a fundamental difference in setting between the test and comparator. Furthermore, diathermy is destructive to tissue and subsequent histopathological analyses must resort to reviewing tissue adjacent to the in vivo REIMS testing site^9^. This then assumes the histopathology result is a true reflection of the adjacent burnt region, when it is known that tissue samples may be heterogeneous^29^. Of the papers evaluating in vivo REIMS, Balog et al.^9^ used continuous video monitoring of the diathermy, synchronized with REIMS data, to provide additional information regarding the tissue being cut. This was supplemented with subsequent histopathological examination along the electrosurgical dissection line. Janssen et al.^18^ used optical tracking to assist in surgical navigation of the diathermy electrode, but relied on visual identification of tumour and healthy tissue regions. Burnt areas were not validated by histopathology, which introduces significant limitations to the analysis by Janssen et al.^18^. Mason et al.^33^ captured video sequences of the procedure, to allow correlation of the tissue being analysed with REIMS spectra. All samples were then submitted for histopathological analysis. As such, all three papers discussing in vivo REIMS analysis utilized some form of visual identification of tissue type in an attempt to further evaluate in vivo REIMS analysis. Only two of these studies supplemented this with histopathology. The ex vivo nature of the ‘gold standard’ histopathological comparator and small sample size do limit these in vivo analyses.
There are significant practical limitations of REIMS, including financial cost and large machine size. The technology in its current form requires a central location within operating theatres due to limited mobility, as well as temperature regulation mechanisms^39^. There is also a complex process of instrument set-up, including calibration, which requires technical expertise. Surgical smoke generated by the diathermy unit must be aspirated into the REIMS machine for analysis. This process is often driven by a Venturi air pump^38^, which transports smoke via polytetrafluoroethylene (PTFE) tubing to the machine^40^. Many diathermy units have built-in smoke evacuation channels, originating near the diathermy tip, which help facilitate this process. Another limitation of the REIMS set-up is the delay between tissue contact with diathermy and REIMS detection. The large machine size and requirement for a central location mean that a significant length of tubing may be needed between the diathermy unit and the REIMS unit, especially for in vivo applications. A delay of between 0.7 and 2.5 s was noted by Balog et al.^9^ and a 1.8 s delay was noted by St John et al.^36^. This delay introduces latency between tissue sampling and the REIMS signal feedback, which may cause errors with interpretation or delays in the procedure. This delay can affect the usability and practical applicability of the REIMS set-up^76^, but can be minimized by optimizing tube diameter and flow rate. These logistical and technical challenges have been identified as an obstacle to routine implementation in a clinical environment^33^, but, with further development, some of these limitations may be addressed. The destructive nature of diathermy use during REIMS testing, especially on small tissue samples, can make the precise cell composition of sampling points difficult to confirm^24^. This may also impact the postoperative formal histopathological analysis of tissue^28^. Consideration must also be given to surgical cases that do not routinely use diathermy, in which a diathermy set-up would be required specifically to facilitate REIMS analysis, incurring further costs. There has been no formal analysis to date investigating the impact of REIMS technology on operating time and operating theatre turnaround. Many of the included studies had a significant risk of bias, again suggesting the need for high-quality, randomized, prospective research further evaluating the technology.
With further research into REIMS and uptake of the platform, more in vivo data should be generated to validate the promising ex vivo results. This should also help determine the optimal univariate and multivariate data analysis methods for each pathology and patient cohort. Alexander et al.^37^ identified that age and sex were not strongly predictive of data, although there was some clustering in males and patients >70 years of age. Davies et al.^32^ also found that patient sex did not discriminate in their model. Because REIMS data appear relatively unchanged by common variables such as age and sex, development of large pathology-specific REIMS databases could facilitate robust data models to improve detection accuracy. As the technology supporting REIMS analysis improves, and data analysis models are generated based on large sample numbers, REIMS interpretation could move towards a succinct ‘on screen’ assessment of the sample (red/green, pathological/normal), rather than a full spectrum of data, to assist with intraoperative decision-making.
The potential for REIMS to guide intraoperative tissue identification has been explored in a number of surgical disciplines with significant potential benefits. This systematic review has highlighted the uses, qualitative and quantitative outcomes, and limitations of REIMS in surgery to date. Future research should focus on in vivo applications of REIMS, with large patient numbers and in a broader range of surgical applications, to provide a more rigorous assessment of the technology and its potential benefits.
Supplementary Material
znaf228_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Balog J, Szaniszlo T, Schaefer K-C, Denes J, Lopata A, Godorhazy L et al Identification of biological tissues by rapid evaporative ionization mass spectrometry. Anal Chem 2010;82:7343–735020681559 10.1021/ac 101283 x · doi ↗ · pubmed ↗
- 2Preeti A, Sameer G, Kulranjan S, Arun Abhinav S, Preeti R, Sunita Y et al Intra-operative frozen sections: experience at a tertiary care centre. Asian Pac J Cancer Prev 2016;17:5057–506128122434 10.22034/APJCP.2016.17.12.5057 PMC 5454636 · doi ↗ · pubmed ↗
- 3Mahe E, Ara S, Bishara M, Kurian A, Tauqir S, Ursani N et al Intraoperative pathology consultation: error, cause and impact. Can J Surg 2013;56:E 13–E 1823706852 10.1503/cjs.011112 PMC 3672438 · doi ↗ · pubmed ↗
- 4Orringer DA, Pandian B, Niknafs YS, Hollon TC, Boyle J, Lewis S et al Rapid intraoperative histology of unprocessed surgical specimens via fibre-laser-based stimulated Raman scattering microscopy. Nat Biomed Eng 2017;1:002728955599 10.1038/s 41551-016-0027 PMC 5612414 · doi ↗ · pubmed ↗
- 5Watson AB, Loughman J. The surgical diathermy: principles of operation and safe use. Anaesth Intensive Care 1978;6:310–321736252 10.1177/0310057 X 7800600404 · doi ↗ · pubmed ↗
- 6Spearman J, Tsavellas G, Nichols P. Current attitudes and practices towards diathermy smoke. Ann R Coll Surg Engl 2007;89:162–16517346413 10.1308/003588407 X 155752 PMC 1964566 · doi ↗ · pubmed ↗
- 7Karuppal R, Surendran S, Patinharayil G, Muhammed Fazil VV, Marthya A. It is time for a more cautious approach to surgical diathermy, especially in COVID-19 outbreak: a schematic review. J Orthop 2020;20:297–30032425415 10.1016/j.jor.2020.05.013PMC 7229731 · doi ↗ · pubmed ↗
- 8Schäfer K-C, Dénes J, Albrecht K, Szaniszló T, Balog J, Skoumal R et al In vivo, in situ tissue analysis using rapid evaporative ionization mass spectrometry. Angew Chem Int Ed Engl 2009;48:8240–824219746375 10.1002/anie.200902546 · doi ↗ · pubmed ↗