Sample Size of Trials Investigating the Impact of Point‐of‐Care Ultrasound‐Guided Strategies on Patient Outcomes: A Systematic Review
William Beaubien‐Souligny, Michel Gouin, Karel Huard

TL;DR
This paper reviews how sample sizes in trials using point-of-care ultrasound are often too small to detect meaningful effects, leading to underpowered studies.
Contribution
The study introduces a systematic analysis of sample size assumptions in POCUS-guided trials and highlights their underpowered nature.
Findings
Most POCUS-guided trials have median sample sizes of 206 participants, often below what is needed for adequate power.
Only 68% of trials reported sample size justifications, and 41% failed to meet recruitment targets.
Sample size requirements depend heavily on the proportion of cases where POCUS changes management.
Abstract
Point‐of‐care ultrasound (POCUS) is increasingly utilized for bedside diagnosis and management in diverse clinical contexts. However, the design of randomized controlled trials (RCTs) evaluating the impact of POCUS‐guided strategies on clinical outcomes presents significant challenges. This study aims to explore the assumptions underlying sample size estimation in POCUS‐guided trials and assess the adequacy of sample sizes in published trials through a systematic review. We performed a sample size analysis considering varying rates of POCUS‐induced management changes and plausible effect sizes on binary and continuous patient‐centered outcomes. Additionally, a systematic review of PubMed was conducted to identify RCTs comparing POCUS‐guided management to usual care, extracting data on planned and actual sample sizes and justifications for sample size decisions. Sample size estimations…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
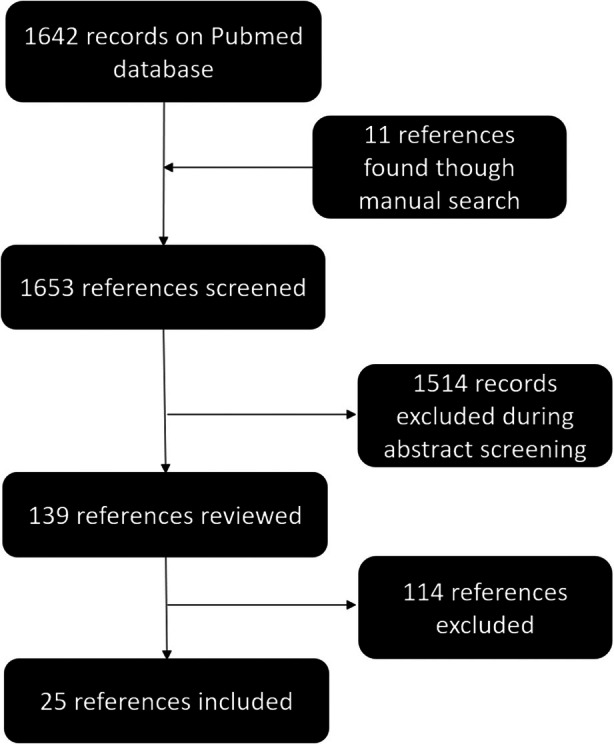 Figure 1
Figure 1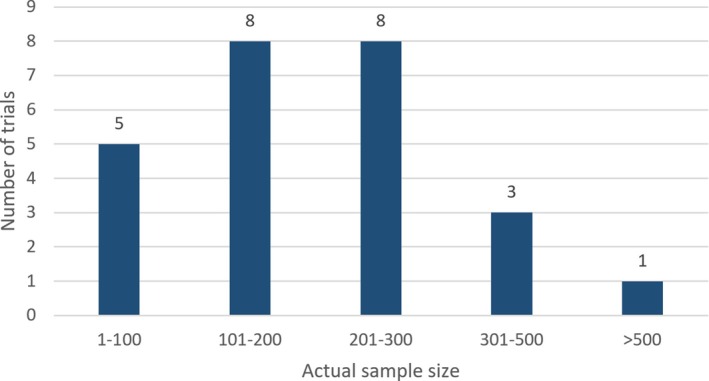 Figure 2
Figure 2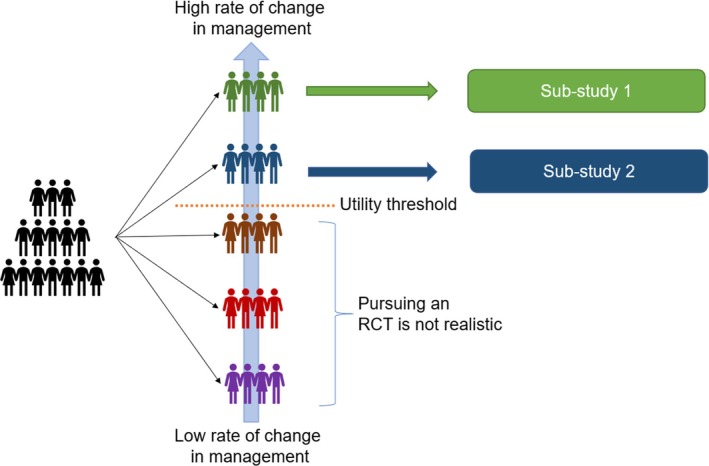 Figure 3
Figure 3| Plausible Effect Size Resulting From POCUS‐Guided Changes in Management (OR) | Proportion of Participants in Which POCUS Results Lead to a Change in Management | Expected Observable Effect Size of the POCUS‐Guided Strategy Compared to Usual Care (OR) | Estimated Sample Size |
|---|---|---|---|
| Large (OR = 0.6) | 100% | 0.60 | 208 |
| 75% | 0.70 | 307 | |
| 50% | 0.80 | 560 | |
| 25% | 0.90 | 1766 | |
| 10% | 0.96 | 9389 | |
| Moderate (OR = 0.7) | 100% | 0.70 | 383 |
| 75% | 0.78 | 593 | |
| 50% | 0.85 | 1148 | |
| 25% | 0.93 | 3889 | |
| 10% | 0.97 | 21,806 | |
| Small (OR = 0.8) | 100% | 0.80 | 888 |
| 75% | 0.85 | 1440 | |
| 50% | 0.90 | 2941 | |
| 25% | 0.95 | 10,607 | |
| 10% | 0.98 | 62,096 |
| Plausible Effect Size Resulting From POCUS‐Guided Changes in Management | Proportion of Participants in Which POCUS Results Lead to a Change in Management | Expected Observable Effect of the POCUS‐Guided Strategy on Continuous Outcome (% Relative Reduction) | Estimated Sample Size |
|---|---|---|---|
| Large (40% reduction in length of stay) | 100% | 40% | 127 |
| 75% | 30% | 225 | |
| 50% | 20% | 504 | |
| 25% | 10% | 2011 | |
| 10% | 4% | 12,560 | |
| Moderate (30% reduction in length of stay) | 100% | 30% | 225 |
| 75% | 22.5% | 398 | |
| 50% | 15% | 895 | |
| 25% | 7.5% | 3574 | |
| 10% | 3% | 22,328 | |
| Small (20% reduction in length of stay) | 100% | 20% | 504 |
| 75% | 15% | 895 | |
| 50% | 10% | 2011 | |
| 25% | 5% | 8039 | |
| 10% | 2% | 50,234 |
| Authors/Year | Summary | Primary Outcome | Rate of Change in Management With POCUS | Planned Sample Size | Actual Sample Size | Main Result |
|---|---|---|---|---|---|---|
| Binary primary outcome | ||||||
| Chardoli et al | POCUS vs usual care during pulseless cardiac arrest | Mortality (ROSC) | NR, potentially addressable findings found in 14%–78% of assessments | NR | 100 |
No difference Rate: 34% vs 28%, |
| Smith‐Blindman et al | POCUS vs radiology US vs CT for suspected nephrolithiasis | High‐risk diagnosis with complications related to missed or delayed diagnosis | NR | 2500 | 2759 (1:1:1 design) |
No difference Rate: 0.7% vs 0.3%, |
| Siriopol et al | Lung POCUS for fluid management vs usual care in hemodialysis patients | All‐cause mortality and first cardiovascular event—including death, stroke, and myocardial infarction | NR | 480 | 250 |
No difference HR: 1.09 CI: 0.64; 1.86, |
| Chen et al | Use of POCUS during morning rounds in patients with sepsis vs usual care | Mortality | 17%–29% of encounters | No sample calculation was performed | 129 (1:2 design) |
No difference Rate: 0.27 vs 0.43, |
| Atkinson et al | POCUS vs usual care for hypotension in the ED | 30‐Day mortality | Not reported, 9%–55% clinically relevant findings | 400 | 273 |
No difference Rate difference: 0.35% CI: −10.2%, 11.0% |
| Rivas‐Lasarte et al | Lung POCUS vs usual care during outpatient follow‐up after acute heart failure | Composite of urgent visits, hospitalization for heart failure or death during follow‐up | NR | 124 | 124 |
Difference HR: 0.52 CI: 0.27, 1.00, |
| Araiza‐Garaygordobil et al | Lung POCUS vs usual care in outpatients with heart failure | Composite of urgent heart failure visits, re‐hospitalizations or death | NR | 124 | 126 |
Difference HR: 0.55, CI 0.31–0.98, |
| Zoccali et al | Lung POCUS for fluid management vs usual care in hemodialysis patients | Composite of all‐cause death, myocardial infarction and decompensated heart failure | NR | 500 | 363 |
No difference HR: 0.88; CI: 0.63–1.24 |
| Musikatavorn et al | US‐guided fluid management (IVC) vs usual care in adults with sepsis | 30‐Day mortality rate | NR | 242 | 211 |
No difference Rate: 18.8% vs 19.8%, |
| Li et al | Cardiopulmonary POCUS vs usual care for septic shock | 28‐Day mortality | NR | 94 | 94 |
No difference Rate: 50.6% vs 60.0% |
| Ricci et al | POCUS vs usual care to guide diuretic adjustments in acute heart failure | 30‐Day readmission rate | NR | 250 | 250 |
No difference 19% vs 15%, |
| Torres‐Macho et al | Lung POCUS vs usual care after discharge for acute heart failure | Cardiovascular death, readmission, or emergency department or day hospital visit for heart failure | NR | 152 | 79 |
No difference 26.1% vs 29.7%
|
| Ravetti et al | POCUS vs usual care after high‐risk surgery | Acute kidney injury | NR | 178 | 111 |
No difference Rate: 27.5% vs 23.3%, |
| Zisis et al | POCUS‐guided lung decongestion in decompensated heart failure vs usual care | Hospital re‐admission or death | NR | NR | 122 |
No difference OR: 1.36; CI: 0.59–3.1; |
| Continuous primary outcome | ||||||
| Lucas et al | POCUS vs standard echocardiography for inpatients with an indication for echocardiography | Length of hospital stay | 37% of patients | 420 | 453 |
No difference 1.7% CI: −12.1, 9.8% |
| Han et al | POCUS to monitoring lung congestion vs usual care after pediatric cardiac surgery for congenital disease | Duration of mechanical ventilation | NR | NR | 100 |
Difference 15.0 vs 38.5 hours |
| Park et al | Use of POCUS vs usual care in the context of renal colic in the ED | Length of stay in the ED | NR | NR | 103 |
Difference 89.0 vs 163 minutes |
| Wilson et al | POCUS vs usual care in patients who require a pelvis ultrasound in the ED | Length of stay in the ED | NR | No sample calculation was performed | 194 |
Difference −120 minutes CI: 66–173 |
| Morgan et al | POCUS vs radiology US in pregnant women with abdominal pain or bleeding | Length of stay in the ED | NR | 300 | 224 |
No difference −20 minutes CI: −54; 7 |
| Kim et al | POCUS vs usual care for renal colic | Length of stay in the ED | NR | 152 | 152 |
Difference 172 vs 234 minutes |
| Guner et al | POCUS‐guided diagnostic strategy vs usual care for chest pain | Length of stay in the ED | NR, POCUS led to findings in 31% | NR | 208 |
Difference 133 vs 215 minutes |
| Cid‐Serra et al. | Multiorgan POCUS vs usual care for patients admitted for a cardiopulmonary diagnosis | Length of hospital stay | NR | 250 | 250 |
No difference 113 vs 125 hours |
| Durgun et al | POCUS diagnostic strategy vs usual care for abdominal pain in the emergency department | Length of stay in the ED | NR, findings in 64% | NR | 207 |
Difference 209 vs 286 minutes |
| Psalidas et al | POCUS vs usual care to evaluate the success of pleurodeses in patients with malignant pleural effusion | Length of hospital stay | NR | 254 | 313 |
Difference 2 vs 3 days, |
| Arvig et al | Repeated cardiopulmonary POCUS vs usual care (only at admission) in adult patients admitted for dyspnea | Reduction of dyspnea score | NR | 206 | 206 | Difference −1.66 point; CI: −2.09 to −1.23 |
- —Fonds de Recherche du Québec ‐ Santé
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Hemodynamic Monitoring and Therapy · Cardiac, Anesthesia and Surgical Outcomes
Performing a randomized clinical trial (RCT) is well‐established as a necessary step to demonstrate the efficacy of a medical strategy. While the methodology of RCTs has been focused primarily on testing pharmacologic interventions, it is also feasible to investigate other types of interventions including complex management strategies guided by additional information including imaging modalities.1, 2
It is generally advisable to test new interventions by comparing them to current usual care to determine if the new strategy is truly advantageous. Pharmacology trials imply that the management in the intervention group will be different in almost all participants compared to the usual care group unless non‐adherence or contamination of the control arm occurs at a high rate. In this setting, the difference observed between groups can be inferred to be proportional to the biological effect of the pharmacologic agent. In contrast, in trials involving strategies guided by additional information, the care provided to participants in the intervention group may not necessarily differ from usual care, as other sources of information could lead to the same decision‐making process and result in similar management.
Point‐of‐care ultrasound (POCUS) has seen an increase in popularity in the last decade under the premise that the information provided can significantly impact patient care through early diagnosis or more precise clinical decisions at the beside.3 The indications to perform POCUS have progressively widened to include trauma,4 respiratory failure,5 undifferentiated shock,6 acute kidney injury,7 and cardiac arrest.6 There are numerous testimonies that POCUS can significantly impact the management.8 However, despite showing that POCUS examination can hasten the time to the correct diagnosis in a multitude of settings,9, 10 incertitude remains on how this type of strategy impacts important patient outcomes.11
We propose to explore assumptions regarding sample size estimation in trials of POCUS‐guided therapy. We then perform a systematic review of the literature to assess the sample size of published trials and evaluate whether sample size decisions during the design of trials investigating the impact of POCUS‐guided strategies on patient‐centered outcomes are appropriate.
Materials and Methods
This report includes an analysis of sample size estimations and a systematic review. It does not contain original participant data, and research ethics board approval was therefore not required.
Analysis Related to Sample Size Requirements
To produce a realistic estimate of sample size requirements for a hypothetical trial with a primary binary patient outcome with 1:1 group attribution, we assumed a rate of 40% in the control group and performed a sample size estimation to achieve a power of 0.8 and a confidence level of 95%. The analysis was repeated for different combinations of the plausible effect size of a POCUS‐guided alteration in clinical management of the studied outcome (odds ratio [OR] 0.6, 07, or 0.8) while considering that these changes would only occur in a given proportion of patients (10%, 25%, 50%, 75%, 100%) which will result in an observed lower adjusted effect size when comparing the intervention and control arms of the trial. The same analysis was repeated using the same methodology but considering a continuous outcome. Analysis was performed in R (version 4.2.2) using package rpact. A complete version of the R script is presented in the online supplemental Appendix 1.
Systematic Review
Eligible Studies
We aimed to include completed randomized clinical trials investigating the impact on patient outcome of a management strategy based on information from POCUS compared to usual care. We excluded trials related to the use of POCUS for procedural guidance and for which the primary outcome was not an outcome related to the patient (i.e., diagnostic performance).
Search Strategy
We performed a systematic search over the PubMed database in July 2024 combining a validated Cochrane term for randomized clinical trials12 and a term specific for studies involving Point‐Of‐Care ultrasound13 (see online supplemental Appendix 1). We also identified additional trials through the bibliography of included studies. A first selection was made based on title, with each entry being reviewed by two investigators. A second selection based on abstract and full‐text review was subsequently performed.
Data Extraction
We extracted information about the population and the intervention investigated in the selected reports. We collected information about planned and final sample size (N), sample size justifications, and reasons for non‐achievement of the planned sample size if reported.
Data Analysis
We report the planned and actual sample size of included trials, as well as the relative difference between the final and the planned sample size (as a %). The reasons for non‐achievement of planned sample size are reported in a descriptive manner when available.
Risk of Bias and Quality of Evidence
In the selected reports, we determine if the calculation of the required sample size is reported within the text or the associated supplementary material. We did not evaluate other components usually included in the risk of bias assessment due to the specific focus of this systematic review.
Results
An Evaluation of Sample Size Requirements
As previously stated, in the context of an RCT evaluating a POCUS‐guided intervention strategy, we can expect that the additional information from POCUS will lead to a change in management in a certain proportion of participants. This proportion may vary depending on the clinical context studied. Since the impact of the POCUS‐guided strategy on patient outcomes can only be mediated through changes in clinical management in response to POCUS findings, we can expect the effective sample size to be much lower than the actual number of participants recruited in the trial.
Another factor to consider is the plausible effect of a POCUS‐guided interventions on patients' outcomes. In some contexts, it can be expected that a relatively rare POCUS finding can lead to a critical change in patient management. For example, finding a significant pericardial effusion during cardiac arrest could lead to a therapeutic pericardiocentesis, which may result in a very large effect on patients' chances of survival. However, in most cases, it is probable that less drastic changes in management will translate to a moderate impact on patients' outcomes. Successful pharmacotherapy trials leading to practice‐changing evidence often demonstrate a moderate effect (OR = 0.7) of an intervention on important patients' outcomes.
According to these considerations, a realistic estimation of sample size requirements in a trial investigating a POCUS‐guided strategy on a binary patient outcome based on the proportion of participants in which POCUS led to a change in management and the expected plausible effect size of these interventions is presented in Table 1.
As an example, if we consider a hypothetical POCUS‐guided strategy that led to a change in management in 50% of participants compared to usual care and that the modification in therapeutic management led to a moderate clinical benefit (OR = 0.70), the expected difference in the incidence of the studied outcome of the POCUS‐guided strategy compared to usual care is expected to be small (OR = 0.85). Consequently, this trial would require a considerable sample size (N = 1 148) to achieve sufficient statistical power.
A continuous outcome, such as length of stay in the hospital, could also be used as a patient‐centered endpoint. A similar analysis regarding this type of outcome and the same previous assumptions is presented in Table 2. With a similar example, if POCUS‐guided strategy leads to a change in management in 50% of participants compared to usual care, even if the modification in therapeutic management can lead to a significant reduction in the hospital length of stay (reduction from 10 to 7 days of hospitalization [−3 days, relative 30% reduction]), the expected difference in the incidence of the studied outcome within a trial of POCUS‐guided strategy compared to usual care is expected to be smaller (−1.5 days, relative 15% reduction). Consequently, this trial would require a considerable sample size (N = 895) to achieve sufficient statistical power.
Systematic Review of Planned and Final Sample Sizes in Published Trials of POCUS‐Guided Management
We screened 1653 references and identified 25 eligible trials (Figure 1 and Table 3). The median sample size was 206 participants (interquartile range = 122; 250) as shown in Figure 2. Sample size justifications were provided for 17 trials (68.0%). Among these trials, 7 (41.2%) did not achieve their pre‐specified sample size target with a median relative difference of −31.8% (interquartile range: −26.4; −42.8%) between the planned and final sample size. Several reasons were cited including insufficient recruitment,14, 15, 16 perceived futility,15 and other circumstances (pandemic,17 site drop‐off16).
Reference inclusion flowchart.
Final sample size of trials comparing POCUS‐guided strategies to usual care for a primary patient outcome (N = 25).
In terms of results, 2/14 (14.3%) of studies investigating a binary outcome reported a significant difference, while 8/11 (72.7%) of studies investigating a continuous outcome (i.e., length of stay) reported a significant result (P = .003).
Based on the analysis presented in the previous section, only one RCT18 considering a binary primary outcome reported a sample size with appropriate statistical power to detect the impact of a POCUS‐guided strategy, assuming the additional information would have led to a large clinical impact in approximately half of the patients randomized in the intervention group. Of note, in terms of patient‐centered outcomes, the sample size estimation for this study was centered on non‐inferiority of the POCUS‐guided approach related to the occurrence of a patient‐centered binary event (high‐risk diagnoses in the context of suspected urolithiasis).
Discussion
In this analysis, we first suggest that a realistic sample size estimation regarding trials of POCUS‐guided management should consider the plausible effect of the change in management resulting from the additional information provided, as well as the proportion of participants in the intervention group for whom POCUS results will lead to a change in management compared to usual care. Secondly, through a systematic review, we propose that most previous trials of POCUS‐guided management were generally underpowered according to these considerations, although a higher proportion of trials investigating continuous outcomes demonstrated significant differences in their primary outcome compared to trials investigating a binary outcome.
The concerns related to misleading results that can arise from trials that are underpowered to detect the plausible effect of an intervention have already been explored in other areas of biomedical research.19 However, these concerns are particularly relevant to POCUS research, as there are several barriers to conducting multicenter trials on complex medical interventions.20 Integrating POCUS as a primary source of information to guide therapy comes with a specific set of challenges which are compounded when the design of a large multicenter trial is considered. First, there must be enough POCUS operators at participating sites, while ensuring that contamination is avoided. This is challenging to achieve since POCUS operators in this context are likely members of the hospital staff and are likely to use POCUS in their practice. Secondly, POCUS skill and interpretation must be standardized within teams and across sites. Therefore, an onboarding strategy including proper training becomes a crucial preliminary step before site activation. Nonetheless, this approach has been shown to be feasible.21 In general, according to these considerations, the human and financial costs required to conduct a definitive trial of a POCUS‐guided strategy are substantial.
Our review suggests that researchers in this field may not have been fully prepared. An important proportion did not meet their target enrollment at the end of the trial, and some authors did not report either the rationale of sample size estimation or the actual enrollment target. The strategies to overcome the barriers associated with the design and conduct of RCTs of POCUS‐guided strategies have seldom been explored. One approach would be to ensure, prior to designing a large‐scale multicenter trial, that a high rate of management changes in response to POCUS information is expected in the studied population. Epidemiological studies and questionnaires in POCUS users, and pilot trials in target populations would help describe the rate of modification and determine whether a large trial is likely to succeed. For example, Table 1 shows that the required sample size in a population with a 25% rate of modification (N = 3 889) would be more than 6 times higher than if the rate of modification is 75% (N = 593) considering a high‐impact change in management resulting from POCUS. In this regard, studies investigating the impact of the use of POCUS as a reliable method to safely exclude a diagnosis in the emergency department leading to earlier discharge are more likely to impact a higher proportion of patients. This may explain why studies considering a continuous primary outcome, usually length of stay, were more likely to yield a positive result according to our review. Even if most studies reported a modest reduction of emergency department length of stay (<2 hours), this difference can translate into meaningful improvements in efficiency, resulting in a benefit that extends to other patients as well in the form of reduced waiting time or by enabling clinicians to devote greater attention to emergency department patients with complex needs.
Despite the potential barriers, performing large‐scale biomarker‐guided trials has been previously done, such as natriuretic peptide‐guided therapy for heart failure, whose benefit is only apparent in large meta‐analysis22 despite widespread use in heart failure clinics.23 Another approach would be to obtain these key elements directly during a pilot phase of the RCT, which would also enable exploration of optimal workflow and feasibility of the proposed intervention. Enrichment strategies to enroll participants in which POCUS information is the most likely to modify management must be pursued. Novel trial designs, including adaptive basket trials, could in theory be used to define the target subgroups in which the conduct of a large‐scale trial would be feasible without the need for separate pilot trials if the intervention (or type of POCUS assessment) is applicable to this heterogeneous population (Figure 3). Finally, including only participants for whom there is uncertainty related to the use of POCUS according to the treating clinician could also be an important enrichment strategy, although it could lead to significant heterogeneity related to the usual care of practitioners and within institutions.
Concept of an adaptive basket trial related to Point‐Of‐Care ultrasound assessment. A large general hospitalized or ICU population is considered at the start of the trial. At a predefined timepoint, the sub‐groups for whom the trial will continue will be selected based on the proportion of participants for whom the information from the POCUS examination results in a change in clinical management.
Our analysis has several limitations. First, this analysis and review excluded use of POCUS for procedural guidance to focus on POCUS‐guided management strategies. Other considerations specific to procedural POCUS could have been relevant to this analysis. Secondly, our sample size estimation is derived from a limited number of possible combinations of parameters. Thirdly, our systematic review was not prospectively registered and is limited to report published in the PubMed database. Finally, we only considered the studies regarding the clinical impact of a POCUS‐guided strategy which exclude studies on other potential benefits of POCUS including diagnostic accuracy. It could be argued that the evidence‐base for the use of the technology could rest entirely upon its benefit, even if the impact on patient outcomes remains elusive. While POCUS has been advocated as the fifth pillar of physical examination, our expectations from an evidence‐based medicine standpoint seems at odds with other traditional components of physical examination. For example, The Journal of American Medical Association's classic series “The Rational Clinical Examination” presents the literature on the diagnostic performance of diverse physical examination maneuvers without regard to whether performing these examinations improves patient outcomes. However, these physical examinations assessments remain widely regarded as the standard for clinicians to determine which skills are worthwhile mastering. Apart from diagnostic accuracy, more appropriate measures of success regarding POCUS may include cost savings in radiology and monitoring apparatus, shorter time to final diagnosis, reduced rate of missed life‐threatening diagnoses, reduced diagnostic uncertainty among clinicians, fewer outpatient visits for additional investigations culminating in greater patient satisfaction.
Conclusion
The design of RCTs on POCUS‐guided therapy should have realistic considerations regarding sample size requirements to determine the impact on patient outcomes. In theory, this involves producing an accurate estimation of the proportion of participants in which POCUS will yield information that will significantly influence decision‐making. Research efforts should continue to define the optimal approach for generating the evidence base for the use of POCUS in medicine.
Supporting information
Data S1. Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Craig P , Dieppe P , Macintyre S , Michie S , Nazareth I , Petticrew M . Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ (Clin Res ed) 2008; 337:a 1655. 10.1136/bmj.a 1655.PMC 276903218824488 · doi ↗ · pubmed ↗
- 2Murphy P , Koh DM . Imaging in clinical trials. Cancer Imaging 2010; 10:S 74–S 82. 10.1102/1470-7330.2010.9027.20880784 PMC 2967134 · doi ↗ · pubmed ↗
- 3Diaz‐Gomez JL , Mayo PH , Koenig SJ . Point‐of‐care ultrasonography. N Engl J Med 2021; 385:1593–1602.34670045 10.1056/NEJ Mra 1916062 · doi ↗ · pubmed ↗
- 4Scalea TM , Rodriguez A , Chiu WC , et al. Focused assessment with sonography for trauma (FAST): results from an international consensus conference. J Trauma 1999; 46:466–472.10088853 10.1097/00005373-199903000-00022 · doi ↗ · pubmed ↗
- 5Volpicelli G , Elbarbary M , Blaivas M , et al. International evidence‐based recommendations for point‐of‐care lung ultrasound. Intensive Care Med 2012; 38:577–591.22392031 10.1007/s 00134-012-2513-4 · doi ↗ · pubmed ↗
- 6Atkinson P , Bowra J , Milne J , et al. International Federation for Emergency Medicine Consensus Statement: sonography in hypotension and cardiac arrest (S Ho C): an international consensus on the use of point of care ultrasound for undifferentiated hypotension and during cardiac arrest. Can J Emerg Med 2017; 19:459–470.10.1017/cem.2016.39427998322 · doi ↗ · pubmed ↗
- 7Koratala A , Ronco C , Kazory A . Multi‐organ point‐of‐care ultrasound in acute kidney injury. Blood Purif 2022; 51:967–971.35306497 10.1159/000522652 · doi ↗ · pubmed ↗
- 8Andersen CA , Brodersen J , Davidsen AS , Graumann O , Jensen MBB . Use and impact of point‐of‐care ultrasonography in general practice: a prospective observational study. BMJ Open 2020; 10:e 037664.10.1136/bmjopen-2020-037664 PMC 750030032948563 · doi ↗ · pubmed ↗