Free flaps monitoring using implantable doppler: our experience and of the literature
Roberto Baraziol, Annachiara Tellarini, Diego Faccio, Alice Alban, Ferruccio Paganini, Luigi Valdatta, Federico Tamborini

TL;DR
This paper reviews the use of implantable Dopplers to monitor buried free flaps in surgery, comparing two devices and their effectiveness based on literature and the authors' experience.
Contribution
The paper provides a comparative analysis of two implantable Dopplers for buried flap monitoring, based on both literature and the authors' clinical practice.
Findings
Cook Swartz is preferred for head and neck flaps due to fewer false positives.
Synovis Flow Coupler is favored for DIEP flaps based on clinical practice.
Literature confirms the effectiveness of implantable Dopplers over clinical evaluation for buried flaps.
Abstract
Buried free flaps monitoring cannot rely on clinical evaluation, which remains the gold standard in flaps with a skin paddle. A reliable way to monitor buried free flaps is through implantable dopplers, which provide a continuous and direct signal of anastomotic flow. Since the only way to ascertain a suspicion of vascular impairment in buried free flaps is through reoperative exploration, a high specificity is required together with a high sensitivity to avoid unnecessary theatre take-backs A systematic literature search was performed to screen three different databases (PubMed, Web of Sciences, and Embase) and using the following keywords: “Cook Swartz” AND “doppler” AND “flap” AND “monitoring” and “Synovis” AND “Flow Coupler” AND “flap” AND “monitoring”. The indicators of efficacy and effectiveness of the two available implantable dopplers were analyzed and compared to our…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
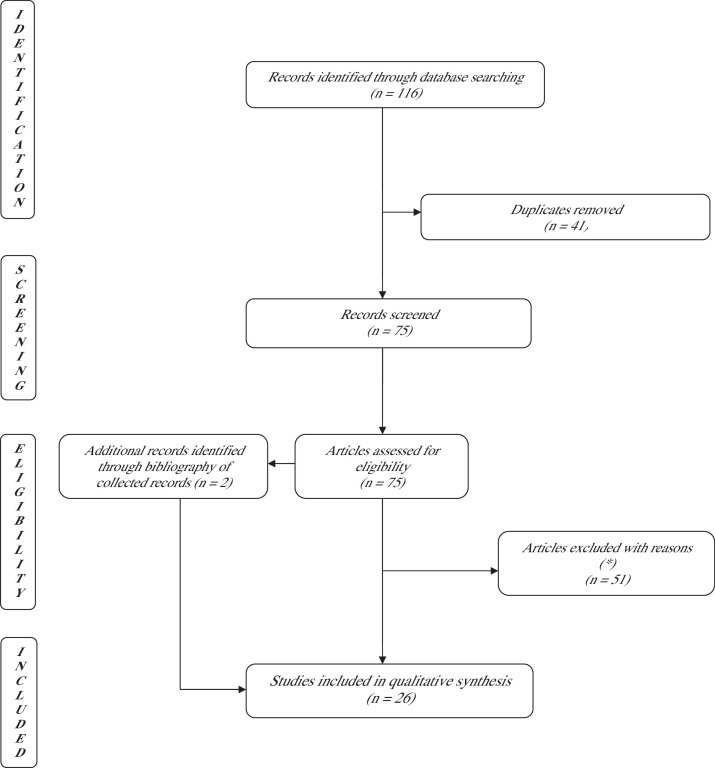 Figure 1
Figure 1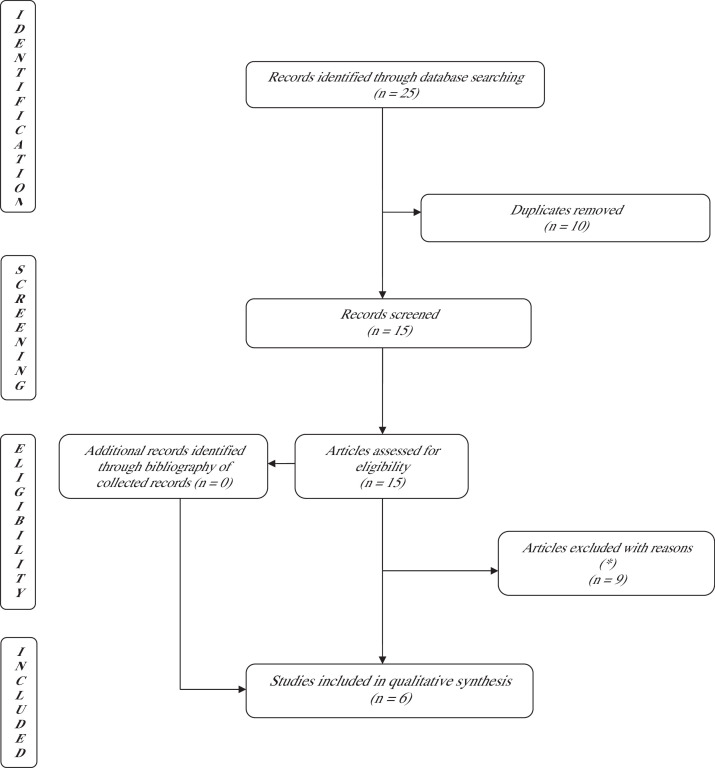 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Dental Implant Techniques and Outcomes · Tissue Engineering and Regenerative Medicine
Introduction
Many techniques for flap monitoring following free tissue transfer have been described in addition to clinical monitoring, which is considered the gold standard, with a very low rate of false positive and false negative in experienced hands. However, there is little evidence that any of these techniques is superior to others'.
Material and methods
Aim of this study was to critically interpret the results of our experience with buried free flaps monitoring using implantable dopplers. To do so, we have made a systematic review of the pertinent literature.
On 1st October 2024, a literature search in accordance with the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines was conducted using PubMed, web of sciences, and Scopus databases to identify relevant articles on free flap monitoring with implantable dopplers (see Figure 1, Figure 2).Figure 1PRISMA flowchart using the keywords: ([{cook Swartz} and {doppler}] and [flap]) and (monitoring). A total of 116 studies were identified through the database search: 26 articles were selected and included.*Review articles, case report, descriptive articles, articles not focusing on test performance.Figure 1. Figure 2PRISMA flowchart using the keywords: ([{Synovis} and {flow coupler}] and [flap]) and (monitoring). A total of 25 studies were identified through the database search: six articles were selected and included. *Review articles, case report, descriptive articles, articles not focusing on test performance.Figure 2
The search algorithm used included two sets of keywords independently typed: “([{Cook Swartz} and {doppler}] and [flap]) and (monitoring)” and “([{Synovis} and {Flow Coupler}] and [flap]) and (monitoring).
The data were independently collected and analyzed by RB and AT.
The inclusion criteria were the following: clinical trials, case series, implantable dopplers, buried free flaps monitoring.
The exclusion criteria consisted of the following: previous reviews and metanalysis, case reports, expert descriptive articles, and animal studies.
Data on patients demographics, flap location/indication and devices performance in term of efficacy and effectiveness were collected. We particularly focused on the following indicators: sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), false positive rate (FPR), false negative rate (FNR), failure rate, success rate and doppler placement (artery vs vein vs both) (See Table 1, Table 2, Table 3, Table 4 and Table 7, Table 8).Table 1. Cook Swartz: characteristic of enrolled patient.Table 1. AuthorTypeNumber Of Patients/ Monitored FlapsSexAge (Mean)Preop-radiotherapyFlap typeFlap LocationBuried Flaps (also) includedIndication for flapVein anastomosis (Coupler Vs Hand Sewn)Doppler duration (Days)Guillemaud et al., 1R351 / 384244 men and 107 women58.63NRRadial forearm (n = 261), fibula (n = 73), anterolateral thigh (n = 38), subscapular (n = 11), gracilis (n = 1)H–NNRTumor (n = 382); non tumor (n = 2)Hand sewnMean: 8.95 days (Range 0–40)Leibig et al.,2R129 / 14783 men and 64 women53.5 ± 18.126.5 %Gracilis (n = 53); latissimus dorsi (n = 28); free vascularized scapular flap (n = 16); free fibular flap (n = 12); free iliac crest (n = 11); radialis flap (n = 26), ALT (n = 1)H-NNRTumor (n = 73); non tumor (n = 74: free muscle transfers for facial reanimation surgery; trauma; osteoradionecrosis; wound healing disorders)Hand sewnmean: 8Paprottka et al.,3R35 / 3515 men and 20 womenNRNRDIEP (n = 15), gracilis (n = 3), transverse muscolocutaneous gracilis (n = 1), ALT (n = 6); LD (n = 10)H-Nyes ( %NR)Tumor (n = NA), trauma (n = NA)Hand sewnmean: 10Um et al.,4R76 /10976 women48.653.9 %DIEP (n = 91), SIEA (n = 2), muscle sparing TRAM (n = 9); TUG (n = 7)BreastNRTumor (n = 109)Couplermean: 5.2Schmulder, et al.,5R473/226244 men and 229 women54.2NRNRH-N, breast, limbYestumor (n = NA), trauma (n = NA), reanimation (n = NA), other (n = NA)hand sewnmean: 7Hayler, et al.,6P99/10074 men and 25 women61.2 ± 12.1 (15.4–86.7)NRRadial forearm (n = 39), scapula tip (n = 20), ALT 8n = 15), fibula (n = 14), LD (n = 4), lateral border scapular (n = 4), parascapular (n = 2), infraclavicular (n = 1), gracilis (n = 1)H-NYestumor (n = 100)hand sewnmean: 9.4 ± 2.3Frost, et al.,7P20/219 men and 12 women35–68 (range)61.9 %Jejunum (n = 2), DIEP (n = 9), rectus abdominis (1), TRAM (n = 1), fibula (n = 6), ALT (n = 1), LD (n = 1)H-N, breast, limb, thoracic wallYes (n = 4)Tumor (n = 18, 85.7 %), Non tumor (n = 3, 14.3 %)hand sewnrange: 7–10Chang, et al.,8R439/440NR54.5 ± 15.837.6 %NRH–N (n = 364), breast (n = 53), extremity free flaps (n = 22).yesNRHand sewnNRLenz, et al.,9R69/6952 men and 17 women48NRGracilis (n = 47), LD (n = 25), rectus abdominis (n = 37); vastus lateralis (n = 1) [skin grafted free muscle flaps + NPWT]lower limbnoTumor (n = 6; 5 %); infection/chronic osteomyelitis (n = 14, 13 %), trauma (n = 55, 50 %), postoperative wound healing disorders (n = 30, 27 %), tissue defect due to impaired perfusion (n = 5, 5 %)Hand sewnAt least 7 days (the dangle of the leg was usually started about 1 week after surgery and the Doppler signal was checked after every step)Rozen, et al.,10R20 (20)6 women, and 14 men45.6 (15–73)0 %ALT (n = 2), parascapular (n = 1), LD (n = 12). lateral arm (n = 4), radial (n = 1)lower limbyesTrauma/trauma sequelae (n = 20)Hand sewn28 daysSmit, et al.,11R103 (121) [145 Doppler probes]103 women50±9.5 (range: 22–67)NRDIEP (n = 102)), SIEP (n = 15), SGAP (n = 4)breastNRTumor (n = 121)Hand sewn and coupler ( %NR)7 daysKimet al.,12R5 (5)3 menrange: 57–66 yearsNRChimeric thoracordorsal artery perforator free flap (n = 2), innervated chimeric latissimus dorsi muscle flap (n = ), chimeric latissimus dorsi and serratus anterior free flap (n = 1), free vascularised digastric lymph node transferH-N (n = 1), hand (n = 1),yesTumor (n = 1), trauma (n = 1), facial paralysis (n = 1), recurrent ulcer (n = 1), lymphedema (n = 1)Hand sewn7 daysWhitaker et al.,13R103 (121)103 womenNRNRDIEP (n = 106), SIEA (n = 15), SGAP (n = 4)breastnoTumor (n = 121)Hand sewnNROliver et al.,14R24 (24)NRNRnoGracilis, LD, TRAM, fibula, radial forearm, scapula, rectusNRnoNRHand sewn7–14 daysRozen et al.,15R8 (10)8 womenNRNRDIEP (n = 6), SGAP (n = 4)breastyesTumor (n = 10)Coupler (vein)7 daysPryor et al.,16R24 (24)16 men and 8 women57 (range: 14–78)57 (14–78)Radial forearm flap (n = 10), rectus abdominus (n = 6), fibula (n = 17), Anterolateral thigh (n = 13), scapula (n = 4)H–Nyes (n = 6)Tumor (n = 24)Hand sewnNRHo et al.,17R73 (75)54 men and 19 women59 (range: 17–84)32.9 %Fasciocutaneous radial forearm (n = 73), anterolateral thigfh (n = 17), iliac crest (n = 18) fibula (n = 13), scapula (n = 4), thoracordorsal system (n = 3), double flaps (radial forearm+iliac crest/fibula) (n = 2)H–NYes (n = 10)Tumor (n = 64), trauma (n = 1), osteoradionecrosis of mandible (n = 10)Hand sewnNRLevine et al.,18R84 (134)84 womenNRNRDIEP (n = 104), TUG (n = 10), IGAP (n = 2), PAP (n = 10), SGAP (n = 2), SIEA (n = 5), DFAP (n = 1)BreastYes (n = 2) [total revision based in clinical monitoring: n = 78]tumor (n = 134)Coupler3 daysSmit et al.,19R323 (323)(NR) men and (NR) women49.1 ±12.5 (range: 26–85)yes ( % NR)DIEP (n = NR), SGAP (n = NR), SIEA (n = NR), ALT (n = NR), radialis (n = NR), lateral arm (n = NR), LD (n = NR), fibula (n = NR), scapular (n = NR), gracilis (n = NR), serratus (n = NR)Breast (n = 251), H–N (n = 39), extremities (n = 33)NRNRHand sewnNRTeven et al.,20R100 (100)14 men and 86 women51.847 %VLNT (n = 100)upper/lower limb, H-Nyes (n = 100)LymphedemaHand sewn7 daysClert et al.,21R23 (23)17 men and 6 women58 (37–68)yes ( % NR)Fibula: n = 7; antebrachial: n = 15; scapular: n = 1H-NNRTumor (n = 20), osteoradionecrosis (n = 3)hand sewn14 daysWax et al.,22R1142 (1142)(NR) men and (NR) women67 (3–97)NRRadial/ulna: n = 506; ALT: n = 117; rectus: n = 94; LD: n = 101; fibula: n = 187; radial osteocutaneous: n = 56; scapula: n = 25; jejunum: n = 39; enteral: n = 8; other: n = 9H-NNRTumor (n = 1142)coupler5 daysHorne et al.,23R119 (125)NRNRNoFree gracilis: n = 125H–NNRLong-standing facial paralysisNRNRRosenber et al.,24R20 (20)NRNRNRFibula: n = 8; VRAM: n = 1; TRAM: n = 1; radial forearm: n = 1; ALT: n = 7; rectus abdominis: n = 1; jejunum: n = 1Limb: n = 6; thorax: n = 1; H-N: n = 12; breast: n = 1n = 20Tumor (n = 20)Hand sewnNRPark et al.,25R120 (120)75 men nd 45 women57yes (25 %)Scapula: n = 6; fibula: n = 54, radial forearm: n = 45, ALT: n = 17H–NNRTumor (n = 120)Hand sewn5 daysFujiwara et al.,26R120 (120)20 women, 80 men62.9 (21–94)22.5 %Radial forearm (n = 60), fibula (n = 28), anterolateral thigh (n = 15), scapula (n = 7), LD (n = 6), other (rectus, scapula + LD) (n = 4)H–N0.8 %Tumor (n = 79), other (n = 41)CouplerNRAbbreviations: ALT, anterolateral thigh; DIEP, deep inferior epigastric perforator; HN, head and neck; LD, latissimus dorsi; NPWT, negative pressure wound therapy; NR , not reported; P, prospective; Preop, preoperative; R, retrospective; SGAP, superior gluteal artery perforator; TRAM, transverse rectus abdominus myocutaneous; TUG, transverse upper gracilis.Table 2. Cook Swartz: indicators of effectiveness.Table 2. AuthorReduced/lost doppler signal [% on monitored flaps]Salvage rateFalse positive rates (FP/FP+TN)False negative rate (FN/FN+TP)Failure rateSensitivity-specificity-PPV-NPVPlacementGuillemaud et al.,1n = 46 (1″ %)92.0 %1.8 %68.4 %1.8 %Sensitivity: 65.8 %;Specificity: 98.2 %; Positive predictive value: 80.7 %; Negative predictive value: 100 %n = 318: A; n = 74: A ± V; n = 4: VLeibig et al.,2n = 29 (19.7 %)63.0 %1.7 %37 %6.8 %sensitivity: 82.4 % (around the artery), 84.6 % (around the vein), (p=0.87); specificity: 89.2 % (around the artery), 96.1 % (around the vein), (p=0.17); PPV: 82.7 % (around the artery), 61.1 % (around the vein), (p=0.056); NPV: 96.7 % (around the artery), 94.2 % /around the vein), (p= 0.55)n = 68: A; n = 79: VPaprottka, et al.,3n = 8 (22.9 %)37.5 %7.4 %25 %5.7 %sensitivity 75 %, specificity 93 %, PPV 75 %, NPV 92.6 %n = 35:VVUm et al.,4n = 11 (10.1 %)81.8 %1 %0 %1.8 %sensitivity: 100 %; specificity: 99 %; PPV: 91.7 %; NPV: 100 %n = 109: VSchmulder, et al.,5n = 36 (15.9 %)95 %1.6 %0 %12.1 %sensitivity: 100 %; specificity: 98.4 %; PPV: 91.7 %; NPV: 100 %n = 226: VHayleret al.,06n = 17 (12 %)75.0 %1 %12 %2 % [partial]sensitivity: 87.1 %; specificity: 85.7 %; PPV: 98.8 %; NPV: 33.3 %n = 100: A+VFrostet al.,7n = 3 (14.3 %)33.3 %0 %33.3 %66.7 % [partial and complete]sensitivity: 66.7 %; specificity: 100 %; PPV: 100 %; NPV: 95 %n = 3: A+V; n =13: V; n =5: AChanget al.,8n =56 (12.8 %)62.5 %11.6 %22.2 %4.8 %sensitivity: 77.8 %; specificity: 88.4 %n = 267: A; n =101: V; n = 71: A+VLenzet al.,9n = 14 (20.3 %)80 %3.6 %7.7 %4.3 %sensitivity: 92.3 %; specificity: 96.4 %; PPV:85.7 %; NPV: 98.2 %n =69: VRozenet al.,10n = 2 (10 %)100 %0 %0 %0 %sensitivity: 100 %; specificity: 100 %; PPV:100 %; NPV: 100 %n =20: VSmitet al.,11n = 15 (12.4 %)86.7 %6.7 %0.9 %1.7 %sensitivity: 100 %; specificity: 99.2 %; PPV:93.3 %; NPV: 100 %n = 145: V [in 51 flaps, a second venous anastomosis was done]Kim et al.,12n = 1 (20 %)100 %0 %0 %0 %sensitivity: 100 %; specificity: 100 %; PPV: 100 %; NPV: 100 %VWhitaker et al.,13n = 11 (9.1 %)80 %0.9 %0 %1.7 %sensitivity: 100 %; specificity: 99.1 %; PPV:90.9 %; NPV: 100 %n = 121: VOliver, et al.,14n = 2 (8.3 %)100 %0 %0 %0 %sensitivity: 100 %; specificity:100 %; PPV:100 %; NPV: 100 %n = 24: VRozenet al.,15N = 0\0 %0 %0 %sensitivity: 100 %; specificity:100 %; PPV:100 %; NPV: 100 %n = 10: VPryoret al.,16N = 6 (25 %)75 %14.3 %0 %4 %sensitivity; 100 %; specificity: 85.7 %; PPV: 50; NPV: 100 %n = 12: A; n =11: V; n =1: A+VHo et al.,17N = 9 (12 %)62 %4.5 %33.3 %6.7 %sensitity: 66.7 %; specificity: 95.5 %; PPV: 66.7 %; NPV: 95.5 %n = 67: A; n =7:V; n =1: A+VLevine et al.,18N = 20 %0.8 %50 %2.2 %sensitivity: 50 %; specificity: 99.2 %; PPV: 50 %; NPV= 99.2 %n = 134: VSmit, 200919n = 37 (10.4 %) (excluding one case of accidental remove of the device by the patient)69 %0.6 %0 %31 %sensitivity: 100 %; specificity: 99.4 %; PPV: 71.4 %; NPV = 100 %n = 323: VTeven et al.,20n = 5 (5 %)100 %2.1 %0 %0 %sensitivity: 100 %; specificity: 97.7 %; PPV: 60 %; NPV = 100 %n = 100: AClert et al.,21n = 3 (13 %)100 %9.1 %0 %0 %sensitivity: 100 %; specificity: 90.9 %; PPV: 33.3 %; NPV: 100 %n = 20: V; n = 3: AWax et al.,22n = 134 (11.7 %)82 %0.8 %13 %2.5 %sensitivity: 87 %; specificity: 99 %; PPV: 89.3 %; NPV: 99.1 %n = 43: V; n =1099: AHorner et al.,23NRNRNRNRNRsensitivity: 100 %, specificity: 88 %; PPV: 41 %; NPV: 100 %NRRosenberg et al.,24n = 8 (40 %)12.5 %36.8 %0 %0 %sensitivity: 100 %; specificity: 63.2 %; PPV: 12.5 %; NPV: 100 %n = 12: V; n =6: A; n = 1: unspecified; n =1: flap perforatorPark et al.,25n = 23 (19.2 %)71.4 %10.2 %0 %4.2 %sensitivity: 100; specificity: 89.8 %; PPV: 52.2 %; NPV: 100 %n = 120: AFujiwara et al.,26n = 1 (0.8 %)0 %2.9 %90.9 %0.8 %sensitivity: 9.1 %, spexificity: 97.1 %, PPV: 25 %, NPV: 90.9 %n = 120: AAbbreviations: A, artery; A+V, artery + vein; FN, false negative; FP, false positive; NPV , negative predictive value; PPV, positive predictive value; TN, true negative; TP, true positive; V = veinTable 3Synovis: characteristics of enrolled patients.Table 3. Authortype of studyPatients/flapFlow coupler anastomosisSexAge (mean)Pre-operative radiotherapyFlap typeRecipient vesselFlap locationBuried flaps (also) includedFlap indicationSynovis duration (days)Um, 20144R74 (111)NR74 women50.347.3 %DIEP (n = 90), SIEA (n =6), MS TRAM (n =10), TUG (n =3), SGAP (n =2)NRbreastNRtumor (n =74)mean: 4.8 daysCreasy, 202327R106 (126)185 (NR)106 womenNRNRDIEP (n =45), PAP (n =21), ALT (n =41), TFL (n =2), VL (n =1), TDAP (n =2), LD (n =1), RFFF (n =4), SCIP (n =1), MFC periosteal (n =6)NRNRyes ( %NR)tumor(n =106)3–5 daysShtarbanov, 202428R16 (18)19 (n =3: 2 mm; n =13: 2.5 mm; n =2: 1.5 mm; n =1: 3 mm)NRNRNRNRNRhand, breast, lower limbyes ( %NR)tumor (n =16)NRZhang, 201229R18(19)20 (n = 5: 2 mm; n =8: 3 mm; n =7: 2.5 mm)11 women and 7 men20–76NRLD (n =2), fibula (n =7), radial forearm (n =2), anterolateral thigh (n =4), DCIA (n =2), scapula (n =1), lateral arm (n =1)cefhalic (n =1), external jugular (n =6), internal jugular (n =1), anterior jugular (n =1), facial (n =9), retromandibular (n =1), superficial temporal (n =1)head and neckyes ( %10.5 %)tumor (n =11), ostreomyelitis (n =2), osteoradionecrosis (n =2), other (n =3)5–6 daysChadwig, 201930R14(26)24 (n =12: 2.5 mm; n = 8: 3 mm; n =2: 3.5 mm)14 women39 (24–58)NRDIEP (n =26)IMVbreastyes (100 %)tumor (n =7), risk reducing mastectomy (n =7)4.5 daysFujiwara, 201826R120 (120)191 (2.5 mm, range, 1.5–4.0)20 women, 80 men62.9 (21–94)22.5 %radial forearm (n =60), fibula (n =28), anterolateral thigh (n =15), scapula (n=7), LD (n=6), other (rectus, scapula+LD) (n=4)external jugular (n=85), common facial (n=53), branch of common facial (n=16), facial (n=16), superior thyroid (n=10), internal jugular (n=10), anterior jugular (n=6), other (n=3)H-Nyes (NR %)tumor (n=79), other (n=41)NRAbbreviations: ALT, anterolateral thigh; DCIA, deep circumflex iliac artery; DIEP, deep inferior epigastric perforator; HN, head and neck; LD, latissimus dorsi; MFC, medial femoral condyle; MS- TRAM, muscle sparing transverse rectus abdominus myocutaneous; NPWT = negative pressure wound therapy; NR, not reported; P, prospective; PAP, profunda artery perforator; Preop, preoperative; R, retrospective; RFFF, radial forearm free flap; SCIP, superficial circumflex iliac perforator; SGAP, superior gluteal artery perforator; TFL, tensor fascia latae; TDAP, thoracodorsal artery perforator; TRAM, transverse rectus abdominus myocutaneous; TUG, transverse upper gracilis; VL, vastus lateralis;Table 4. Synovis: indicators of effectiveness.Table 4. AuthorReduced/Lost Doppler Signal [ % On Monitored Flaps]Salvage RateFalse Positive Rates (FP/FP+TN)False Negative Rate (FN/FN+TP)Failure RateSensitivity-Specificity-PPV-NPVAnastomosisComplications Related To The DeviceUm, 201444.5 %50 %1.9 %0 %0.9 %sensitivity: 100 %, specificity: 98.1 %, PPV: 66.7 %, NPV: 100 %E-E0.9 % vein kinking caused by the deviceCreasy, 2023272.4 %100 %0 %0 %0 %NRNRnoShtarbanov, 20242831.3 %100 %20 %0 %5.5 %sensitivity: 100 %, specificity: 80 %, PPV: 60 %; NPV: 100 %E-E16.7 % vein twisting caused by the deviceZhang, 20122930 % [due to: n=2: inadvertent intraoperative removal; n=2: vessel kinking; n=2: equipment failure]100 %0 %0 %0 %sensitivity: 100 %, specificity: 100 %, PPV: 100 %; NPV: 100 %NR10.5 % vein twisting caused by the deviceChadwig, 2019304.2 %100 %4.2 %0 %0 %sensitivity: 100 %, specificity: 95.8 %, PPV: 0 %; NPV: 100 %NRnoFujiwara, 2018268.3 %90 %13.6 %0 %0.8 %sensitivity:100 %, specificity: 86.4 %; PPV: 44 %; NPV: 100 %NRnoAbbreviations: E-E = end to end; FN = false negative; FP = false positive; NPV = negative predictive value; PPV = positive predictive value; TN = true negative; TP = true positive; V = vein
Data were recorded and tabulated using Microsoft Excel (Microsoft Corp., Redmond, Washington, Version 2210).
Quality assessment
The risk of bias of each study is reported in Supplementary Table 1.
Results
From January 2019 to February 2024, 179 free flaps (see table 1) were operated on at our institution. Of these, 52 were monitored using implantable dopplers of which 39 were Synovis flow couplers (Synovis Life Technologies, Inc., St. Paul, MN) and 14 Cook Swartz (Cook Medical, Bloomington, IN). Of the 39 Flow Couplers, 29 were used in breast and nine in head and neck surgery, whereas of the 14 Cook Swartz, two were used in breast surgery and 12 in head and neck surgery. All the monitored flaps were buried. With the flow couplers, we had one case of false positivity and one case of flap failure, both in the head and neck group. These entailed a specificity of 97.2 % and a PPV of 50 %, with 100 % sensitivity and NPV. The false-positive case corresponded to a flap where the signal was barely detectable, yet clinically the flap appeared to be viable; conversely, the failed case involved a condylar flap that had already experienced complications intraoperatively. The Cook Swartz performed better, with only one case of flap failure, in a true positive labelled patient undergone head and neck surgery.
To understand if we were getting the most out of these devices, the literature was systematically explored. The search using Cook Swartz thesaurus identified 116 articles while that of Synovis Flow Coupler 25 articles. After removing duplicates (n = 41 and n = 10, respectively) and articles that did not meet the inclusion criteria (n = 51 and n =7, respectively), we collected 26 and six articles, respectively (see Tables 1,2,3,4).
Table 7, Table 8 show a summary of the indicators of effectiveness of the two devices according to the literature.
Our results (Table 5, Table 6) are in line with those reported in literature, with a worse performance in terms of specificity and PPV of Synovis as compared to Cook Swartz.Table 5. Our casistics.Table 5:Conventional anastomosisImplantable DopplerFlap failuren = 179n = 127 (70.9 %)n = 52 (29.1 %)n = 2 (1.1 %)Head and neck: n = 120 (67 %)Breast: n = 46 (25.7 %)Upper limb: n = 10 (5.6 %)Lower limb: n = 3 (1.7 %)Table 6. Our results.Table 6:N = 38 flow couplers (n=29 breast; n=9 head and neck)N =14 Cook Swartz (n=2 breasts, n=12 head and neck)N =36 true negativesN =1 true positive (failed) (head and neck)N = 1 false positive (head and neck)N = 0 false negativeN = 13 true negativesN = 1 true positive (failed) (head and neck)n = 0 false positiven = 0 false negativeSensitivity: 100 %Sensitivity: 100 %Specificity: 97.1 %Specificity: 100 %PPV: 50 %PPV: 100 %NPV: 100 %NPVAbbreviations: NPV, negative predictive value; PPV, positive predictive valueTable 7Cook Swartz: summary of the pertinent literature.Table 7:Cook Swartz26 articles4102 patients e 4038 flapsTime to Doppler removal3–28 daysFlap revision according to changed CS signal:0 %-40 %Salvage rate0–100 %Failure rate0- 66.7 %FPR0–36.8 % (81 % of studies ≤ 10 % and *54 % ≤ 2 %)FNR0 %-90.9 % (46 % of studies ≤ 10 % and 23 % > 30 %)Sensitivity9–100 %; > 90 % in 62 % of studies (up to 100 % in 58 %)Specificity63–100 %; > 90 % in 73 % of studiesPPV12.5 % -100 %; >90 % in 38.5 % of studiesNPV33.3 % -100 %; > 90 % nel 96.2 %Table 8. Synovis: summary of the Pertinenti literature.Table 8. Synovis7 articles348 patients and 420 flapsTime to Synovis removal:4.8–6 daysFlap revision according to changed FC signal2.4–30 %Salvage rate50–100 %Failure rate0- 5.5 %FPR0–20 %FNR0 %Sensitivity100 %Specificity80–100 %*PPV0–100 %NPV100 %
Discussion
For fasciocutaneous flaps transferred to body regions with easy observation, the only monitoring required is clinical.6^,^8 Buried flaps, muscle flaps without monitor islands, skin grafted muscle flaps, quite the opposite, can only be monitored accurately with the use of implantable probes or exposed paddles for clinical assessment.6^,^8 Implantable probes also allow for the postoperative concept of negative pressure wound therapy (NPWT) of free muscle flaps.8^,^9
In our daily practice, the criterion upon which we base the decision to use an implantable Doppler is whether the flap is buried. This is the rationale behind the use of Doppler monitoring in the head and neck as well as breast reconstructions, where flaps are typically buried. In head and neck reconstructions, for example, nearly all flaps are buried or semi-buried, and the use of a non-clinical monitoring system becomes necessary due to the frequent intraoral location of the flap, which is subject to color and turgor changes caused by saliva (maceration tends to give the flap a pale appearance), as well as the difficulty in having the patient open their mouth due to spasms in the postoperative period. In contrast, for free flaps monitoring in the extremities (lower/upper limbs), such an expensive system is not recommended, as the flaps are usually not buried and clinical monitoring remains the gold standard. In clinically monitorable flaps, the use of the probes may be beneficial only if it also facilitates faster performance, as is the case with the Synovis device, which functions as a coupler and releases the probe simultaneously with the suturing process (being a coupler it also helps to ensure mechanical patency). Conversely, the Cook-Swartz system consists solely of a probe that is positioned on the anastomosis after it has been completed.
The main flaws of clinical monitoring are its dependence on clinical experience and the fact that when a vascular problem becomes clinically evident, often the flap is irreparably damaged.13 In most cases, the ability to recognize a compromised flap and subsequent early re-exploration is the key to successful salvage, as most successful salvages occur within the first 24 hours.6
The implantable Doppler probes allow the direct measurement of blood flow since a monitor is placed onto the pedicle thus helping detect flap compromise before clinical ischemia becomes evident.3 The early detection of flap compromise and prompt return to the operating room can influence free flap salvage rates by returning perfusion to the flap before the no-reflow phenomenon occurs.4^,^5 In the current literature, the rate of salvage varies from 33 % to 89 %.4
The two devices allowing a continuous monitoring of flow across the anastomosis are the Cook Swartz and the Synovis Flow Coupler. These implantable probes have the strength of continuous flow evaluation of the pedicle flow opposite to the other monitoring methods (microdyalisis, clinical assessment, near-infrared spectroscopy, microdialysis, laser Doppler flowmetry combined with tissue spectrophotometry or modified oxygen microelectrode …) which only provide indirect evidence of impaired pedicle blood flow by measuring capillary perfusion and therefore producing critical latency.6^,^8 No Difference (p > 0.05) between the two devices in terms of their accuracy in detecting vessel compromise have been identified in the clinical setting.4 The singular advantage of the Flow Coupler is that it allows the Doppler to be placed simultaneously at the time of anastomosis, eliminating the need for any additional intraoperative procedures.4
Different studies of the Cook Swartz implantable Doppler showed a significant increase in flap salvage rates contrary to clinical assessment (96.14 % vs. 89.27 %)5^,^20 without increasing the rate of false-positive operative re-explorations and concluded that it could be used as a stand-alone measure of flap status.4, 5, 6 In buried flaps, the difference in flap salvage between implantable Dopplers and clinical exam is even larger (94 % vs 40 %) because buried flaps cannot be evaluated clinically and it is difficult to confirm that they are healthy without operative exploration. The risk of an increased false positive rate is not a serious drawback for free flaps that are not buried, because false-positive signals can be confirmed as falsely positive by clinical examination and ignored. However, for completely buried free flaps, there is no accepted rapid and reliable confirmatory test, so one must resort to operative exploration, which is an invasive procedure that is both time consuming and labor intensive.24
The risk of false negatives has been reported for the Cook Swartz venous placement (an arterial signal could persist even in the setting of a venous thrombosis)31 and for both the devices in head and neck flaps where there exists the problem of transmitted vessel interference, due to the proximity of the large-calibre vessels, namely the carotid artery and the internal jugular vein leading to FN. In the neck, venous signals are also prone to false positive findings, because of their variation according to the head position and to the respiratory cycle. When the venous signal appears to be missed, two dynamic manoeuvers have been described to increase the venous flow and the signal perception reducing the false positive rate: the “whoosh test” (which consist of exerting a digital pressure over the flap) and the “heave test” (a Valsalva Manoeuver).21^,^22
Our early experience, combined with literature findings, has progressively prompted us to prefer the use of the Flow Coupler in buried diep flap (where it also aids in the anastomosis making) while reducing its application in buried head and neck flaps so as to reduce the false positive rates and the subsequent unnecessary operating room take back. In DIEP flaps, the most critical point is the venous anastomosis, which is technically demanding, as the mammary artery exhibits significant pressure and is less likely to undergo occlusion. That is why, in DIEP flaps, we tend to place the probe on the vein. Conversely, in head and neck reconstructions, where venous pressure is lower (due to variations corresponding to the respiratory cycle, etc.), we routinely perform two venous anastomoses and one arterial anastomosis. In this scenario, occlusion of both veins is less likely, making the artery the critical point to monitor. Therefore, in head and neck cases, we typically position the doppler (Cook Swartz) probe on the artery.
In the head and neck surgery, our current trend is to use the Cook Swartz placed around the arteries, being these less prone to positional changes and respiratory cycle oscillations.
An important advantage of implantable dopplers as direct monitoring techniques versus the clinical monitoring is also observed during the intraoperative period, due to disclosure of any kind of problem (blood disturbance and pressure on the vascular pedicle), from the moment, the implantable Doppler was connected until patient education about appropriate neck positions and inappropriate movements based on the signal shown on the monitor's screen.5^,^11
The system is based on a “yes” versus “no” response (audible signal vs signal absence) and does not require any interpretation or medical education. The patients themselves can alert the medical staff if the signal shades away. Furthermore the presence of a constant sound reassures and relieves anxiety on patients who can personally monitor their flap status. Among the limits of the present study we have to cite its retrospective design, the small cohort of patients included and the fact that the patients were not randomized to one device or another but the first were monetarized using Synovis and the last by Cook Swartz after the first case of false positivity. Furthermore data span over a period of five years, possibly reflecting a learning curve in our ability to use them. Another important drawback of this study is the lack of a statistical analysis between the performances of the two devices. Thus our results, although in line with the current literature, must be read with caution.
Future studies should focus on AI-assisted Doppler interpretation and cost-analysis comparisons between the two systems in different body parts.
Conclusion
Implantable dopplers are a valid supplement to clinical monitoring which cannot be considered the gold standard for all free flaps. Buried flaps, skin grafted muscle flaps, intra-oral flaps, flaps in dark-skin patients are better monitored with implantable dopplers, which also ensure a continuous check of pedicle flow, thus revealing vascular problems in advance (before the no reflow phenomenon occurs) also in fasciocutaneous flaps. To reduce the risk of false positive results (which in buried flap cannot be excluded without theatre take back) we use the Cook Swartz doppler probe around the artery in the head and neck flaps, while we use the Synovis flow coupler in diep flaps where the anatomical location of recipient vessel is less prone to variations of the flow.
Funding
None.
Declaration of competing interest
The authors have no conflict of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guillemaud J.P.Seikaly H.Cote D.Allen H.Harris J.R.The implantable cook-swartz doppler probe for postoperative monitoring in head and neck free flap reconstruction Arch Otolaryngol Neck Surg 1347200872910.1001/archotol.134.7.72918645123 · doi ↗ · pubmed ↗
- 2Leibig N.Ha-Phuoc A.Stark G.B.Retrospective evaluation of diagnostic accuracy of free flap monitoring with the Cook-Swartz-Doppler probe in head and neck reconstruction J Cranio-Maxillofac Surg 471220191973197910.1016/j.jcms.2019.11.00131810844 · doi ↗ · pubmed ↗
- 3Paprottka F.J.Klimas D.Krezdorn N.Schlarb D.Trevatt A.E.J.Hebebrand D.Cook— Swartz doppler probe surveillance for free flaps—Defining pros and cons Surg 06012020 e 42e 4610.1055/s-0040-17029221 PMC 705406132133414 · doi ↗ · pubmed ↗
- 4Um G.T.Chang J.Louie O.Implantable Cook-Swartz Doppler probe versus Synovis Flow Coupler for the post-operative monitoring of free flap breast reconstruction J Plast Reconstr Aesthet Surg 677201496096610.1016/j.bjps.2014.03.03424767693 · doi ↗ · pubmed ↗
- 5Schmulder A.Gur E.Zaretski A.Eight-year experience of the Cook-Swartz Doppler in free-flap operations: microsurgical and reexploration results with regard to a wide spectrum of surgeries Microsurgery 31120111610.1002/micr.2081620683856 · doi ↗ · pubmed ↗
- 6Hayler R.Low T(Hubert)Fung K.Nichols A.C.Mac Neil S.D.Yoo J.Implantable doppler ultrasound monitoring in head and neck free flaps: balancing the pros and cons Laryngoscope 1316202110.1002/lary.2924733141464 · doi ↗ · pubmed ↗
- 7Frost M.W.Niumsawatt V.Rozen W.M.Eschen G.E.T.Damsgaard T.E.Kiil BJ.Direct comparison of postoperative monitoring of free flaps with microdialysis, implantable cook-swartz doppler probe, and clinical monitoring in 20 consecutive patients Microsurgery 354201526227110.1002/micr.2233125285732 · doi ↗ · pubmed ↗
- 8El Chang A Ibrahim Zhang H.Deciphering the sensitivity and specificity of the implantable doppler probe in Free Flap I’•Jonitoring Plast Reconstr Surg 1373201697197610.1097/01.prs.0000480016.20326.8f 26910681 · doi ↗ · pubmed ↗