Dental Caries and Oral Mucositis Among Children Undergoing Cancer Therapy at Kenyatta National Hospital, Kenya: A Cross-Sectional Study
Diana A Okello, Mary Masiga, Marjorie Muasya

TL;DR
This study examines dental caries and oral mucositis in Kenyan children undergoing cancer therapy, highlighting the need for dental care integration into cancer treatment.
Contribution
The study provides new prevalence data on dental caries and oral mucositis in Kenyan pediatric cancer patients and advocates for dental involvement in cancer care.
Findings
Dental caries prevalence was 58.8%, higher in children aged six to 12 years.
Oral mucositis was observed in 28.4% of children, mostly Grades I and II.
Only 2.9% of children had undergone dental assessment before cancer therapy.
Abstract
Background Dental caries and oral mucositis are often experienced by children undergoing antineoplastic therapy. Understanding the prevalence and characteristics of these complications is essential for developing targeted supportive oral care strategies to improve overall treatment outcomes and the quality of life of the children. Methods This study employed a cross-sectional design with 102 children aged three to 12 years undergoing cancer therapy at Kenyatta National Hospital, Kenya. Participants were selected through purposive sampling. Data was collected via a structured questionnaire and clinical oral examination, with dental caries assessed using the decayed, missing, and filled teeth (dmft, primary teeth)/Decayed, Missing, and Filled Teeth (DMFT, permanent teeth) index, and oral mucositis assessed using the WHO Oral Mucositis Scale (1979). Results Acute lymphoblastic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4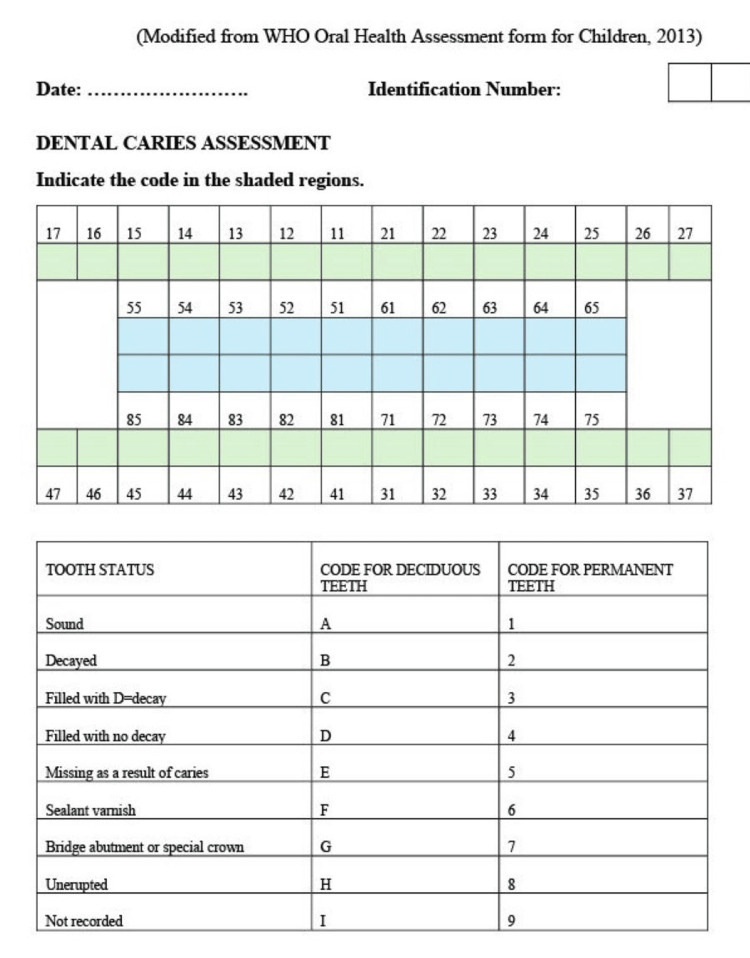 Figure 5
Figure 5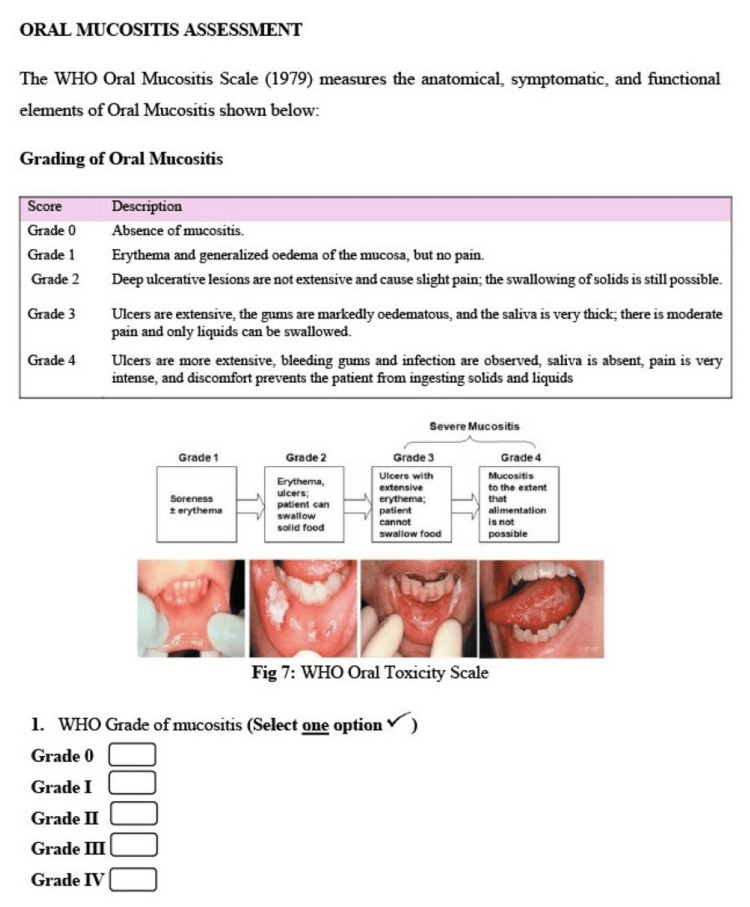 Figure 6
Figure 6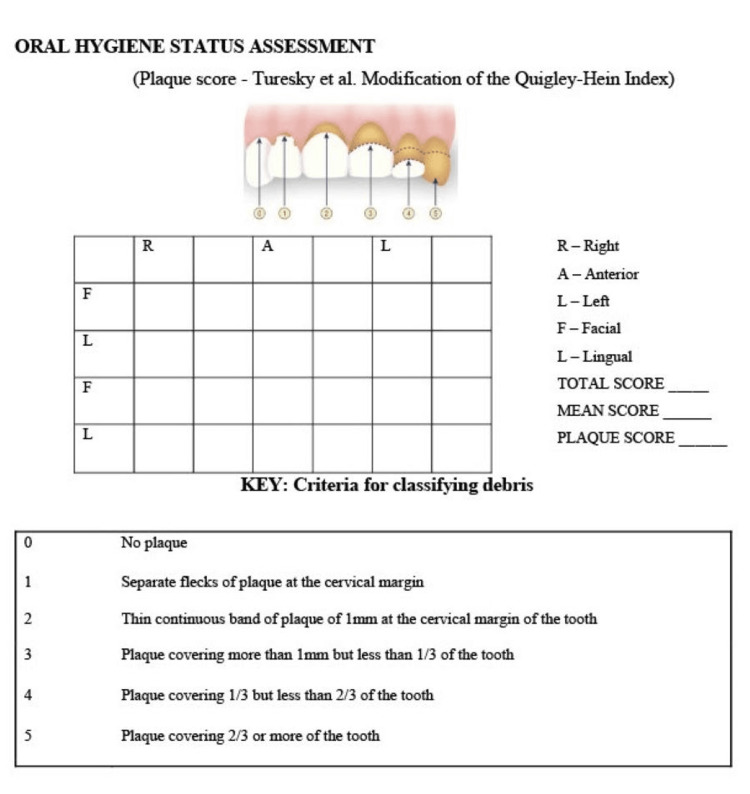 Figure 7
Figure 7| Characteristic | Category | d | m | f | dmft | ANOVA |
| M +SD | M +SD | M+SD | M+SD | |||
| Gender | Male | 3.02 +3.76 | 0.0 | 0.0 | 3.02+3.76 | F(1,100) = 2.38, p=0.126 |
| Female | 1.94 +3.07 | 0.0 | 0.02+0.15 | 1.96+3.08 | ||
| Characteristic | Category | D | M | F | DMFT | ANOVA |
| M+SD | M+SD | M+SD | M +SD | |||
| Gender | Male | 0.13 +0.61 | 0.04+0.27 | 0.00 | 0.16+0.66 | F(1,100) = 0.67, p=0.796 |
| Female | 0.06+0.32 | 0.0 | 0.06+0.44 | 0.13+0.74 |
| Characteristic | Category | Caries prevalence | Pearson’s Chi-Square | |||||
| Present | Absent | χ2 | df | p-value | ||||
| n | % | n | % | |||||
| Treatment modalities | CT alone | 35 | 57.4 | 26 | 42.6 | 0.992 | 5 | 0.963 |
| CT and RT | 4 | 57.1 | 3 | 42.9 | ||||
| RT alone | 1 | 100 | 0 | 0.0 | ||||
| CT and Surgery | 14 | 58.3 | 10 | 41.7 | ||||
| Surgery alone | 2 | 66.7 | 1 | 33.3 | ||||
| CT, RT, & Surgery | 4 | 66.7 | 2 | 33.3 | ||||
| Overall | 60 | 58.8 | 42 | 41.2 | ||||
| Variable Category | Oral mucositis | Test | ||||||
| Present | Absent | |||||||
| n | % | n | % | χ2 | df | p-value | ||
| Gender | Male | 16 | 29.1 | 39 | 70.9 | 0.026 | 1 | 0.873 |
| Female | 13 | 27.7 | 34 | 72.3 | ||||
| Age categories (years) | 3 – 5 | 15 | 26.3 | 42 | 73.7 | 0.284 | 1 | 0.594 |
| 6 – 12 | 14 | 31.1 | 31 | 68.9 | ||||
| Oral Mucositis Grades | Age groups years | Test | ||||
| 3 - 5 (N=57) | 6 - 12 (N=45) | χ2 (df) | p-value | |||
| N | % | N | % | |||
| Grade 0 Grade I Grade II Grade III Grade IV | 42 | 57.5% | 31 | 42.5% | 3.514 (3) | 0.319 |
| 6 | 46.2% | 7 | 53.8% | |||
| 9 | 64.3% | 5 | 35.7% | |||
| 0 | 0.0% | 2 | 100.0% | |||
| 0 | 0.0% | 0 | 0.0% | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral health in cancer treatment · Head and Neck Cancer Studies · Cancer Diagnosis and Treatment
Introduction
Approximately 80% of global childhood cancer cases occur in low- and middle-income countries (LMICs), a disparity primarily attributed to the predominance of younger populations within these regions [1]. The management of childhood cancers involves multiple therapeutic modalities, including chemotherapy, radiotherapy, surgery, and, more recently, haematopoietic stem cell transplantation (HSCT) and immunotherapy [2-4]. These treatment options are frequently associated with oral complications, such as dental caries, oral infections, oral mucositis, and xerostomia [5]. These oral complications can significantly affect the nutritional status and overall health, including the quality of life of paediatric oncology patients [6,7]. Consequently, a thorough understanding of the regional paediatric cancer burden and the prevalence of therapy-related oral morbidities is essential for informing effective, context-specific supportive care strategies that enhance treatment outcomes and patient well-being.
Chemotherapy is associated with oral complications in approximately 40% of patients, with the prevalence rising to over 90% in children under the age of 12 years [7-9]. Eighty to 100% of patients receiving radiotherapy directed to the head and neck region inevitably develop radiation-induced mucositis, and the addition of chemotherapy significantly increases this risk [10-12]. Approximately 80% of children undergoing HSCT experience oral mucositis, xerostomia, dysgeusia, as well as both local and systemic infections [13,14]. The most frequently reported oral toxicities linked with immunotherapeutic agents include low-grade mucositis, lichenoid mucosal reactions, dysgeusia, and xerostomia [15,16]. Despite these known complications, data on the immunotherapy-induced oral adverse events in paediatric patients remains scarce.
Several studies examining the oral complications of antineoplastic therapy have identified dental caries and oral mucositis as the most prevalent conditions. Dental caries is a non-communicable biofilm-driven disease, influenced by prolonged exposure to cariogenic dietary habits, resulting in the progressive demineralization of tooth structure [17]. This condition is largely preventable, and its prevention plays a vital role in the oral healthcare of paediatric patients undergoing cancer treatment [18-20]. Wang et al. investigated 39 children diagnosed with acute lymphoblastic leukemia (ALL) undergoing chemotherapy and compared them with age-matched counterparts who were not diagnosed with ALL. This Chinese study reported that 69.2% of all documented oral conditions were dental caries. This high prevalence was linked to the methotrexate’s mucosal cytotoxic effects, which compromised oral hygiene. Moreover, chemotherapy-induced nausea and vomiting often result in children consuming smaller, more frequent meals, which increases the risk of dental caries due to extended exposure of the teeth to dietary sugars. Microbiological analysis of supragingival plaque revealed a higher abundance of Lactobacillus species in the chemotherapy group, further predisposing these children to caries progression. Key contributing factors therefore included frequent eating, poor oral hygiene, shifts in the oral microbiome, and high sugar consumption [21].
Oral mucositis (OM) is characterized by inflammation of the oral mucosa, which is a widespread and often debilitating complication of antineoplastic therapy [7]. Younger age, neutropenia, poor oral hygiene, compromised nutritional status, and the type of malignancy, often influence the development of OM [8]. OM usually develops within five to seven days after starting chemotherapy and can continue throughout the treatment duration, a pattern observed by Cheng et al. in China [22]. Ulcerations generally emerge within seven to 10 days, often presenting with minimal inflammatory infiltration at the margins and requiring up to 14 days to heal. In severe cases, individual lesions can coalesce into large, shallow ulcers with necrotic bases [23-25]. Radiation-induced mucositis (RIM), on the other hand, usually develops around 14 days after the start of radiotherapy and resolves within three to four weeks. Clinically, RIM is marked by ulcers with poorly defined borders and lacks the erythematous halo commonly seen in chemotherapy-induced mucositis. RIM predominantly affects the floor of the mouth, buccal mucosa, and soft palate, while sparing the gingiva and tongue [26]. These painful lesions can severely impair nutrition, oral hygiene practices, and commonly increase susceptibility to secondary infections.
These oral complications significantly contribute to the overall disease burden among paediatric cancer patients. Addressing the current knowledge gap on the prevalence of dental caries and oral mucositis in Kenyan children undergoing cancer therapy, the findings of this study aim to enrich the existing body of literature and provide foundational data to guide future research and inform context-specific clinical management strategies.
Materials and methods
Study design
Ethical approval to conduct the study was granted by the Kenyatta National Hospital (KNH) Ethics and Research Committee at University of Nairobi (Ref. No. P796/10/2021). This study employed descriptive cross-sectional design at KNH. KNH provides chemotherapy, surgery, and radiotherapy as its main cancer treatment modalities; however, HSCT and immunotherapy were not available during data collection. The hospital has an official bed capacity of approximately 1,800, including 400 pediatric beds, although actual occupancy often exceeds 3,000 due to high patient demand. Paediatric oncology patients are admitted across multiple inpatient wards, with an average of 140 children receiving cancer treatment.
Patient recruitment
Considering the study design, the sample size was determined using Cochran’s formula (Z test) and computed as follows [27]:
Where n = sample size; Z = value from the standard normal distribution for 95% confidence level = 1.96; p = prevalence of dental caries and oral mucositis among paediatric oncology patients = 0.5; and d = allowable error (absolute) = 0.05.
Therefore, nonetheless, the sample size calculated is for a study population >10,000 and the desired sample size is for a study population <10,000, the sample size was corrected for a study population <10000:
Where n = desired sample size for a study population <10000; n_0_ = sample size derived for a study population >10000; and N = estimated size of the study population (patients) = 140.
\begin{document}n= n_0/(1+((n_0- 1))/N)\end{document}
\begin{document}n=384/(1+((384-1))/140)\end{document}
n=102.
Sample size calculation and finite population correction (FPC) for a paediatric oncology cohort (N=140). Applying the FPC reduced the large-population estimate to achieve the sample size of 102, with a negligible effect on precision.
Therefore, a sample size of 102 paediatric oncology children were enrolled into the study using purposive sampling, based on their eligibility and availability during the study period. Children aged three to 12 years undergoing cancer treatment at the study site were eligible if parental or guardian consent was obtained, with assent provided by the child when appropriate. Children who were critically ill or in medical isolation at the time of recruitment were excluded.
Data collection
Data was collected using two primary methods: a structured questionnaire (Appendix 1) developed by the principal investigator (PI) and a clinical examination (Appendix 2). The questionnaire was adapted and modified from the World Health Organization (WHO) Simplified Oral Health Questionnaire for Children to include a section on medical history, and was pre-tested on 10% of the target sample prior to the main study [28]. Parents or guardians served as the informants for the sections on dietary habits and oral hygiene practices. The ward nurse thereafter prepared the list of all eligible children, and intraoral examinations were subsequently conducted by the PI without prior access to individual medical histories or treatment regimens.
The clinical examinations were conducted by the PI under field conditions using natural light. Each child underwent an intraoral assessment to evaluate the overall oral hygiene status and the presence of oral mucositis and dental caries. Dental caries was assessed by visual-tactile examination using the WHO Oral Health Assessment Form for Children (2013) [28]. Caries experience was recorded with the decayed, missing, and filled teeth (dmft) index for primary teeth and the Decayed, Missing, and Filled Teeth (DMFT) index for permanent teeth, applied as appropriate in mixed dentition, in accordance with WHO Oral Health Survey criteria [28]. Teeth were dried with gauze before inspection. Caries was identified by the presence of white chalky lesions in the cervical region, visible loss of tooth structure, or evidence of previous treatment, such as restorations or extractions. Oral mucositis was evaluated by gently retracting the lips and buccal tissues, with its presence and severity assessed according to the WHO Oral Mucositis Scale (1979) [29]. Oral hygiene was assessed based on dental plaque accumulation. Each child chewed a disclosing tablet for one minute and spread the dye using the tongue. After rinsing, plaque was assessed on six index teeth following the Sillness and Löe criteria [30]. The extent of plaque on buccal and lingual surfaces was quantified using the modified Quigley-Hein Plaque Index by Turesky et al. [31].
The medical history was subsequently obtained by the PI from hospital records and included details such as the child’s age, sex, type of cancer, diagnostic approach, cancer therapy regimen, and any preceding dental care received. This ensured that the PI was blinded during the clinical assessments, thereby reducing the risk of diagnostic bias.
To ensure diagnostic consistency, one of the study supervisors (a senior paediatric dentist) conducted a calibration exercise with the PI on 10% of the sample, standardizing the diagnostic assessment of dental caries, oral mucositis, and dental plaque in one of the paediatric oncology wards. To evaluate both inter-examiner and intra-examiner reliability, Cohen’s Kappa (κ) coefficient was employed. Kappa values for dental caries, oral mucositis, and plaque were 0.82, 0.90, and 0.86, indicating substantial inter-examiner agreement. Intra-examiner reliability was also high with Kappa values of 0.90, 0.96, and 0.85 for dental caries, oral mucositis, plaque scores, demonstrating strong consistency and reproducibility of the PI’s assessments.
Statistical analysis
Data analysis was performed with IBM SPSS version 25 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized using descriptive statistics such as means, standard deviations, and medians. Relationships between variables were examined through Analysis of Variance (ANOVA), Pearson’s Chi-square test, and Spearman’s rank-order correlation. A 95% confidence interval (CI) was applied to determine the reliability and accuracy of the associations. Findings were displayed in tables to enhance and support the narrative.
Results
Study participant characteristics
One hundred and two participants completed the study, comprising 55 males (53.9%) and 47 females (46.1%). The mean age was 6.08 ± 3.1 years, ranging from three to 12 years. Leukaemia was the most frequently diagnosed malignancy, accounting for 35 cases (34.3%). The majority (59.8%, N=61) received chemotherapy alone. ALL was the most prevalent cancer subtype. Chemotherapy agents, including actinomycin-D, carboplatin, cytarabine, daunorubicin, doxorubicin, etoposide, L-asparaginase, methotrexate, and vincristine, were administered in different combinations and regimens tailored to their specific diagnoses.
Dental caries
For clinical evaluation, participants were grouped by dentition development into three to five years (primary dentition) and six to 12 years (mixed dentition or permanent dentition). Notably, only 2.9% of the participants had received a dental assessment prior to the cancer treatment. A total of 57 children (55.9%) were in the primary dentition phase (ages three to five), while 45 children (44.1%) were in the mixed or permanent dentition phase (ages six to 12).
Dental caries experience was evaluated using the dmft and DMFT indices, categorized according to the stage of dentition. Dental caries prevalence was 58.8%. Among children aged three to five years (primary dentition), the prevalence was 49.1%, whereas a notably higher rate of 71.1% was observed in those aged six to 12 years (mixed or permanent dentition). There was a statistically significant relationship between age and the occurrence of dental caries, with children aged between six and 12 years having a higher odds of dental caries compared to those the younger group (χ² = 5.020, p = 0.025). In the primary dentition group, the average dmft score was 2.33, whereas the mixed/permanent dentition group recorded a 2.78 mean DMFT score. Specifically, permanent teeth alone had a 0.33 mean DMFT score. In both dentition groups, the decayed component constituted the largest proportion of the dmft and DMFT indices, suggesting that most of the carious lesions remained untreated, particularly within the primary dentition, as shown in Table 1.
Dental caries prevalence was further assessed by cancer therapy type. Children receiving chemotherapy demonstrated a higher dental caries prevalence; however, this observation may be influenced by the fact that chemotherapy was the predominant treatment modality among study participants (Table 2).
Oral mucositis
Oral mucositis overall prevalence was 28.4%. Regarding gender, male children exhibited a slightly higher prevalence than female children. In terms of age, the younger age group (three to five years) demonstrated a higher occurrence of oral mucositis, although the difference was not statistically significant as presented in Table 3.
As detailed in Table 4, the majority of children diagnosed with OM were classified as having Grade I or Grade II severity. Specifically, 14 children (13.7%) exhibited Grade II mucositis, 13 children (12.7%) presented with Grade I, and only two children (2%) were identified with Grade III OM.
Oral hygiene status
Oral hygiene was evaluated by examining dental plaque presence and severity. All 102 participants (100%) exhibited varying levels of plaque. To measure this, the modified version of the Quigley-Hein Plaque Index by Turesky et al. was applied to assess plaque accumulation on both the buccal and lingual tooth surfaces. Based on the proportion of tooth surfaces covered by plaque, oral hygiene was classified as mild in 12 children (11.8%), moderate in 57 children (55.9%), and severe in 33 children (32.2%). Children receiving a combined a treatment of chemotherapy and surgery exhibited poorer oral hygiene.
Discussion
Children undergoing cancer treatment frequently experience adverse oral effects, with dental caries and oral mucositis among the most commonly reported conditions [32]. Although ALL comprised the largest subgroup in our cohort, other malignancies were represented; accordingly, interpretations are framed for the overall paediatric oncology population rather than a single diagnosis. At KNH, the standard ALL protocol spans two to three years across five phases (Induction, Consolidation, Interim Maintenance, Delayed Intensification, Maintenance), and most participants were assessed during induction when hospitalization for diagnostic work-up and stabilization is common [33]. Chemotherapeutic agents administered, such as actinomycin-D, carboplatin, cytarabine, daunorubicin, doxorubicin, etoposide, L-asparaginase, methotrexate, and vincristine, were consistent with risk-adapted regimens used globally [34].
Dental caries prevalence in the study was 58.8%, considerably higher than 23.9% reported in the 2015 Kenya National Oral Health Survey [35]. Similar trends were observed in Sudan, where children receiving cancer treatment exhibited a 37.9% prevalence, compared to 24% in the general paediatric population [36]. This reinforces existing evidence that children with systemic illnesses face a disproportionate burden of oral diseases, with oral healthcare being among their most frequently unmet needs [37]. Several chemotherapeutic agents are associated with reduced salivary flow and qualitative salivary alterations that may increase dental caries risk; however, sialometry was not performed in this study, references to hyposalivation are provided as literature context rather than causal inferences from our data [38]. In this cohort, limited access to paediatric dental care evidenced by only 2.9% receiving a dental evaluation during therapy was identified as a system-level risk factor for unmet preventive and therapeutic oral care.
Oral mucositis was present in 28.4% of participants, predominantly Grades I - II, lower than rates reported in prospective cohorts, such as 40% in a Brazilian paediatric cohort and 69% in Swedish children with ALL [9,39]. Differences likely reflect study design and timing in regards clinical assessment. Our cross-sectional assessment provides a point estimate at a single time point and cannot capture onset, peak severity, or fluctuations across treatment cycles. Heterogeneity in diagnoses and treatment phases, including participants assessed during rest periods, may also have allowed for mucosal healing, contributing to lower prevalence. In addition, KNH protocols which provide for prophylactic povidone-iodine mouth rinses and “magic mouthwash” containing lidocaine, chlorpheniramine, dexamethasone, and relcer gel, may mitigate mucosal inflammation, although we cannot ascribe causality [40]. Under detection of oral mucositis may be because daily monitoring was not conducted.
Oral hygiene was generally poor, with plaque observed in all children; among those with oral mucositis, 89.7% had moderate-to-severe plaque. Poor oral hygiene may be attributable to pain or interruptions in routine oral care (e.g. tooth brushing) during hospitalization both frequently reported in children with chronic illnesses [21]. These are descriptive findings from a cross-sectional snapshot and were not intended to test a plaque-oral mucositis association but they should be viewed as hypothesis-generating for future longitudinal studies.
Conclusions
In this single-centre cross-sectional study of 102 children undergoing cancer therapy at KNH, the prevalence of dental caries was 58.8% and oral mucositis 28.4% (predominantly Grades I - II), with majority having poor oral hygiene and minimal access to dental care (2.9% received a dental evaluation). The latter represents a system-level risk factor and underscores the need to integrate paediatric dental services into oncology pathways e.g., standardized pre-treatment oral screening, routine dental and oral mucositis surveillance, and timely referral, particularly in LMICs.
These findings should be interpreted in light of key limitations such as the cross-sectional design, single-centre, and clinical examinations under field conditions without adjunctive imaging (possible underestimation of early lesions). Future multi-centre, prospective studies with serial oral mucositis grading, objective salivary measures (e.g., sialometry), are recommended. Health ministries and oncology programs should mandate standardized pre-treatment oral screening and risk stratification for all paediatric cancer patients, with embedded referral pathways to paediatric dentistry and routine oral mucositis surveillance documented in the oncology record.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer of childhood in sub-Saharan Africa Ecancermedicalscience Stefan C Bray F Ferlay J Liu B Parkin DM 11201710.3332/ecancer.2017.755PMC 557466228900468 · doi ↗ · pubmed ↗
- 2Childhood cancers in a referral hospital in south-south Nigeria: a review of the spectrum and outcome of treatment Pan African Medical Journal Utuk EO Ikpeme EE 3252220152697723310.11604/pamj.2015.22.325.6990 PMC 4769810 · doi ↗ · pubmed ↗
- 3Advances in pediatric hematopoietic stem cell transplantation Cancer Biol Ther Barfield RC Kasow KA Hale GA 15331539720081892749410.4161/cbt.7.10.7046 · doi ↗ · pubmed ↗
- 4Few people actually benefit from 'breakthrough' cancer immunotherapy Gay N Prasad V 2017 https://www.statnews.com/2017/03/08/immunotherapy-cancer-breakthrough/
- 5Prevalence and capacity of cancer diagnostics and treatment: a demand and supply survey of health-care facilities in Kenya Cancer Control Wambalaba FW Son B Wambalaba AE Nyong’o D Nyong’o A 107327481988693029201910.1177/1073274819886930 PMC 689394031795739 · doi ↗ · pubmed ↗
- 6Management of oral mucositis in patients who have cancer Dent Clin North Am Lalla RV Sonis ST Peterson DE 617752200811815486510.1016/j.cden.2007.10.002PMC 2266835 · doi ↗ · pubmed ↗
- 7What do measures of ‘oral health‐related quality of life’ measure?Community Dent Oral Epidemiol Locker D Allen F 4014113520071803928110.1111/j.1600-0528.2007.00418.x · doi ↗ · pubmed ↗
- 8Chemotherapy-induced and/or radiation therapy-induced oral mucositis-complicating the treatment of cancer Neoplasia Naidu MU Ramana GV Rani PU Suman A Roy P 4234316200411554835010.1593/neo.04169 PMC 1531648 · doi ↗ · pubmed ↗