Efficacy and safety of biologics in erythrodermic psoriasis: a systematic review and single-arm meta-analysis
Lingjie Gao, Lu Shen, Hongwei Yan, Xinyang Liu, Yiran Wang, Xiaobo Li

TL;DR
This study reviews and analyzes the effectiveness and safety of biologic treatments for a severe skin condition called erythrodermic psoriasis.
Contribution
The study provides a systematic review and single-arm meta-analysis comparing the efficacy and safety of different biologic therapies for erythrodermic psoriasis.
Findings
IL-17-targeted biologics showed higher PASI 75 response rates and improved skin lesion outcomes over time.
IL-23-targeted biologics had the lowest adverse event rates, indicating better safety compared to other biologics.
Abstract
Erythrodermic psoriasis (EP) is a rare but severe inflammatory skin disease that affects the whole body. It presents clinically as widespread redness, scaling, and systemic symptoms. Treatment choices are currently limited, and conventional drugs often raise safety issues, highlighting the need for more effective and safer treatments. Biologics have emerged as a new approach. This study aimed to systematically evaluate the efficacy and safety of different biologics for EP by conducting a systematic review and single-arm meta-analysis. We performed a systematic search of four databases—Embase, PubMed, Scopus, and the Cochrane Library—for relevant clinical studies published up to May 2025. Treatment effects were evaluated by analyzing statistical data such as single-arm PASI 75 response rates and their 95% confidence intervals (CI). Heterogeneity was assessed using the I² statistic, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
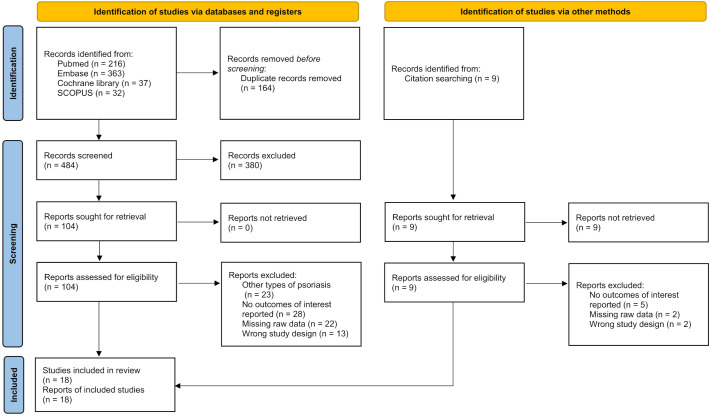 Figure 1
Figure 1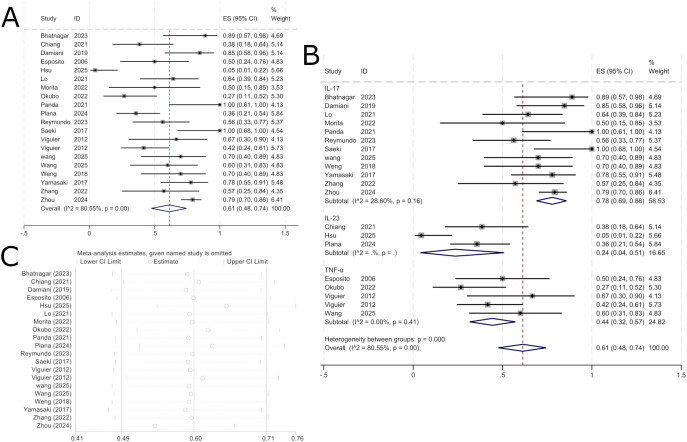 Figure 2
Figure 2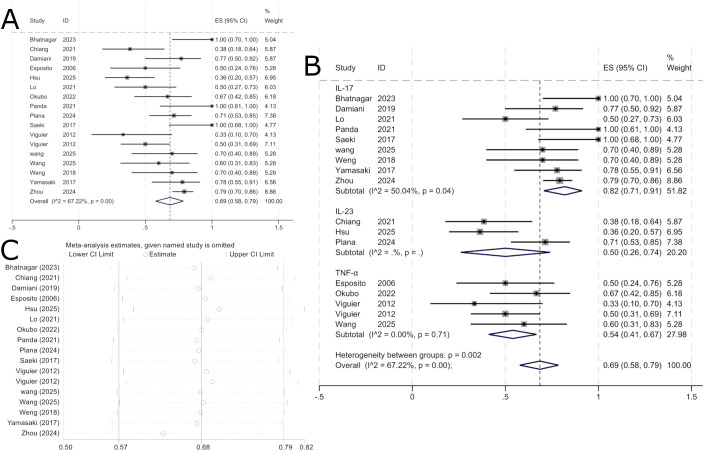 Figure 3
Figure 3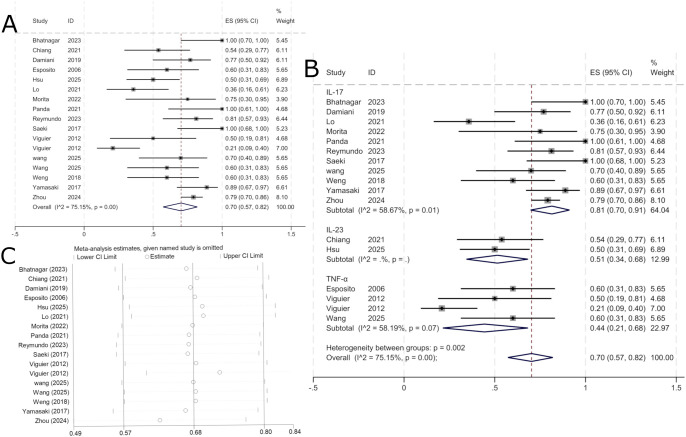 Figure 4
Figure 4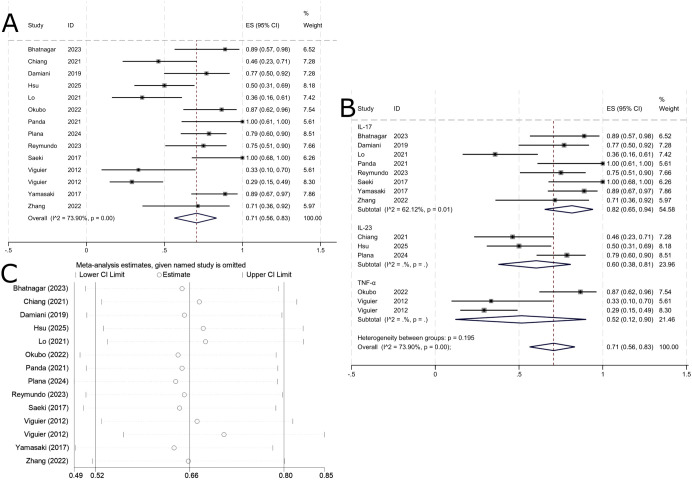 Figure 5
Figure 5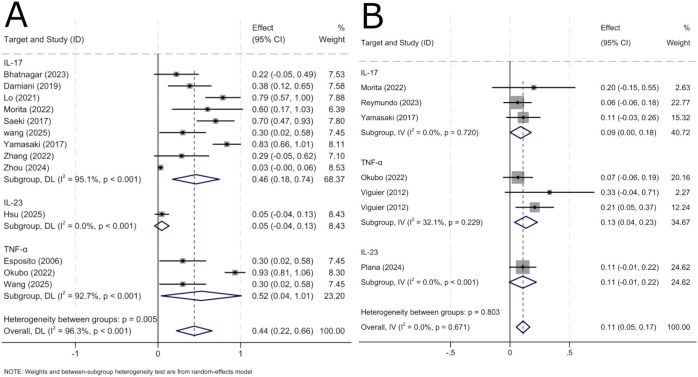 Figure 6
Figure 6| Author | Number of Participants | Male | Region | BMI | Age | Average disease duration, years | Study type | Drug | Targeted therapy | Outcome measure | Duration | Baseline PASI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bhatnagar | 9 | 7 | India | 56(14.6)1 | 15.4(10.2)1 | Prospective Study | Secukinumab | IL-17 | PASI, Body Surface Area(BSA), AE | 24W | 44.9(9.4)1 | |
| Chiang | 13 | 12 | China | 24.6(4.1)1 | 50.5(15.3)1 | 24.2 (13.3)1 | Case Series | Guselkumab | IL-23 | PASI, Drug Survival | 28W | 23.8 (8.7)1 |
| Damiani | 13 | 9 | International | 4 (22-27)2 | 40 (28-52)2 | Retrospective Study | Secukinumab | IL-17 | PASI, Dermatology Life Quality Index(DLQI), AE | 52W | 10 (7–15)3 | |
| Esposito | 10 | 8 | Italy | 56.4(11.1)1 | 1.3(1.3)1 | Prospective Study | Etanercept | TNF-α | PASI, AE | 24W | 39.8(15.2)1 | |
| Hsu | 22 | 16 | Taiwan | 28.5(4.6)1 | 49.7(12.8)1 | 23.7 (10.7)1 | Retrospective Study | Risankizumab | IL-23 | PASI, Drug Survival, AE | 100W | 20.7 (7.8)1 |
| Lo | 14 | 10 | China | 48.6(13.2)1 | 20.2 (10.4)1 | Retrospective Study | Ixekizumab | IL-17 | PASI, BSA, AE | 52W | 32.3 (12.6)1 | |
| Morita | 5 | 3 | Japan | 28.1(2.8)1 | 42.2(14.4)1 | 0.44 | Prospective Study | Ixekizumab | IL-17 | Global improvement score(GIS), Physician Global Assessment(PGA), Psoriasis Severity Index(PSSI), PASI, BSA, DLQI, AE | 20W | 41.14 |
| Okubo | 15 | 13 | Japan | 400mg:25.6(4.1)1 | 400mg:47.8(11.3)1 | 400mg:4.7 (5.3) 1 | Prospective Study | Certolizumab | TNF-α | PGA, Clinical Global Impressions scale- Improvement(CGI-I), PASI, DLQI, AE | 52W | 400mg:43.7(17.9)1 |
| Panda | 6 | 4 | India | 37.3(6.9)1 | 6.2(2.2)1 | Case Series | Secukinumab | IL-17 | PASI, DLQI, Visual Analogue Scale(VAS) | 52W | 26.0(4.0)1 | |
| Plana | 28 | 22 | Spain | 27.8 (5.7)1 | 52.6 (16.8)1 | 22.75 (13.6)1 | Retrospective Study | Ustekinumab | IL-23 | PASI, BSA, AE | 148W | 43.1 (12.3)1 |
| Reymundo | 16 | 11 | Portugal | 29.4 (4.8)1 | 54.81 (17.1)1 | 17.9 (16.4)1 | Retrospective Study | Secukinumab | IL-17 | PASI, DLQI, PGA, AE | 144W | 35.5(2.7)1 |
| Saeki | 8 | 7 | Japan | 50.2(12.9)1 | 18.4(14.0)1 | Prospective Study | Ixekizumab | IL-17 | PASI, DLQI, PGA, BSA, GIS, PSSI, Itch Numeric Rating Scale(INRS), AE | 52W | 42.8(11.6)1 | |
| Viguier | 28 | 20 | France | 25.2 (18.4-49)2 | 40 (19-73)2 | Retrospective Study | Etanercept | TNF-α | PASI, BSA, DLQI, PGA, AE | 96W | 38(20-65)2 | |
| Wang | 20 | 12 | China | 26.2(7.0)1 | 43.8(16.9)1 | 13.7(11.7)1 | Retrospective Study | Adalimumabs | TNF-α | PASI, AE | 24W | 45.4(8.8)1 |
| Weng | 10 | 8 | China | 42.6(11.0)1 | 20.6(11.4)1 | Case Series | Secukinumab | IL-17 | PASI, BSA | 24W | 32.4(5.7)1 | |
| Yamasaki | 18 | 14 | Japan | 24.3(4.9)1 | 50.8(12.2)1 | 6.37(10.1)1 | Prospective Study | Brodalumab | IL-17 | CGI-I, PASI, DLQI, PGA, BSA, AE | 52W | 36.1(13.1)1 |
| Zhang | 7 | 7 | China | 51.4(15.8)1 | 3.8(3.8)1 | Case Series | Secukinumab | IL-17 | PASI, BSA, AE | 90W | 42.2(12.1)1 | |
| Zhou | 160 | 128 | China | 24.2 (22.2,26.0)3 | 48.2(16.5) | 10.0 (0, 19.0)3 | Retrospective Study | Secukinumab | IL-17 | PASI, BSA, AE | 24W | 24.7 (15.2,38.7)3 |
| Research | Type of bias | Overall risk | ||||||
|---|---|---|---|---|---|---|---|---|
| ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | ||
| Bhatnagar 2023 ( | Moderate | Moderate | Low | Low | Low | Low | Low | Moderate |
| Damiani 2019 ( | Moderate | Moderate | Low | Low | Moderate | Low | Low | Moderate |
| Esposito 2006 ( | Severe | Moderate | Low | Low | Low | Moderate | Low | High |
| Hsu 2025 ( | Moderate | Moderate | Low | Low | Moderate | Low | Low | Moderate |
| Lo 2021 ( | High | Moderate | Low | Moderate | Moderate | Low | Low | High |
| Morita 2022 ( | Low | Moderate | Low | Low | Low | Moderate | Low | Moderate |
| Okubo 2022 ( | High | High | Low | Low | Low | Moderate | Low | High |
| Plana 2024 ( | Moderate | Moderate | Low | Moderate | Low | Low | Moderate | Moderate |
| Reymundo 2023 ( | Moderate | Low | Low | Moderate | Moderate | Low | Low | Moderate |
| Saeki 2017 ( | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Viguier 2012 ( | Severe | Moderate | Low | Moderate | Severe | Low | Low | High |
| Yamasaki | Moderate | Low | Low | Moderate | Low | Moderate | Low | Moderate |
| Wang 2025 ( | Moderate | Moderate | Low | Low | Low | Low | Low | Moderate |
| Zhou 2024 ( | Moderate | Low | Low | Low | Moderate | Moderate | Low | Moderate |
| Research | Type of bias | Overall risk | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | ⑧ | ⑨ | ⑩ | ||
| Chiang2021 ( | Yes | Yes | Yes | Yes | Yes | Yes | es | Yes | Yes | Yes | Low |
| Panda2021 ( | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | Low |
| Weng2018 ( | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | Moderate |
| Zhang2022 ( | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | Moderate |
| Result | Study | Heterogeneity | ES(95%CI) | P | P(Egger) | |
|---|---|---|---|---|---|---|
| P | I2 | |||||
| Within 12W, PASI 75(%) | 18 | 0.000 | 80.55 | 61 (95%CI:40%-73%) | 0.000 | 0.529 |
| Within 16W, PASI 75(%) | 15 | 0.002 | 67.22 | 69 (95%CI:40%-73%) | 0.000 | 0.410 |
| Within 24W, PASI 75(%) | 15 | 0.002 | 75.15 | 70 (95%CI:57%-82%) | 0.000 | 0.158 |
| Within 24W, PASI 75(%) | 13 | 0.195 | 73.9 | 71 (95%CI:56%-83%) | 0.000 | 0.396 |
| TAE(%) | 13 | 0.005 | 96.3 | 44 (95%CI:22%-66%) | 0.000 | 0.017 |
| SAE(%) | 6 | 0.803 | 0.0 | 0.11 (95%CI:4%-23%) | 0.671 | 0.050 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsoriasis: Treatment and Pathogenesis · Cutaneous lymphoproliferative disorders research · Dermatology and Skin Diseases
Introduction
1
Erythrodermic psoriasis (EP) is a rare and severe inflammatory skin disease (1). Clinical manifestations include generalized diffuse erythema affecting more than 75% of the body surface area(BSA) (2), accompanied by extensive desquamation involving nearly all exposed skin (3). Systemic symptoms like fever, lymphadenopathy, and electrolyte imbalances are common (4). In severe cases, the condition can progress to multiple organ failure, substantially increasing the risk of mortality (5). Epidemiological studies show significant geographical and demographic differences in EP prevalence, with higher rates observed in high-income regions and among elderly populations. This pattern highlights the complexity of managing the disease and the need for effective treatments.
The development of erythrodermic psoriasis can be initiated by various triggers, such as sudden withdrawal or rapid tapering of corticosteroids and other systemic therapies, drug hypersensitivity reactions, systemic infections, and psychological stress (6). Pathophysiologically, erythrodermic psoriasis is characterized by a more severe and systemic inflammatory response compared to plaque psoriasis, featuring marked vascular alterations and elevated intercellular adhesion molecule expression in affected skin (7). Central to this process is the aberrant activation of dendritic cells, which drives overactivation of the interleukin-23 (IL-23)–Th17 axis and subsequent release of effector cytokines, including tumor necrosis factor-α (TNF-α) (8). These cytokines create a complex inflammatory network that further amplifies immune responses, promoting dysregulated keratinocyte proliferation and impaired differentiation. Ultimately, this leads to widespread erythema, scaling, and compromised skin barrier function across the body, often accompanied by severe systemic complications (9).
Erythrodermic psoriasis (EP) is currently managed with a range of treatments, including topical agents, phototherapy, conventional systemic drugs, and biologics. Topical medications are appropriate for mild cases but have limited effect in moderate-to-severe disease. Conventional systemic therapies, such as methotrexate and cyclosporine, can improve lesions in moderate-to-severe patients; however, long-term use carries risks of serious adverse events, including liver and kidney toxicity—which often restrict their clinical utility and negatively impact treatment adherence and patient satisfaction (10). These limitations highlight the ongoing challenges in EP management and emphasize the urgent need for novel therapies that are both more effective and safer.
In recent years, biologics have shown important progress in the treatment of psoriasis and other autoimmune diseases. By precisely targeting and regulating abnormal immune pathways, these drugs not only improve treatment outcomes but also help overcome the safety limitations of conventional therapies. Biologics have shown favorable results across different subtypes of psoriasis. The Psoriasis Area and Severity Index (PASI) is the main measure of treatment success, and PASI 75 response—defined as at least a 75% reduction from the baseline PASI score—is widely used as a key efficacy endpoint in clinical trials (11, 12).Nevertheless, there is still a lack of comprehensive evidence from systematic reviews and single-arm meta-analyses focusing specifically on the use of biologics in the erythrodermic psoriasis (EP) subtype.
Therefore, this study systematically evaluates the efficacy and safety of various biologics—specifically IL-17, TNF-α, and IL-23 inhibitors—in patients with erythrodermic psoriasis (EP) by integrating available clinical evidence. The main goal is not only to confirm the overall role of biologics in EP treatment, but also to directly compare differences in efficacy and safety among these drug classes at key time points. The goal was to offer reliable, evidence-based guidance for clinical decision-making, with the ultimate aim of improving treatment outcomes and patient quality of life.
Method
2
Literature search
2.1
On May 26, 2025, the authors searched four electronic databases—PubMed, Scopus, Embase, and the Cochrane Library—using a combination of keywords related to erythrodermic psoriasis, biologics, and clinical trials. PubMed was used as an example, and retrieval formula is provided in Supplementary Table 1. A manual search of relevant sources was also performed. The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (13), and was registered in PROSPERO (CRD420251129658).
Inclusion and exclusion criteria
2.2
Inclusion Criteria: (1) Patients clinically diagnosed with erythrodermic psoriasis; (2) Patients receiving initial therapy with biologics or who have previously received biologic therapy; (3) Reporting of efficacy evaluation indicators such as the Psoriasis Area and Severity Index (PASI) or adverse events for erythrodermic psoriasis. Exclusion Criteria: (1) Literature classified as reviews or commentaries; (2) Duplicate publications or updated literature; (3) Literature where full text was unavailable or data were incomplete.
Efficacy evaluation indicators
2.3
Clinical efficacy was assessed using the Psoriasis Area and Severity Index (PASI) 75 response as the primary outcome measure, reported as the proportion of patients who achieved a PASI 75 improvement.
Data extraction and risk of bias assessment
2.4
The following characteristics were extracted from the included studies: author, region, ethnicity, sample size, age, sex, treatment regimen, and outcome measures. Study quality was evaluated using the ROBINS-I tool (14) and the JBI Critical Appraisal Tool for Case Series (15). Any disagreements between researchers were resolved through discussion. Unresolved issues were referred to a relevant expert, with third-party arbitration used if consensus could not be reached.
Statistical analysis
2.5
Treatment efficacy was analyzed using single-arm proportion rates with 95% confidence intervals (CI). Heterogeneity was evaluated with the I² statistic, and subgroup analyses were performed by drug target and treatment duration. A fixed-effect model was used when I² ≤ 50% and p ≥ 0.1; otherwise, a random-effects model was applied. All tests were two-sided, with statistical significance set at p < 0.05. Publication bias was assessed using Egger’s test, where p > 0.05 suggested no significant bias. Sensitivity analysis was conducted to examine the robustness of the pooled results. All analyses were carried out using Stata 18.0 software.
Result
3
Study characteristics
3.1
Of the 648 studies identified, 18 met the inclusion criteria (16–33) (Figure 1), involving a total of 342 patients. Among them, 194 were treated with IL-17-targeted biologics (secukinumab, ixekizumab,Brodalumab), 63 received TNF-α-targeted biologics (etanercept, infliximab, adalimumab, certolizumab), and 63 were administered IL-23-targeted biologics (guselkumab, ustekinumab, risankizumab). Baseline data and key characteristics of the included studies are summarized in Table 1. (see Table 1 for details).
Study flow diagram.
Risk of bias assessment
3.2
The ROBINS-I tool is designed for use with non-randomized studies that evaluate intervention effects. It is mainly used to assess the methodological quality of case reports and case series, and is commonly applied in systematic reviews to evaluate risk of bias in observational studies (see Table 2, Table 3).
PASI
3.3
PASI 75 response rate at 12 weeks
3.3.1
A total of 18 publications, comprising 20 study groups, provided outcome data at 12 weeks for 342 patients, among whom 210 achieved a PASI 75 response. The pooled analysis showed that the overall PASI 75 response rate for biologic therapy in erythrodermic psoriasis at 12 weeks was 61% (95% CI: 40%–73%; Figure 2A). The specific drugs and number of studies in each subgroup are as follows: IL-17 inhibitors include secukinumab (n=8), ixekizumab (n=3), and brodalumab (n=1); IL-23 inhibitors include ustekinumab (n=1), risankizumab (n=1), and guselkumab (n=1); TNF-α inhibitors included etanercept (n=2), certolizumab (n=1), adalimumab (n=1), and infliximab (n=1).
Pooled analysis of response rate for PASI 75 within 12 weeks. (A) Forest plot of PASI 75 response rate within 12 weeks. (B) Forest Plot of PASI 75 Response Rate Subgroup Analysis Within 12 Weeks. (C) Forest Plot of PASI 75 Response Rate Subgroup Analysis Within 12 Weeks.
In subgroup analysis by biologic target, the PASI 75 response rate was 78% (95% CI: 69%–86%) for IL-17-targeted biologics, 44% (95% CI: 32%–57%) for TNF-α-targeted biologics, and 24% (95% CI: 4%–51%) for IL-23-targeted biologics. As shown in Figure 2B, IL-17-targeted biologics were the most effective in achieving PASI 75 improvement over 12 weeks, followed by TNF-α-targeted biologics, while IL-23-targeted biologics showed the lowest response. Due to substantial heterogeneity (I² = 80.55%), a random-effects model was used. Sensitivity analysis indicated that the results were robust and stable across studies (Figure 2C).
PASI 75 response rate at 16 weeks
3.3.2
A total of 15 publications encompassing 17 study groups provided comparative outcome data at 16 weeks, involving 315 patients, of whom 216 achieved a PASI 75 response rate. Pooled analysis indicated that the PASI 75 response rate for biologic therapy in erythrodermic psoriasis within 16 weeks was 69% (95% CI: 40%-73%), as shown in Figure 3A.Subgroup analyses were conducted for different targeted biologics used, with specific drugs and study numbers in each subgroup as follows: IL-17 inhibitors included secukinumab (n=6), ixekizumab (n=2), and brodalumab (n=1); IL-23 inhibitors included ustekinumab (n=1), risankizumab (n=1), and guselkumab (n=1); TNF-α inhibitors included etanercept (n=2), certolizumab (n=1), adalimumab (n=1), and infliximab (n=1).
Pooled analysis of response rate for PASI 75 within 16 weeks. (A) Forest plot of PASI 75 response rate within 16 weeks. (B) Forest Plot of PASI 75 Response Rate Subgroup Analysis Within 16 Weeks. (C) Forest Plot of PASI 75 Response Rate Subgroup Analysis Within 16 Weeks.
Results showed that the PASI 75 response rate was 82% (95% CI: 71%-91%) among patients receiving IL-17-targeted biologics, while the PASI 75 response rate for IL-23-targeted biologics was 50% (95% CI: 26%-74%), and for TNF-α-targeted biologics it was 54% (95% CI: 41%-67%). As shown in Figure 3B, this indicates that over 16 weeks, IL-17-targeted biologics demonstrated the most effective PASI 75 improvement in treating erythrodermic psoriasis, followed by TNF-α-targeted biologics, while IL-23-targeted biologics showed the poorest efficacy. Since I² = 67.22% > 50%, a random-effects model was selected for analysis. Sensitivity analysis was conducted to examine sources of heterogeneity, revealing good stability in the results, as shown in Figure 3C.
PASI 75 response rate at 24 weeks
3.3.3
A total of 15 publications, comprising 17 study groups, reported outcome data at 24 weeks for 291 patients, of whom 203 achieved a PASI 75 response. The pooled analysis indicated a PASI 75 response rate of 70% (95% CI: 57%–82%) for biologic therapy in erythrodermic psoriasis at 24 weeks (Figure 4A). The specific drugs and number of studies in each subgroup are as follows: IL-17 inhibitors include secukinumab (n=7), ixekizumab (n=4), and brodalumab (n=1); IL-23 inhibitors include risankizumab (n=1) and guselkumab (n=1); TNF-α inhibitors included etanercept (n=2), adalimumab (n=1), and infliximab (n=1).
Pooled analysis of response rate for PASI 75 within 24 weeks. (A) Forest plot of PASI 75 response rate within 24 weeks. (B) Forest Plot of PASI 75 Response Rate Subgroup Analysis Within 24 Weeks. (C) Forest Plot of PASI 75 Response Rate Subgroup Analysis Within 24 Weeks.
Subgroup analysis by biologic target showed PASI 75 response rates of 81% (95% CI: 70%–91%) for IL-17-targeted biologics, 51% (95% CI: 34%–68%) for IL-23-targeted biologics, and 44% (95% CI: 21%–68%) for TNF-α-targeted biologics. As shown in Figure 4B, IL-17-targeted biologics demonstrated the highest efficacy over 24 weeks, followed by IL-23-targeted biologics, while TNF-α-targeted biologics showed the lowest response. Given the substantial heterogeneity (I² = 75.15%), a random-effects model was used. Sensitivity analysis confirmed the stability of the results (Figure 4C).
PASI 75 response rate after 24 weeks
3.3.4
This analysis pooled data from studies with extended follow-up (28–148 weeks) to assess the medium- and long-term efficacy of biologics (Table 1).The study comprised 13 literature sources, comprising 14 study groups, provided outcome data at 24 weeks for 197 patients, among whom 139 achieved a PASI 75 response. The pooled PASI 75 response rate for biologic therapy in erythrodermic psoriasis at 24 weeks was 71% (95% CI: 56%–83%; Figure 5A). The specific drugs and number of studies in each subgroup are as follows: IL-17 inhibitors include secukinumab (n=5), ixekizumab (n=2), and brodalumab (n=1); IL-23 inhibitors include ustekinumab (n=1), risankizumab (n=1), and guselkumab (n=1); TNF-α inhibitors included etanercept (n=1), certolizumab (n=1), and infliximab (n=1).
Pooled analysis of response rate for PASI 75 after 24 weeks. (A) Forest plot of PASI 75 response rate after 24 weeks. (B) Forest Plot of PASI 75 Response Rate Subgroup Analysis after 24 Weeks. (C) Forest Plot of PASI 75 Response Rate Subgroup Analysis after 24 Weeks.
Subgroup analysis by biologic target showed PASI 75 response rates of 82% (95% CI: 65%–94%) for IL-17-targeted biologics, 60% (95% CI: 38%–81%) for IL-23-targeted biologics, and 52% (95% CI: 12%–90%) for TNF-α-targeted biologics. As illustrated in Figure 5B, IL-17-targeted biologics demonstrated the highest efficacy after 24 weeks, followed by IL-23-targeted biologics, while TNF-α-targeted biologics showed the lowest response. Due to substantial heterogeneity (I² = 73.90%), a random-effects model was used. Sensitivity analysis indicated stable results across the included studies (Figure 5C).
Adverse events
3.3.5
The safety analysis included 12 publications (13 study groups) reporting adverse events in erythrodermic psoriasis patients treated with biologics. The overall incidence of adverse events was 44% (95% CI: 22%–66%). Subgroup analysis by drug class showed incidence rates of 46% (95% CI: 18%–74%) for IL-17-targeted biologics, 5% (95% CI: –4%–13%) for IL-23-targeted biologics, and 52% (95% CI: 4%–101%) for TNF-α-targeted biologics (Figure 6A). Severe adverse events occurred in 11% (95% CI: 5%–17%) of patients (Figure 6B). Commonly reported adverse events included infections, injection site reactions, infusion-related reactions, and diarrhea. Candida infections and injection site reactions were more frequent with IL-7 inhibitors, whereas infusion reactions and serious infections were more commonly associated with TNF-α inhibitors.
Pooled analysis of adverse event. (A) Forest Plot of Overall Adverse Event Incidence by Subgroup Analysis. (B) Forest Plot of Subgroup Analysis for Serious Adverse Event Incidence.
Publication bias analysis
3.4
Publication bias was assessed using Egger’s test for the included studies. No significant publication bias was observed for PASI 75 at 12 weeks (p = 0.529), 16 weeks (p = 0.410), 24 weeks (p = 0.158), 24 weeks or longer (p = 0.396), or the incidence of serious adverse events (p = 0.050), as all p-values were ≥ 0.05 (Supplementary Figures 1-5). In contrast, significant publication bias was detected for the overall adverse event rate (p = 0.017), as shown in Supplementary Figures 6.
All the results mentioned above are summarized in Table 4.
Discussion
4
This study evaluated the efficacy and safety of biologics in erythrodermic psoriasis (EP) by means of a systematic review and single-arm meta-analysis. EP is a severe, potentially life-threatening systemic inflammatory skin disease. Its pathogenesis involves abnormal activation of multiple inflammatory pathways and complex cytokine regulation. Current evidence indicates that EP is mainly driven by widespread Th1 and Th17 immune activation, with key roles played by cytokines such as TNF-α, IL-17, and IL-23 in disease initiation and progression (1, 34). Specifically, TNF-α acts as an important early mediator in EP inflammation and further promotes the release of IL-17 and IL-23, creating a positive feedback loop that amplifies systemic inflammation (35). IL-17, a proinflammatory cytokine produced by Th17 cells and type 3 innate lymphoid cells (ILC3), is a central player in EP pathogenesis. It promotes neutrophil activation and infiltration, thereby intensifying the inflammatory response (36, 37). IL-23 is highly expressed in EP lesions and works together with TNF-α to stimulate the proliferation and activation of Th17 cells (38, 39). This leads to increased production of IL-17A and IL-17F, resulting in excessive cell proliferation and abnormal differentiation (40), which together contribute to disease progression.
This study found that biologics targeting different pathways are all effective in treating erythrodermic psoriasis. During the 12-week treatment period, the proportion of patients achieving a PASI 75 response increased gradually over time. Subgroup analysis by target showed that IL-17-targeted biologics performed particularly well in improving skin lesion severity, with the highest response rates observed at 16 and 24 weeks, indicating superior skin clearance. Previous studies have reported complete skin clearance in EP patients following treatment with IL-17-targeted biologics (41), supporting the central role of IL-17 as a key cytokine and aligning with the present findings.
The enrolled patient population demonstrated considerable heterogeneity in baseline characteristics. Patients receiving IL-17 inhibitors tended to present with more severe disease at baseline, which further underscores the notable efficacy observed with this drug class. Variations in prior biologic exposure were also evident across treatment groups, with the IL-23 inhibitor subgroup including a higher proportion of patients with refractory disease, potentially contributing to the lower early response rates observed. Furthermore, differences in demographic factors such as age and ethnicity, as well as comorbidities like metabolic syndrome and prior infections, may have indirectly influenced outcomes by altering drug metabolism or immune response. These baseline imbalances, likely reflecting real-world clinical selection, suggest that the efficacy and safety profiles identified in this analysis are contextual and should be interpreted with these factors in mind. These findings highlight the importance of stratified study designs in future research and individualized treatment selection based on specific patient characteristics.
In terms of treatment trajectory, TNF-α inhibitors showed a better response than IL-23 inhibitors at weeks 12 and 16. With longer treatment duration, however, IL-23 inhibitors gradually overtook TNF-α inhibitors in efficacy by week 24 and beyond. This pattern may be explained by the characteristically slower onset of action of IL-23-targeted therapy. Previous studies have shown that the superior efficacy of anti-IL-23 agents in plaque psoriasis often becomes fully apparent over extended treatment periods, such as 24 to 52 weeks (42). Consistent with this profile, the present analysis also indicated a clear increase in response rates for IL-23 inhibitors at and beyond week 24.
This study also noted a decrease or fluctuation in the PASI 75 response rate for anti-TNF-α agents by week 24 and beyond compared to earlier time points. Several factors may explain this observation. First, the systemic hyperinflammation seen in erythrodermic psoriasis may promote the development of anti-drug antibodies, which can reduce drug activity or accelerate clearance, thereby impairing treatment efficacy (43). Second, in some cases, TNF-α inhibitors may trigger or worsen other immune-mediated inflammatory conditions, such as new or aggravated psoriasiform skin lesions or arthritis (44). Such events could be recorded as reduced treatment response in clinical evaluations. In addition, the analyzed population may have included patients with refractory disease who did not respond adequately to prior conventional or biologic therapies, and who may thus show limited response to TNF-α inhibition. Therefore, the apparent decline in late-stage efficacy of anti-TNF-α agents likely reflects the complexity of treating this severe and often refractory EP population, rather than an inherent lack of efficacy.
Erythrodermic psoriasis (EP) presents clinically as widespread redness, swelling, and scaling that can affect the entire or nearly entire skin surface. It is often accompanied by severe itching, pain, and systemic symptoms (41). Studies suggest that EP may lead to serious complications such as heart failure and sepsis, which can be life-threatening in severe cases (4)Compared to other subtypes of psoriasis, patients with EP have a higher risk of mortality, making early disease control and the choice of effective treatment crucial. This study shows that IL-17-targeted biologics are highly effective in EP. A PASI 75 response rate of 78% (95% CI: 69%–86%) was achieved within 12 weeks of treatment, which was significantly higher than that of TNF-α and IL-23-targeted biologics. These results highlight the important role of IL-17-targeted biologics in the management of EP and support their use as a first-line treatment option for rapid and effective disease control.
Additionally, this study systematically evaluated treatment safety and found an overall adverse event incidence of 42% (95% CI: 21%–67%). Subgroup analysis by drug class showed distinct safety profiles: TNF-α inhibitors had the highest overall adverse event rate at 52% (95% CI: 4%–101%), followed by IL-17 inhibitors at 46% (95% CI: 18%–74%), while IL-23 inhibitors demonstrated the lowest rate of 5% (95% CI: –4%–13%). Although based on limited data, this finding is consistent with the favorable tolerability of IL-23 inhibitors observed in plaque psoriasis (45). The high target specificity of IL-23 inhibitors may contribute to this safety advantage by minimizing broad effects on immune function. For serious adverse events, incidence was 13% (95% CI: 4%–23%) with TNF-α inhibitors, 11% (95% CI: –1%–22%) with IL-23 inhibitors and 9% (95% CI: 0%–18%) with IL-17 inhibitors.
Despite differences in overall adverse event rates, the risk of serious adverse events remained relatively comparable across biologic classes and within an acceptably low range. These results suggest that biologics have an acceptable safety profile in EP treatment, with TNF-α-targeted agents exhibiting the most favorable safety. This information supports the selection of individualized treatment strategies in clinical practice.
This study has several limitations. First, the number of included studies was relatively small (n = 18), and most were observational rather than randomized controlled trials. This may reduce the precision of the pooled estimates and affect the reliability of subgroup analyses. Additionally, due to incomplete information on patients’ prior treatment history in the original study, we were unable to conduct a systematic stratified analysis between treatment-naive and treatment-experienced patients receiving biologics. This limitation may also influence the interpretation of efficacy and safety outcomes. Second, there were inconsistencies across studies in how efficacy endpoints such as PASI 75 and adverse events were defined, assessed, and reported. In particular, the documentation of mild to moderate adverse events varied considerably, which may have introduced heterogeneity, especially in the overall adverse event rate. In addition, follow-up duration differed among the included studies, limiting the assessment of long-term outcomes such as efficacy maintenance beyond 24 weeks, drug resistance, and delayed safety risks. Finally, some findings—such as the fluctuating efficacy of anti–TNF-α agents—differ from those typically reported in plaque psoriasis trials. This does not diminish the validity of our results but rather highlights that erythrodermic psoriasis, as a distinct and severe inflammatory condition, may lead to different biologic response patterns, influenced by factors such as high inflammatory burden, patient selection bias, and concomitant medications.
Conclusions
5
This meta-analysis indicates that biologics have favorable efficacy and safety in the treatment of erythrodermic psoriasis (EP), supporting their use in clinical practice. Comprehensive analysis shows that IL-17-targeted biologics produce a faster and stronger clinical response compared to other biologic types, while IL-23-targeted biologics demonstrate better safety. Based on current evidence, future large-scale studies with long-term follow-up are needed to further evaluate the efficacy and safety of different biologics in specific patient groups and to assess their role in long-term relapse prevention. Such research will help develop more individualized treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rendon A Schakel K . Psoriasis pathogenesis and treatment. Int J Mol Sci. (2019) 20:1475. doi: 10.3390/ijms 20061475, PMID: 30909615 PMC 6471628 · doi ↗ · pubmed ↗
- 2Eddy DE Harman D . Free radical theory of aging: effect of age, sex and dietary precursors on rat-brain docosahexanoic acid. J Am Geriatr Soc. (1977) 25:220–9. doi: 10.1111/j.1532-5415.1977.tb 00303.x, PMID: 856907 · doi ↗ · pubmed ↗
- 3Yamada M Kubo H Kobayashi S Ishizawa K He M Suzuki T . The increase in surface CXCR 4 expression on lung extravascular neutrophils and its effects on neutrophils during endotoxin-induced lung injury. Cell Mol Immunol. (2011) 8:305–14. doi: 10.1038/cmi.2011.8, PMID: 21460863 PMC 4002449 · doi ↗ · pubmed ↗
- 4Rosenbach M Hsu S Korman NJ Lebwohl MG Young M Bebo BF Jr. . Treatment of erythrodermic psoriasis: from the medical board of the National Psoriasis Foundation. J Am Acad Dermatol. (2010) 62:655–62. doi: 10.1016/j.jaad.2009.05.048, PMID: 19665821 · doi ↗ · pubmed ↗
- 5Lo Y Tsai TF . Updates on the treatment of erythrodermic psoriasis. Psoriasis (Auckl). (2021) 11:59–73. doi: 10.2147/PTT.S 288345, PMID: 34136373 PMC 8200157 · doi ↗ · pubmed ↗
- 6Oda T Sawada Y Yamaguchi T Ohmori S Omoto D Haruyama S . Psoriatic erythroderma caused by terbinafine: A possible pathogenetic role for IL-23. J Investig Allergol Clin Immunol. (2017) 27:63–4. doi: 10.18176/jiaci.0116, PMID: 28211348 · doi ↗ · pubmed ↗
- 7Bressan AL Picciani BLS Azulay-Abulafia L Fausto-Silva AK Almeida PN Cunha KSG . Evaluation of ICAM-1 expression and vascular changes in the skin of patients with plaque, pustular, and erythrodermic psoriasis. Int J Dermatol. (2018) 57:209–16. doi: 10.1111/ijd.13883, PMID: 29318579 · doi ↗ · pubmed ↗
- 8Moy AP Murali M Kroshinsky D Duncan LM Nazarian RM . Immunologic overlap of helper T-cell subtypes 17 and 22 in erythrodermic psoriasis and atopic dermatitis. JAMA Dermatol. (2015) 151:753–60. doi: 10.1001/jamadermatol.2015.2, PMID: 25760640 · doi ↗ · pubmed ↗