The accuracy of preoperative ultrasound use in primary flexor tendon repair: A systematic review
Faderani Ryan, Seraj Shaikh Sanjid, Shahrjerdi Puneh, Kungwengwe Garikai, Kanapathy Muholan, Nikkhah Dariush, Mosahebi Afshin

TL;DR
This review assesses how accurate ultrasound is in diagnosing flexor tendon injuries before surgery, finding it effective for complete tears but less so for partial ones.
Contribution
The study systematically evaluates the diagnostic accuracy of preoperative ultrasound for flexor tendon injuries in clinical settings.
Findings
Ultrasound has high sensitivity and specificity for complete flexor tendon tears.
Ultrasound is less accurate for partial tears, with low sensitivity.
Ultrasound aids in surgical planning, reducing exploratory surgery and operative time.
Abstract
Flexor tendon injuries disrupt hand function and require precise surgical repair. Traditionally assessed through physical examination alone, ultrasound scanning (USS) is emerging as a valuable tool, offering real-time, non-invasive imaging to assess injury type and extent. This review evaluates the USS's accuracy in preoperative flexor tendon assessment. Following PRISMA guidelines, a systematic review was conducted using MEDLINE, EMBASE, and Web of Science. Studies on primary flexor tendon injuries assessed with preoperative USS were included, while non-clinical studies, animal models, and incomplete datasets were excluded. Two reviewers screened articles, with disagreements resolved by a third reviewer. From 1354 initial studies, nine met inclusion criteria, comprising one RCT, four prospective, and four retrospective studies. In total, 450 patients (593 tendons) with diverse…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
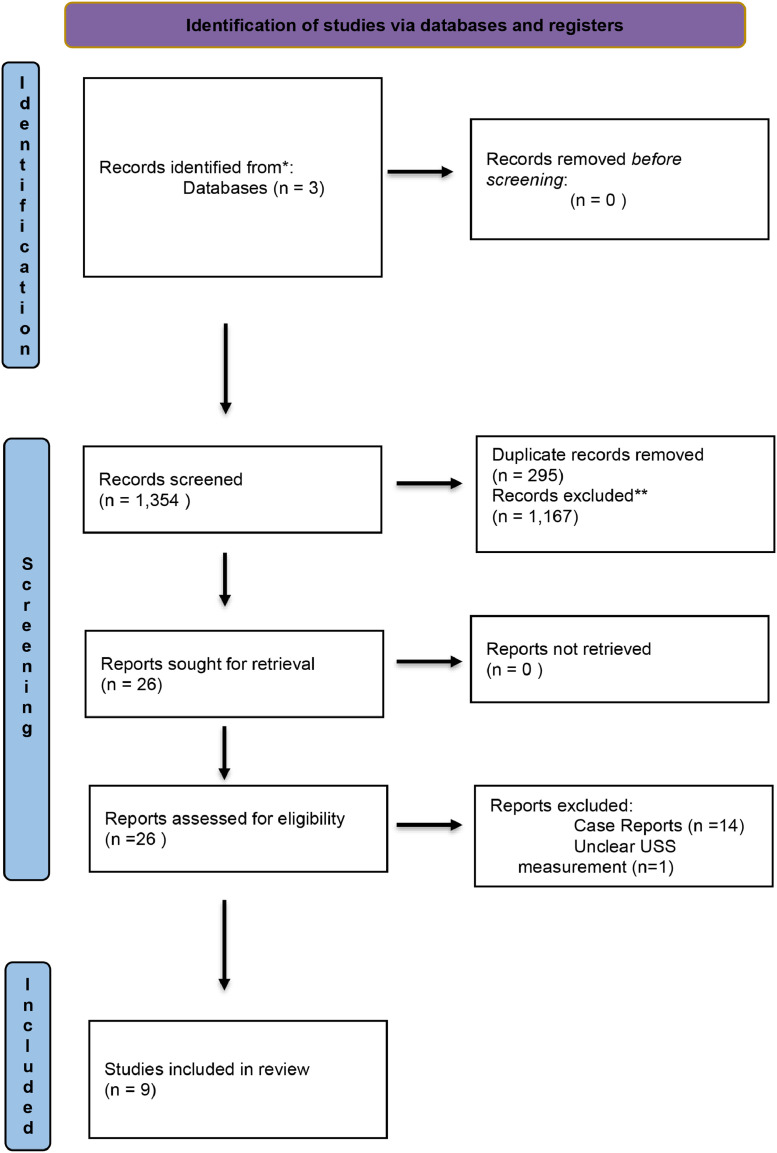 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Tendon Structure and Treatment · Elbow and Forearm Trauma Treatment
Introduction
Flexor tendon injuries, if left untreated, can lead to significant hand deformity and disability, often necessitating surgical repair to restore hand function.1 Such injuries, commonly caused by lacerations, occupational or sports accidents, disrupt tendon anatomy and function, requiring preoperative assessments to guide both operative and non-operative management.2
Physical examination has been the traditional gold standard for pre-operative assessment of flexor tendon injuries. Increasingly, ultrasound scanning (USS) has emerged as an adjunct to physical examination of flexor tendon injuries, offering real-time, high-resolution images.3 USS is non-invasive, inexpensive, widely available, and radiation-free. Studies have shown various applications of USS regarding flexor tendon repairs. For example, USS has been utilized to evaluate flexor tendon integrity and distinguish between partial and complete tears.4, 5, 6 The ability of USS to visualize soft tissue structures, measure tendon retraction, and assess surrounding anatomical features makes it a valuable tool in the preoperative planning for flexor tendon repairs.7, 8, 9
This review seeks to determine the overall utility of USS in preoperative assessment for flexor tendon repairs. Preoperative evaluation with USS could lead to better surgical outcomes, reduced operative times, minimized complications, and improved patient-reported outcomes and satisfaction. A review of the literature suggests that no prior systematic reviews have addressed the use of preoperative ultrasound in the surgical repair of flexor tendon injuries.
Aims
How accurate is USS of flexor tendons in identifying primary flexor tendon injuries in the pre-operative phase?
Methods
This systematic review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines.10
Search strategies
A systematic review of the literature was performed using the MEDLINE (OvidSP), EMBASE (OvidSP) and WoS (Web of Science) databases. The search strategy included a combination of text words and Medical Subject Headings (MeSH) terms. The following search strategy was tailored across the three databases to ensure optimal search results:
((TS=(Flexor tendon* OR flexor digitorum superficialis adj5 tendon* OR FDS adj5 tendon* OR flexor digitorum profundus adj5 tendon* OR FDP adj5 tendon* OR flexor policis longus adj5 tendon* OR FPL adj5 tendon* OR Flexor zone*)) AND TS=(injur* OR ruptur* OR lacerat* OR sever* OR avuls* OR tear*)) AND TS=(Repair* OR Reconstruct* OR surg*)) AND TS=(finger* OR hand* OR hand injur* OR finger injur*)) AND TS=(ultrasound* OR ultrasonography* OR sonograph* OR echograph).
No language or publication restrictions were applied.
Inclusion criteria
All primary clinical studies involving use of pre-operative ultrasound imaging in primary flexor tendon sheath repairs involving all patients were included.
Exclusion criteria
The exclusion criteria were studies that reported no clinical data pertaining to ultrasound imaging in flexor tendon sheath repairs, post-operative ultrasound imaging, non-English language articles, in vitro studies, all review articles and studies in animal or cadaveric models. Abstracts, conference proceedings without full text, and ongoing trials with incomplete data sets were excluded.
Outcome measures
The primary outcome measures were number of tendon assessed by USS, USS device, mechanism of injury, number of complete and partial injuries confirmed by USS.
Study selection and data management
Study selection was conducted in a two-stage process. Two reviewers initially screened titles and abstracts for potential eligibility after excluding duplicate studies. Next, studies identified as relevant underwent full-text review by both reviewers. Discussion and referral to a third reviewer were used to resolve conflicts between the reviewers in the study selection. The data from all full-text articles accepted for final analysis were independently retrieved using a standardized data extraction form. Any discrepancies between reviewers at this point were resolved through discussion or referral to senior author. The search results were recorded including abstracts, full-text articles, and records of reviewers’ decisions, including reasons for exclusion.
The extracted data includes details on study characteristics, patient demography, the type of ultrasound used, details regarding the flexor tendon injury, and patient-reported outcome measures. Data was extracted from the studies as presented or calculated.
Results
Search results
An initial 1354 studies were found from the initial searches. Initial searches were conducted on MEDLINE (OvidSP), EMBASE (OvidSP) and WoS (Web of Science) databases. 295 duplicate papers were identified and removed. The screening process and conclusion of finalized articles are illustrated in the PRISMA diagram (Figure 1). 26 papers were then examined for eligibility and full-paper review. Following a full-paper review, 17 publications were excluded. These excluded studies were either case reports or did not differentiate the time of USS. Following exclusion, nine articles were included for final analysis.Figure 1PRISMA diagram.Figure 1
Study characteristics
There was one randomized control trial, four prospective cohort studies, and four retrospective case-control studies. All studies used USS in the preoperative phase.
Study demographics
Across the nine papers, 593 flexor tendons were identified in 450 patients: men (n = 296) and women (n = 154). Traumatic flexor tendon injuries resulted from street fights, workplace injuries, gunshots, saw blades, knives, tin cans, band saws, barbecue grills or self-inflicted wounds (Table 1, Table 2, Table 3, Table 4).Table 1. Summary of included studies.Table 1. StudyMechanism/Injury typeNo. of tendons (n =)Type of USSComplete tears (n =)Incomplete tears (n =)No tear (n =)Wang et al., 199937Trauma (unspecified)8AT: HD1–3000 5–9 MHz hockey stick linear probe3Not recorded5Lee et al., 20006Gunshot, saw blade, knife, tin can, band saw, barbecue grill18Advanced technology laboratories ultramark 9 ultrasound scanner (Bothell, WA), with a 38-mm L10–5 MHz linear transducer6112Jeyapalan et al., 20089Trauma (unspecified)13Siemens Antares (Siemens AG, Erlangen, Germany) ATL HDI 5000 (ATL ultrasound, Philips medical systems company, Bothell, USA).102Zhang et al., 20128Work accidents, self-inflicted185LOGIQ 9, GE Healthcare, 10 MHz79160Al-Hourani et al., 201838Trauma (unspecified)9Philips 15 MHz iU22 diagnostic US system with L15–7IO transducer8Not recorded1Akhavan et al., 201939Street fight: 61.6 %, work: 25 %, home: 13.4 %214Bedside “point-of-care” USS 12 MHz SonositeTM surface probe.48 (inc incomplete)48 (includes complete)165Bekhet et al., 20215Injured site: first digit (17.5 % n = 7), second digit (20.0 % n = 8), third digit (15.0 % n = 6), fourth digit (15.0 % n = 6), fifth digit (15.0 % n = 6), wrist (7.5 % n = 3), palm (10.0 % n = 4). Injured zone: I (10.0 % n = 4), II (47.5 % n = 19), III (12.5 % n = 13), IV (5.0 % n = 2)50LOGIQ P9 ultrasound system from GE Healthcare, Chicago, IL,USA) with Doppler2195Meisami et al., 202140Trauma (unspecified)80Toshiba device52253Bezirgan et al., 202341Zone 1 (n = 6), Zone 2 (n = 14), Zone 5 (n = 1)21Not RecordedNot recordedNot recordedNot recordedTable 2Summary of tendon injuries.Table 2. StudyNo. of tendonsInjured tendonsFlexor zone of injuryOpen/ClosedWang et al., 199937209/20 FDP 7/20 FDS 4/20 FPLNot specified19/20 Open 1/20 Closed (#)Lee et al., 20006178/17 FDP 7/17 FDP + FDS 2/17 FPL3/17 Zone 1 6/17 Zone 2 1/17 Zone 3 10/17 investigated post tendon repair3/17 Closed 14/17 OpenJeyapalan et al., 20089185185 FDP + FDS100 % Zone 2Not specifiedZhang et al., 2012893 FDP + FDS 1 FDS + A2/A3 pulley 2 FDP 2 FPLNot specifiedNot specifiedAl-Hourani et al., 201838214Not specifiedNot specified214 Open (penetrating injury)Akhavan et al., 2019395014/50 FDS 26/50 FDP 1/50 FCU 7/50 FPL 1/50 FCR 1/50 PL4/40 Zone I 19/40 Zone II 5/40 Zone III 2/40 Zone IV 2/40 Zone V 1/40 T1 6/40 T2 1/40 T322/35 Open 13/35 ClosedBekhet et al., 20215801.8 % FCR + FCU 13.3 % FDP 21.2 % FDSNot specified80 Open (penetrating hand trauma)Meisami et al., 20214021Not specified6/21 Zone 1 14/21 Zone 2 1/21 Zone 5Not specifiedBezirgan et al., 202341209/20 FDP 7/20 FDS 4/20 FPLNot specified19/20 Open 1/20 Closed (#)FPL, Flexor pollicis longus; FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis; FCR, flexor carpii radialis; FCU, flexor carpii ulnaris; A pulley, annular pulley.Table 3. Summary of accuracy USS results (complete tears).Table 3. StudySensitivity (%) ± (CI)Specificity (%) ± (CI)PPV (%)NPV (%)LR+LR-Diagnostic Odds Ratio (DOR)Wang et al., 199937100 (100, 100)100 (100, 100)100100N/AN/AN/ALee et al., 2000687.5 (61, 100)91.7 (69.6, 100)87.591.6710.50.136377.035Jeyapalan et al., 20089100 (100, 100)100 (100, 100)100100N/AN/AN/AZhang et al., 20128100 (100, 100)100 (100, 100)100100N/AN/AN/AAl-Hourani et al., 20183875 (45, 100)99.8 (96.7, 100)99.991301.3750.2511200.7Akhavan et al., 201939100 (100, 100)99.4 (97.2, 100)97.99100166.6670N/ABekhet et al., 20215100 (100, 100)100 (100, 100)100100N/AN/AN/AMeisami et al., 20214086.5 (77.2, 95.8)72.2 (60, 84.4)81.878.93.120.18716.684Bezirgan et al., 20234150 (28.6, 71.4)67 (46.9, 87.1)86251.5150.74632.03CI, Confidence interval; PPV, positive predictive value; NPV, negative predictive value; LR+, positive likelihood ratio; LR-, negative likelihood ratio.Table 4. Summary of accuracy USS results (incomplete tears).Table 4. StudySensitivity (%) ± (CI)Specificity (%) ± (CI)PPV (%)NPV (%)LR+LR-Diagnostic Odds Ratio (DOR)Wang et al., 199937No documentation on partial tearsLee et al., 20006000000N/AJeyapalan et al., 20089No documentation on partial tearsZhang et al., 20128100 (100, 100)100 (100, 100)100100N/AN/AN/AAl-Hourani et al., 201838No documentation on partial tearsAkhavan et al., 201939No documentation on partial tearsBekhet et al., 20215100 (100, 100)100 (100, 100)100100N/AN/AN/AMeisami et al., 20214086.5 (73.1, 99.9)72.2 (54.6, 89.8)81.878.93.120.18716.684Bezirgan et al., 202341No documentation on partial tearsCI, Confidence interval; PPV, positive predictive value; NPV, negative predictive value; LR+, positive likelihood ratio; LR-, negative likelihood ratio.
Quality of included studies
The quality of included studies was assessed using the GRADE tool.11 Limitations, results inconsistency, evidence indirectness, imprecision, and publication bias were all considered when assessing each study. Three studies were deemed low quality, one study was assessed as moderate quality, and four studies were high quality (see Table 5). Studies were generally considered low/ moderate quality due to lower effect magnitudes, inconsistency, and indirectness.Table 5. Study design and GRADE rating.Table 5. StudyStudy designQuality of assessment (GRADE)Wang et al., 199937Retrospective cohort studyLowLee et al., 20006Prospective cohort studyLowJeyapalan et al., 20089Retrospective case control studyLowZhang et al., 20128Randomized controlled studyHighAl-Hourani et al., 201838Retrospective case control studyModerateAkhavan et al., 201939Prospective cohort blind studyHighBekhet et al., 20215Prospective cohort studyHighMeisami et al., 202140Prospective cohort studyHighBezirgan et al., 202341Retrospective case control studyHigh
Risk of bias
The only randomized control trial had a high risk of bias due to allocation concealment bias. ROB2 was used to assess RCTs in this study12 (see Table 6). Included non-randomized clinical studies were assessed against the ROBINS-I risk of bias tool.13 Non-RCTs generally had a moderate to high risk of bias due to selection, comparability and outcome metrics (see Table 7).Table 6ROB 2 risk of bias analysis of RCTs.Table 6. Image, table 6Table 7ROBINS-I risk of bias analysis of Non-RCTs.Table 7. Image, table 7
Outcomes
Outcomes were assessed by calculating the overall positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LR+), negative likelihood ratio (LR-) and diagnostic odds ratio (DOR). Overall pre-operative USS findings for complete primary flexor tendon injuries were as follows (pooled mean ± SD): sensitivity (88.78 % ± 17.06), specificity (92.23 % ± 13.17), PPV (94.81 % ± 7.46), NPV (77.40 % ± 37.65), LR+ (96.64 ± 134.20), LR- (0.26 ± 0.28) and DOR (324.11 ± 585.29). Summary of pre-operative USS findings for incomplete primary flexor tendon injuries were as follows (pooled mean ± SD): sensitivity (0.67 % ± 0.58), specificity (66 % ± 0.57), PPV (63 % ± 0.55), NPV (67 % ± 0.58), LR+ (19.23± 27.19), LR- (0 ± 0) and DOR (N/A).
Discussion
This systematic review has shown that USS is capable of predicting flexor tendon injuries in both pre- and peri‑operative settings following trauma. USS identified 236 complete and partial flexor tendon injuries amongst the 593 injured tendons. This systematic review demonstrated high sensitivity and specificity in identifying complete primary flexor tendon injuries using USS.
Benefits of USS use
USS provides considerable advantages in the assessment and diagnosis of flexor tendon injuries during the pre-operative phase. USS provides real-time, dynamic imaging, allowing clinicians to assess tendon integrity and function without requiring invasive diagnostic procedures.5^,^7 This eliminates the risks associated with exploratory surgery, which is often used to determine the extent of tendon damage. Avoiding this using USS can potentially prevent unnecessary surgical interventions for patient care.14 Across the medical literature, USS has proven to significantly reduce the time, cost, and environmental impact of operative procedures.15 The materials used intraoperatively and the energy consumption required for operating rooms add to the environmental footprint and medical waste.16 Avoiding surgery through precise USS diagnosis could reduce these environmental impacts.
USS is valuable for visualizing flexor tendons17 in real-time, thereby avoiding complications such as neurovascular injury. In clinically indicated tendon explorations, USS assists in targeted and tailored incisions, minimizing extensive tissue dissection and reducing operative time.18 This, in turn, could decrease patient recovery time, thereby lowering healthcare costs and freeing up surgical resources.19 The use of USS could potentially lead to a reduction in treatment delays, improved patient flow pathways, and enhanced clinical decision-making in trauma settings.
Localizing the proximal cut-end of the tendon in flexor tendon injuries through USS is beneficial both in the initial operation and in delayed presentations.6 With these levels of specificity and sensitivity, USS could help in tailored surgical management by determining suitability for primary repair. In acute cases, real-time tendon visualization can better facilitate minimally invasive techniques, such as wide-awake local anesthesia with no tourniquet (WALANT).20 Using USS in conjunction with WALANT could facilitate higher precision in repairs and avoid extensive tissue dissection, thus resulting in less intraoperative trauma and faster recovery times.21
Minimizing scarring is crucial, as extensive scarring in flexor tendon repairs is associated with higher rates of adhesions.22 Adhesions can limit tendon gliding, worsen stiffness, reduce range of motion, and exacerbate chronic pain. Furthermore, prolonged healing times due to scarring can significantly impact a patient’s quality of life and daily activities.23 Complications increase with larger incisions, such as a higher risk of wound breakdown and infection, requiring more dressings, antibiotics, frequent outpatient appointments, and potentially extended hospital inpatient stays.
A minimally invasive approach that encourages early mobilization may reduce these aforementioned risks.24 Fewer post-operative complications and faster rehabilitation may prevent further revision operations and intensive physiotherapy, thereby improving long-term outcomes and alleviating the burden on hand trauma units and other healthcare costs.25
Overall, USS offers a non-invasive, potentially cost-effective, and environmentally-friendly alternative to traditional diagnostic and surgical approaches for flexor tendon injuries, enhancing patient care while minimizing unnecessary resource use.
User operability
Across the analyzed studies in this systematic review, USS operators varied from experienced surgeons to experienced emergency clinicians, radiologists, and radiographers. The operator's experience heavily influences the effectiveness of USS in diagnosing and managing flexor tendon injuries.26 Clinicians with significant USS experience are more adept at identifying nuanced tendon pathology, such as tears, inflammation, and vascularity, demonstrating a clear advantage in preoperative and perioperative settings, which allows for better preoperative planning and perioperative guidance.7^,^27 USS requires a strong understanding of hand anatomy and the ability to interpret dynamic imaging in real-time, which can prove challenging for novices.28 Several countries have established training courses and assessments in USS to lessen the learning curve for trainee clinicians and medical students.29, 30, 31
Despite this learning curve, USS is relatively user-friendly once proficiency is attained. Portable machines and technological advancements have made USS accessible and practical, even in peri‑operative settings.7 With the development of pocket ultrasound devices such as Butterly iQ™32 and Clarius,33 trained surgeons can readily perform perioperative and intraoperative scans, eliminating the need for referral to sonographers.34 For surgeons, using USS can streamline decision-making, potentially reducing the need for more invasive diagnostic techniques. Training programs and standardized protocols can help bridge the gap between novice and experienced users, promoting a broader user base for flexor tendon injury management.35
Partial flexor tendon injuries
Determining the degree of partial tendon injury is necessary for clinical decisions to operate; typically, a partial flexor tendon injury of >60 % cross-sectional area should be repaired.36 However, following the main findings of this systematic review study, USS has been deemed ineffective in detecting partial flexor tendon injuries of the hand. Poor sensitivity, specificity, PPV, and NPV values demonstrate the ineffective use of USS in such cases. Across the finalized studies, the degree to which a partial injury was elicited on USS was not recorded by the majority of studies (n = 8).
Despite demonstrating the high sensitivity and specificity of determining complete primary flexor tendon injuries, this review has not been able to demonstrate efficacy and accuracy in partial injuries. Across the studies examined, there were instances of under-reporting of partial tendon injuries or amalgamating partial and complete injuries when discussing accuracy statistics. In such cases, this systematic review has appropriately recorded such events for clarity. Given the results of this systematic review, the use of USS is recommended to identify complete flexor tendon injuries.
In conclusion, there are currently no systematic reviews in the literature that have assessed the accuracy of USS in evaluating flexor tendon injuries during the pre-operative phase. Only one RCT has focused on this subject,8 and a small sample size limits its findings. The findings of this systematic review demonstrate the accuracy and utility of USS in diagnosing and monitoring complete flexor tendon injuries, supporting its integration into standard clinical practice. More high-quality RCTs with larger cohorts are necessary to validate these results further and reinforce the role of USS in managing flexor tendon injuries.
Contributions
Ryan Faderani: Conceptualisation, data curation, writing and editing. Shaikh Sanjid Seraj: Data curation, formal analysis, writing. Puneh Shahrjerdi: Data curation, formal analysis, writing. Garikai Kungwengwe: Data curation, formal analysis. Muholan Kanapathy: Review and editing. Dariush Nikkhah: Review and editing. Afshin Mosahebi: Review and editing.
Funding
None.
Ethical approval
Not required.
Conflicts of interest
None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tang J.B.Flexor tendon injuries Clin Plast Surg 463201929530610.1016/j.cps.2019.02.00331103074 · doi ↗ · pubmed ↗
- 2Hernandez J.D.Stern P.J.Complex injuries including flexor tendon disruption Hand Clin 212200518719710.1016/j.hcl.2004.12.00115882598 · doi ↗ · pubmed ↗
- 3Sobhy T.Bayoumi S.Assy M.Abdulsalam E.Ultrasonography role for evaluation of hand tendon injuries Egypt J Hosp Med 86202213013410.21608/ejhm.2022.210787 · doi ↗
- 4Baz A.A.M.Hussien A.B.Samad H.M.A.El-Azizi H.M.S.Diagnostic performance of high-resolution ultrasound in pre- and postoperative evaluation of the hand tendons injuries Egypt J Radiol Nucl Med 5212021610.1186/s 43055-020-00375-z · doi ↗
- 5Bekhet C.N.H.Ghaffar M.K.A.Nassef M.A.Khattab R.T.Role of ultrasound in flexor tendon injuries of the hand: a new insight Ultrasound Med Biol 47820212157216610.1016/j.ultrasmedbio.2021.02.02333934941 · doi ↗ · pubmed ↗
- 6Lee D.H.Robbin M.L.Galliott R.Graveman V.A.Ultrasound evaluation of flexor tendon lacerations J Hand Surg Am 252200023624110.1053/jhsu.2000.jhsu 25a 023610722814 · doi ↗ · pubmed ↗
- 7Gudimella R.Dow T.Krauss E.M.Lalonde D.H.Surgeon-performed ultrasound in flexor tendon injury management: a practical guide Plast Reconstr Surg Glob Open 11122023 e 546710.1097/GOX.0000000000005467 PMC 1071834938093729 · doi ↗ · pubmed ↗
- 8Zhang G-Y Zhuang H-Y Wang L-X Value of high frequency ultrasonography in diagnosis and surgical repair of traumatic finger tendon ruptures Med Princ Pract 215201247247510.1159/00033640522377840 · doi ↗ · pubmed ↗