Managing Cytomegalovirus Infection in Lung Transplant Recipients in Real Life: Results of a French Multicenter Survey
Tiphaine Goletto, Kinan El Husseini, Antoine Roux, Mathilde Briard, Gaelle Dauriat, Benjamin Renaud-Picard, Claire Merveilleux du Vignaux, Loic Falque, Benjamin Coiffard, Thomas Villeneuve, Xavier Demant, Adrien Tissot, Domitille Mouren, Francois M. Carlier, Sophie Alain

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
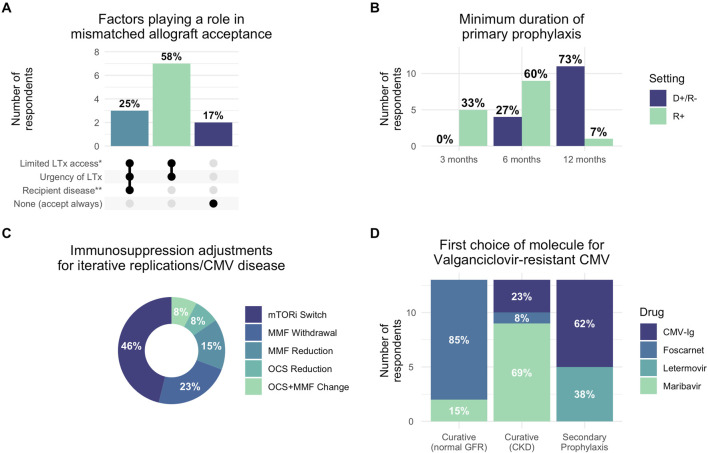 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Transplantation: Methods and Outcomes · Renal Transplantation Outcomes and Treatments
Dear Editors, Cytomegalovirus (CMV) infection remains a major cause of morbidity and mortality following lung transplantation (LTx), with lung recipients facing particularly high risk due to substantial lung-associated lymphoid tissue harbouring latent CMV [1]. Beyond direct effects, CMV infection increases risks for acute rejection, chronic allograft dysfunction, and opportunistic infections. While international guidelines provide recommendations for CMV management [2–4], real-world adherence in LTx centres remains poorly characterized, particularly given that they represented only 15% of transplant centres in recent broader surveys despite bearing the highest CMV burden [5].
We conducted a cross-sectional survey of 10 French-speaking LTx centres [9 out of 11 French centres (82%) and 1 out of 4 Belgian centres (25%)] between September 2022 and February 2023, using a comprehensive questionnaire addressing CMV prevention, diagnosis, treatment, and resistance management. Fifteen physicians participated, with 13 of 15 (86%) reporting adherence to centre-specific protocols that varied between institutions. All physicians surveyed were pulmonologists and lung transplant specialists, who routinely manage LTx patients and CMV infection in this population. Details regarding our methodology, the questionnaire in itself, as well as the full responses, are available in our Supplementary Material.
Our findings revealed substantial heterogeneity in CMV management practices with significant deviations from established guidelines (Figure 1). Most strikingly, prophylaxis duration showed concerning variability: in seropositive recipients (R+), 5 of 15 respondents (33%) used only 3 months of prophylaxis despite guidelines recommending 6–12 months [3, 4], while 9 of 15 (60%) used 6 months and 1 of 15 (7%) used 12 months. For high-risk donor-positive/recipient-negative (D+/R-) patients, 11 of 15 (73%) appropriately used 12-month prophylaxis, though 4 of 15 (27%) used shorter durations. In R+ patients with short telomere syndrome, which is associated with impaired CMV immunity and increased treatment toxicity [6], 10 of 13 respondents (84%) used standard valganciclovir prophylaxis, with 2 of 13 (16%) employing alternative approaches such as anti-CMV immunoglobulins or valaciclovir.
Secondary prophylaxis practices diverged markedly from 2018 guidelines that recommended against routine use [3]. After CMV reactivation, 5 of 14 respondents (36%) systematically initiated secondary prophylaxis with an additional 2 of 14 (14%) using it conditionally. Following CMV disease, these proportions increased to 8 of 14 (57%) and 3 of 14 (21%), respectively. All respondents maintained secondary prophylaxis for 3 months. For patients with iterative replications, 11 of 14 (79%) used long-term prophylaxis with durations varying from 3 to 12 months. This widespread adoption likely reflects the clinical reality that LTx recipients experience higher CMV recurrence rates compared to other solid organ transplant recipients.
Post-prophylaxis monitoring also showed substantial variation, with 6 of 15 respondents (40%) performing monthly monitoring in R+ patients, while in D+/R- patients, 5 of 15 (33%) performed monthly monitoring and 4 of 15 (27%) performed weekly monitoring. This heterogeneity emerged despite 2018 guidelines not supporting surveillance after prophylaxis, though updated 2025 guidelines now suggest monitoring in high-risk patients [4]. CMV-specific cellular immune response testing was used by only 4 of 13 respondents (31%), reflecting limited adoption of these newer diagnostic tools despite their potential for personalized management.
Immunosuppression modification was considered by 5 of 13 respondents (38%) for CMV disease and 12 of 13 (92%) for recurrent infections, most commonly involving mTOR inhibitor introduction or antimetabolite reduction. For hematologic toxicity, 10 of 14 (71%) appropriately used hematologic support, though 2 of 14 (14%) modified immunosuppression and 1 of 14 (7%) reduced valganciclovir doses as first-line interventions, potentially increasing resistance risk [7].
Resistant CMV management revealed evolving practices influenced by new therapeutic options, highlighting both opportunities and challenges in this complex clinical scenario. For patients with normal renal function, 11 of 13 (85%) preferred foscarnet over maribavir (2 of 13, 15%), while in renal impairment, maribavir was preferred by 9 of 13 (69%). Anti-CMV immunoglobulins were used by 8 of 12 respondents (67%) for secondary prophylaxis in resistant cases, with letermovir usage varying widely (8 of 13 (61%) never used it, while others employed it in specific scenarios).
The availability of maribavir through compassionate use programs during our survey period and its subsequent broader approval likely influenced these preferences [8]. Nearly all respondents would test for ganciclovir resistance in case of reactivation despite preventive treatment (11 of 13, 85%) or failure of curative treatment (12 of 13, 93%). These findings underscore the challenges clinicians face when managing resistant CMV, particularly the need to balance efficacy against drug-specific toxicity profiles in an already immunocompromised population with limited access to resistance testing.
The widespread practice variation we observed is particularly significant given that participating centres employ similar immunosuppression protocols and serve comparable populations. Our sample comprised nearly all French LTx centres, suggesting these findings reflect national practice patterns. Similar variability has been reported in Italian programmes [9] and broader European surveys [10], indicating these challenges transcend national boundaries.
The clinical implications are concerning. Santos et al. demonstrated that delayed-onset CMV disease following prophylaxis discontinuation occurs in up to 14% of LTx recipients with associated mortality risk [2]. Our finding that one-third of respondents use only 3-month prophylaxis in R+ patients may have significant clinical consequences, particularly when considering that breakthrough infections may increase resistance risk, impacting long-term allograft survival. Encouragingly, many practice variations we documented have been partially addressed in updated 2025 guidelines [4], which incorporate more aggressive secondary prevention strategies and suggest post-prophylaxis monitoring in high-risk patients, reflecting growing recognition of LTx-specific challenges.
While our study has limitations, including modest sample size and focus on French-speaking centres, our comprehensive coverage of French centres provides valuable insights into an underrepresented but high-risk population. The documented practice heterogeneity, particularly deviations from evidence-based recommendations, highlights critical gaps in CMV management standardization. The fact that 86% of respondents follow centre-specific protocols suggests local guidelines themselves diverge from international recommendations. The higher CMV burden in LTx recipients compared to other solid organ transplant populations necessitates specialized management approaches addressing unique challenges including optimal prophylaxis duration and management of patients with conditions like short telomere syndrome. These findings underscore the need for enhanced education, practice standardization initiatives, and generation of LTx-specific evidence to support future guideline development.
In conclusion, this survey reveals significant heterogeneity in CMV management among French-speaking LTx centres, with notable deviations from international guidelines. Given CMV’s substantial impact on LTx outcomes, addressing these variations through enhanced education, standardized protocols, and LTx-specific evidence generation should be a priority for the transplant community.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zamora MR. Cytomegalovirus and Lung Transplantation. Am J Transplant (2004) 4(8):1219–26. 10.1111/j.1600-6143.2004.00505.x 15268722 · doi ↗ · pubmed ↗
- 2Santos CAQ Brennan DC Yusen RD Olsen MA. Incidence, Risk Factors and Outcomes of Delayed-Onset Cytomegalovirus Disease in a Large Retrospective Cohort of Lung Transplant Recipients. Transplantation (2015) 99(8):1658–66. 10.1097/TP.0000000000000549 25675196 PMC 4534357 · doi ↗ · pubmed ↗
- 3Kotton CN Kumar D Caliendo AM Huprikar S Chou S Danziger-Isakov L The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation. Transplantation (2018) 102(6):900–31. 10.1097/TP.0000000000002191 29596116 · doi ↗ · pubmed ↗
- 4Kotton CN Kumar D Manuel O Chou S Hayden RT Danziger-Isakov L The Fourth International Consensus Guidelines on the Management of Cytomegalovirus in Solid Organ Transplantation. Transplantation (2025) 109:1066–110. 10.1097/TP.0000000000005374 40200403 PMC 12180710 · doi ↗ · pubmed ↗
- 5Grossi PA Kamar N Saliba F Baldanti F Aguado JM Gottlieb J Cytomegalovirus Management in Solid Organ Transplant Recipients: A Pre-COVID-19 Survey From the Working Group of the European Society for Organ Transplantation. Transpl Int (2022) 35:10332. 10.3389/ti.2022.10332 35812158 PMC 9257585 · doi ↗ · pubmed ↗
- 6Popescu I Mannem H Winters SA Hoji A Silveira F Mc Nally E Impaired Cytomegalovirus Immunity in Idiopathic Pulmonary Fibrosis Lung Transplant Recipients with Short Telomeres. Am J Respir Crit Care Med (2019) 199(3):362–76. 10.1164/rccm.201805-0825 OC 30088779 PMC 6363970 · doi ↗ · pubmed ↗
- 7Stevens DR Sawinski D Blumberg E Galanakis N Bloom RD Trofe-Clark J. Increased Risk of Breakthrough Infection Among Cytomegalovirus Donor-Positive/Recipient-Negative Kidney Transplant Recipients Receiving Lower-Dose Valganciclovir Prophylaxis. Transpl Infect Dis (2015) 17(2):163–73. 10.1111/tid.12349 25661673 · doi ↗ · pubmed ↗
- 8Avery RK Alain S Alexander BD Blumberg EA Chemaly RF Cordonnier C Maribavir for Refractory Cytomegalovirus Infections with or Without Resistance Post-Transplant: Results from a Phase 3 Randomized Clinical Trial. Clin Infect Dis (2022) 75(4):690–701. 10.1093/cid/ciab 988 34864943 PMC 9464078 · doi ↗ · pubmed ↗