Cost-Effectiveness of Durvalumab After Chemoradiotherapy in Limited-Stage SCLC
Sheng-Han Tsai, Jui-Hung Tsai, Li-Jun Chen, Szu-Chun Yang

TL;DR
This study evaluates whether adding durvalumab after chemoradiotherapy for limited-stage small cell lung cancer is cost-effective in Taiwan, finding it is not unless the drug's price is significantly reduced.
Contribution
The study provides a cost-effectiveness analysis of durvalumab consolidation therapy in limited-stage SCLC from the perspective of the Taiwanese healthcare system.
Findings
Durvalumab consolidation therapy had an ICER of $101,734 per QALY, exceeding the $70,000 threshold.
Reducing durvalumab's cost to $3,893 per 4 weeks could make it cost-effective.
The therapy had only a 0.3% probability of being cost-effective at the willingness-to-pay threshold.
Abstract
In the ADRIATIC trial, durvalumab consolidation therapy improved the overall survival and progression-free survival of patients with limited-stage SCLC responding to chemoradiotherapy. Based on the data, we aim to assess the cost-effectiveness of the therapy from the perspective of the Taiwanese health care sector. Simulated patients with limited-stage SCLC responding to chemoradiotherapy were entered into a partitioned survival model comparing durvalumab consolidation with no consolidation therapy. The model inputs were derived from the ADRIATIC trial (survival outcomes, adverse events, and subsequent therapies), National Health Insurance payments (costs of physician visits, monitoring, drug administration, and end-of-life care), and the hospital cohort (utility values). A lifetime horizon and annual discount rate of 3% were applied. Subgroup, one-way deterministic, and probabilistic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
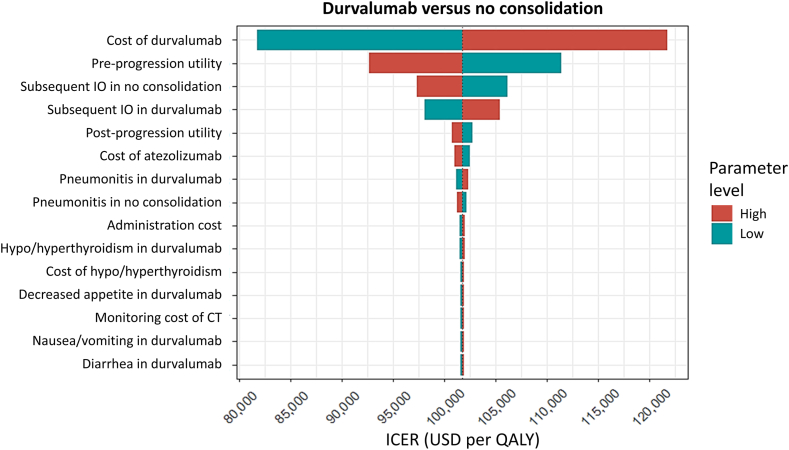 Figure 1
Figure 1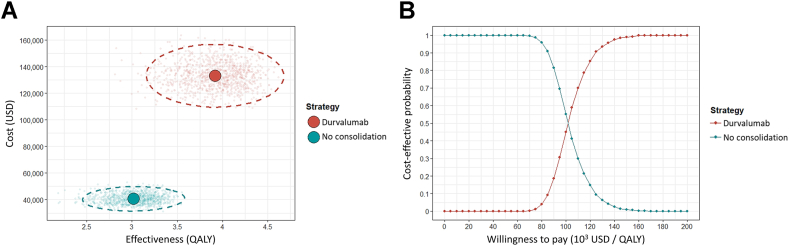 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Research Studies · Lung Cancer Treatments and Mutations · Neuroendocrine Tumor Research Advances
Introduction
Lung cancer is the leading cause of cancer-related deaths worldwide.1 SCLC is the most aggressive histologic subtype of lung cancer. Approximately one-third of patients with SCLC are diagnosed at a limited stage.2 Definitive chemoradiotherapy with concurrent use of etoposide-platinum and thoracic irradiation has been the standard of care for these patients for the past three decades.3 Only recently have there been advances in treatment for limited-stage SCLC. In September 2024, durvalumab, a programmed death-ligand 1 inhibitor, became the first efficacious consolidation immunotherapy for patients with limited-stage SCLC whose disease has not progressed after concurrent chemoradiotherapy.4 According to the ADRIATIC trial, durvalumab consolidation therapy, compared with no consolidation therapy, led to longer median overall survival (OS) (55.9 versus 33.4 mo) and progression-free survival (PFS) (16.6 versus 9.2 mo). Following this evidence, durvalumab consolidation therapy was recommended in the National Comprehensive Cancer Network Clinical Practice Guidelines for SCLC.5 The U.S. Food and Drug Administration also approved this regimen in December 2024.6
Despite the proven clinical benefits of durvalumab consolidation therapy in limited-stage SCLC, maintenance use of this expensive drug imposes profound financial consequences for the health care system. Several previous analyses have evaluated the cost-effectiveness of durvalumab consolidation therapy in patients with stage III NSCLC.7, 8, 9, 10, 11, 12, 13, 14, 15 Evidence suggests that durvalumab consolidation therapy is more cost-effective than no consolidation therapy.7, 8, 9, 10, 11, 12, 13^,^15 Other researchers have studied the economic outcomes of durvalumab with chemotherapy in the first-line treatment of extensive-stage SCLC and concluded that the immunotherapy and chemotherapy combination is not a cost-effective option.16, 17, 18, 19, 20 However, no study has explored the cost-effectiveness of durvalumab consolidation therapy in patients with limited-stage SCLC.
On the basis of the published results of the ADRIATIC trial4 and considering the costs of drug waste, adverse events (AEs), physician visits, disease monitoring, and end-of-life care, we investigated the cost-effectiveness of durvalumab consolidation therapy versus no consolidation therapy for patients with limited-stage SCLC responding to definitive chemoradiotherapy.
Model Overview
A partitioned survival model was created to simulate patients with limited-stage SCLC who received durvalumab consolidation therapy or no consolidation therapy after concurrent chemoradiotherapy (Supplementary Fig. 1). Simulated patients with a WHO performance status score of 0 to 1 and without disease progression after concurrent chemoradiotherapy were included in the model. During durvalumab consolidation therapy, patients received 1500 mg of durvalumab every 4 weeks until disease progression or for a maximum of 24 months. Contrastingly, patients in the nonconsolidation therapy group did not receive anticancer therapy until disease progression. After disease progression, patients in both groups received cytotoxic chemotherapy with or without immunotherapy. Etoposide and carboplatin were selected as the subsequent chemotherapy, as most patients in either group had a progression-free interval of more than 6 months,4 and retreatment with etoposide-platinum was considered.5 The probabilities of subsequent immunotherapy in both strategies were directly derived from the ADRIATIC trial. A model length of 4 weeks was selected for this study because durvalumab was administered every 4 weeks. A lifetime horizon and an annual discount rate of 3% for future costs and life-years were applied. This economic analysis followed the Consolidated Health Economic Evaluation Reporting Standards guideline (Supplementary Table 1).21
Survival Estimates
A web-based software (WebPlotDigitizer; https://automeris.io/WebPlotDigitizer/) was used to extract the PFS and OS curves of durvalumab and placebo groups from the ADRIATIC trial.4 The digitized PFS and OS data were translated into imitated patient-level information using the function “digitise ()” in R software.22^,^23 Parametric models (i.e., loglogistic, Weibull, lognormal, gamma, generalized gamma, exponential) were fit to the data. The model with the most appropriate fit, on the basis of the Akaike Information Criterion or Bayes Information Criterion, was selected. To avoid the logical fallacy of the partitioned survival model, parametric models that produced an extended PFS tail exceeding the OS were excluded. Using the selected parametric models, PFS and OS were extrapolated to the lifetime horizon. Hence, the proportions of patients in the preprogression, postprogression, or death stages at each cycle for both strategies were derived. The modeled PFS and OS curves of the durvalumab consolidation and no consolidation groups were compared with the ADRIATIC trial results.4
Cost and Utility Input
This cost-effectiveness analysis was conducted from the perspective of the Taiwanese health care sector. Direct medical costs, on the basis of payments from the National Health Insurance (NHI), were considered. These included per-cycle costs of physician visits, general monitoring (chest radiography, hemogram, and biochemistry tests), computed tomography, drug administration, and a one-off cost of end-of-life care (Table 1).24 A body weight of 70 kg, a body surface area of 1.84 m^2^, and a glomerular filtration rate of 73 mL/min (i.e., a 65-year-old man with a serum creatinine level of 1 mg/mL) were applied to estimate the doses of anticancer drugs. When calculating the costs of intravenous agents, drug waste was considered by rounding up partially used vials (Supplementary Table 2). In addition, the costs attributable to AEs were estimated by multiplying the incidence rate of AEs by the cost of the respective AEs.25 We used the 2024 exchange rate for Taiwan dollars to US dollars (USD).26Table 1. Model ParametersaParameterValueRangeDistributionSourceProportion of patients in the pre/postprogression state, durvalumab consolidationTime-variant----ADRIATIC durvalumab’s PFS/OS curves4Proportion of patients in the pre/postprogression state, no consolidationTime-variant----ADRIATIC placebo’s PFS/OS curves4Subsequent therapy, durvalumab consolidation Cytotoxic chemotherapy100%----ADRIATIC trial4 Immunotherapy20.7%16.6%–24.9%beta (17, 65)ADRIATIC trial4Subsequent therapy, no consolidation Cytotoxic chemotherapy100%----ADRIATIC trial4 Immunotherapy27.2%21.8%–32.6%beta (31, 83)ADRIATIC trial4Cost of physician visit, USD1210–14gamma (100, 0.12)NHI payment24Monitoring cost per 4 weeks, USD General monitoringb2822–34gamma (100, 0.28)NHI payment24 CT with contrast5242–63gamma (100, 0.52)NHI payment24Administration cost, USD6956–83gamma (100, 0.69)NHI payment24Drug cost per 4 weeks, USD Durvalumab57394591–6887gamma (100, 57.39)NHI payment Etoposide6552–77gamma (100, 0.65)NHI payment Cisplatin5342–63gamma (100, 0.53)NHI payment Carboplatin266213–319gamma (100, 2.66)NHI payment Atezolizumab41633330–4995gamma (100, 41.63)NHI paymentCost of end-of-life care,c USD30272421–3632gamma (100, 30.27)NHI payment24Health utility Preprogression0.830.75–0.92beta (16.2, 3.3)EQ-5D27 Postprogression0.720.65–0.79beta (27.3, 10.6)EQ-5D27CT, computed tomography; EQ-5D, European Quality of Life-Five Dimensions; NHI, National Health Insurance; PFS, progression-free survival; OS, overall survival; USD, US dollars.aSupplementary Table 3 for parameters of adverse events.bChest radiography, hemogram, and biochemistry tests.cHospice consultation, home hospice care, and ward hospice care.
On the basis of a hospital cohort’s data using Taiwanese tariffs,27 a utility value of 0.83 was applied for patients with limited-stage SCLC receiving immunotherapy in the preprogression state. In the ADRIATIC trial, 86.3% in the durvalumab group and 89.8% in the placebo group used chemotherapy as the subsequent anticancer therapies.4 We applied a utility value of 0.72 for patients in the postprogression state receiving cytotoxic chemotherapy.27
Base-Case Analysis
The incremental cost-effectiveness ratio (ICER) was estimated as the incremental cost divided by the quality-adjusted life-year (QALY). The WHO recommends a cost-effectiveness threshold of 1 to 3 times the gross domestic product (GDP) per capita.28 Moreover, the willingness of Taiwanese people to pay for a QALY is approximately 1.57 to 2.15 times the per capita GDP.29 Thus, the willingness-to-pay (WTP) threshold was set at two times the Taiwanese GDP per capita in 2024, which was 70,000 USD.30 The net monetary benefit of each strategy was calculated as the product of QALY and WTP minus the total cost. All analyses were conducted using R version 4.4.1 (The R Foundation for Statistical Computing, Vienna, Austria).
Subgroup Analyses
The PFS and OS curves of patients with or without prophylactic cranial irradiation, undergoing twice-daily or once-daily previous radiotherapy schedules, and receiving carboplatin-etoposide or cisplatin-etoposide as previous chemotherapy differed from those of the overall patient population.31 Therefore, PFS and OS data for each subgroup were fitted, and survival estimates and chemotherapy regimens were varied accordingly for the subgroup analyses.
Deterministic and Probabilistic Analyses
A one-way deterministic analysis was conducted, and a tornado diagram was generated by varying the probabilities of subsequent immunotherapies, costs of physician visits, monitoring, administration, drugs, end-of-life care, health utilities, incidence rates of AEs, and costs for AEs within plausible ranges (Table 1 and Supplementary Table 3). To address the effects of parameter uncertainties, a probabilistic analysis using a Monte Carlo simulation with 1000 iterations was conducted. A cost-effectiveness scatterplot and acceptability curve were also generated.
Ethics Statement
This model-based cost-effectiveness analysis was approved by the institutional review board of the National Cheng Kung University Hospital (B-ER-114-165). Informed consent was waived as data was obtained from a published literature review and deidentified information.
Results
Base-Case Analysis
The modeled PFS and OS curves for patients in the durvalumab consolidation and no consolidation groups are illustrated in Supplementary Figure 2. On the basis of the AIC and BIC of each parametric model (Supplementary Table 4), log-normal distributions were selected. We extrapolated the PFS and OS curves of durvalumab consolidation and no consolidation to a lifetime horizon, as the PFS and OS probabilities of durvalumab did not approach zero in 20 years. The selected PFS and OS curves closely resembled those reported in the ADRIATIC trial, indicating good calibration of the partitioned survival model. The generalized gamma distribution, which produced extended PFS tails exceeding OS tails, was not selected for modeling the PFS curves.
Compared with no consolidation therapy, durvalumab consolidation therapy incurred an additional cost of 91,734 USD and resulted in 0.90 QALY (1.00 life-years) gained ([Table 2](#tbl2)). Consequently, the ICER was 101,734 USD per QALY (83,194 USD per life-year). The primary driver of the total cost and the cost difference between the two strategies was the drug cost. The costs of physician visits, disease monitoring, AEs, and end-of-life care played only minor roles in the total cost and cost differences. Likewise, preprogression QALY (life-year) constituted the main difference in effectiveness. Postprogression QALYs (life-years) did not differ between the two groups. No consolidation therapy revealed a higher net monetary benefit (142,114 USD). The incremental net monetary benefit was $28,615 USD.Table 2. Base-Case ResultsStrategyCosts (USD)Life-YearsQALYsCost Per Life-Year (USD)Cost Per QALY (USD)Net Monetary Benefit (USD)No consolidationTotal cost: 40,686Physician visits: 560Monitoring: 3731Drugs: 27,021Adverse events: 6347End-of-life care: 3027Total: 3.83Preprogression: 2.38Postprogression: 1.45Total: 3.02Preprogression: 1.98Postprogression: 1.04----170,729Durvalumab consolidationTotal cost: 132,420Physician visits: 721Monitoring: 4805Drugs: 115,330Adverse events: 8537End-of-life care: 3027Total: 4.93Preprogression: 3.36Postprogression: 1.57Total: 3.92Preprogression: 2.79Postprogression: 1.1383,194101,734142,114QALY, quality-adjusted life-year; USD, US dollars.
Subgroup Analyses
Patients receiving prophylactic cranial irradiation, undergoing a twice-daily previous radiotherapy schedule, and using carboplatin-etoposide as previous chemotherapy revealed longer QALYs (life-years) than all other patients (Table 3). Specifically, patients using carboplatin-etoposide as a previous chemotherapy had the lowest ICER of 53,637 USD per life-year), whereas the highest ICER of 141,331 USD per life-year) was noted in patients using cisplatin-etoposide as a previous chemotherapy. Subgroups of patients other than those using carboplatin-etoposide as a previous chemotherapy revealed a lower net monetary benefit of durvalumab consolidation therapy compared with no consolidation therapy.Table 3. Subgroup AnalysisStrategyTotal Costs (USD)Life-YearsQALYsCost Per Life-Year (USD)Cost Per QALY (USD)Net Monetary Benefit (USD)Receipt of prophylactic cranial irradiation No consolidation46,8394.533.57----203,050 Durvalumab consolidation139,4235.634.5183,99098,817176,051No receipt of prophylactic cranial irradiation No consolidation36,2013.092.42----133,485 Durvalumab consolidation122,1264.103.2384,853106,763103,897Twice-daily previous radiotherapy schedule No consolidation57,8934.703.65----197,385 Durvalumab consolidation151,1756.074.7468,06085,219180,726Once-daily previous radiotherapy schedule No consolidation37,2753.662.90----165,446 Durvalumab consolidation126,6364.583.6796,704115,583130,204Previous chemotherapy: carboplatin-etoposide No consolidation40,7773.843.02----170,870 Durvalumab consolidation146,9415.814.5653,63769,257172,009Previous chemotherapy: cisplatin-etoposide No consolidation42,7673.943.10----173,953 Durvalumab consolidation125,6494.523.63141,331156,370128,174QALY, quality-adjusted life-year; USD, US dollars.
Deterministic and Probabilistic Analyses
The tornado diagram of durvalumab consolidation therapy versus no consolidation therapy revealed that the cost of durvalumab, the utility value of the preprogression state, and probabilities of subsequent immunotherapy in both strategies were the major determinants of the ICER (Fig. 1). If the 4-week cost of durvalumab could be further reduced to $3893 USD, durvalumab consolidation therapy would become a cost-effective strategy.Figure 1. Tornado diagram of durvalumab consolidation therapy versus no consolidation therapy. The dotted line represents the base-case ICER. CT, computed tomography; ICER, incremental cost-effectiveness ratio; IO, immunotherapy; QALY, quality-adjusted life-year; USD, US dollars.
The cost-effectiveness scattergram (Fig. 2A) illustrates that the 95% confidence ellipse of durvalumab consolidation therapy did not overlap with that of no consolidation therapy. Durvalumab consolidation therapy had probabilities of 0.0%, 0.3%, and 58.8% of being cost-effective at WTP thresholds of 70,000 USD (two per capita GDP), and $105,000 USD (three per capita GDP) per QALY, respectively (Fig. 2B).Figure 2. Cost-effectiveness (A) scattergram and (B) acceptability curves of durvalumab consolidation and no consolidation approaches. The dashed circles in (A) indicate the 95% confidence ellipses. QALY, quality-adjusted life-year; USD, US dollars.
Discussion
This study is the first to evaluate the cost-effectiveness of durvalumab after chemoradiotherapy for patients with limited-stage SCLC. Using a partitioned survival model and directly simulating the PFS, OS, AE, and subsequent therapy data from the ADRIATIC trial (Table 1 and Supplementary Table 3),4 we found that durvalumab consolidation therapy was not cost-effective compared with no consolidation therapy from the perspective of the Taiwanese health care sector. Considering the costs of physician visits, disease monitoring, drug waste (Supplementary Table 2), and end-of-life care, the ICER was 70,000 USD per QALY (Table 2).
In contrast to the cost-effectiveness of durvalumab after chemoradiotherapy in stage III NSCLC,7, 8, 9, 10, 11, 12, 13^,^15 our study reveals that durvalumab consolidation therapy is not a cost-effective strategy in limited-stage SCLC. Plausible reasons include greater PFS and OS benefits in the PACIFIC study32^,^33 compared with the ADRIATIC trial.4 The hazard ratio for disease progression in the PACIFIC study was 0.52 (95% confidence interval [CI]: 0.42–0.65), whereas that in the ADRIATIC trial was 0.76 (99.816% CI: 0.53–1.08). Similarly, the hazard ratios for death were 0.68 (99.73% CI: 0.47–0.997) in the PACIFIC trial and 0.73 (98.321% CI: 0.54–0.98) in the ADRIATIC trial. Lower PFS and OS benefits in the ADRIATIC trial led to a higher ICER for durvalumab consolidation versus no consolidation in limited-stage SCLC. In addition, the drug cost constituted the main cost difference between the two strategies. In the PACIFIC study, durvalumab consolidation therapy was administered only for a maximum of 12 months, whereas in the ADRIATIC trial, the therapy was offered for a maximum of 24 months. Longer administration of durvalumab in the ADRIATIC trial resulted in considerable drug costs and increased the cost difference between the durvalumab consolidation and no consolidation strategies.
A survival benefit of durvalumab consolidation compared with no consolidation was seen regardless of the receipt of prophylactic cranial irradiation, previous radiation schedule, and previous chemotherapy regimens.31 Our subgroup analyses fitting each subgroup’s PFS and OS curves reveal that most of the ICERs exceeded the WTP threshold of $70,000 USD per QALY (Table 3), reinforcing the conclusion that durvalumab consolidation therapy is not cost-effective in limited-stage SCLC. In contrast to real-world clinical practice, patients in the trial using cisplatin-etoposide as a previous chemotherapy experienced the lowest survival benefit of durvalumab consolidation compared with no consolidation.31 As a result, durvalumab consolidation therapy is least likely to be cost-effective for these patients.
This study has several policy implications. For example, if the 4-week cost of 1500 mg durvalumab could be further reduced to 3893 USD, reimbursing the drug by Taiwan’s NHI would be feasible (Fig. 1). A trade-off negotiation between drug prices and NHI coverage is indicated. The cost of subsequent immunotherapy in durvalumab consolidation also played a major role in determining cost-effectiveness, emphasizing that readministration of immunotherapy after durvalumab consolidation should be discouraged.
The durvalumab consolidation and no consolidation groups differed significantly in terms of lifetime cost and QALY (Fig. 2A). However, the incremental cost still exceeded the monetary benefit of QALY gained. We acknowledge that the WTP thresholds vary across a broad range according to the recommendations of the WHO.28 By varying the WTP thresholds over a wide range, durvalumab consolidation therapy would be cost-effective if we were willing to pay a QALY for approximately three times the per capita GDP (Fig. 2B).
Although the parametric models with the best fit were selected on the basis of the AIC/BIC, and a generalized gamma distribution was not chosen because it produced extended tails of the PFS curves (Supplementary Fig. 2), our life year estimates were larger than the median survival estimates in the ADRIATIC trial.4 The AIC and BIC of Weibull distributions were much higher than those of the selected log-normal distributions (Supplementary Table 4). However, the Weibull distribution is flexible and is typically used to estimate lifelong cancer survival. If the Weibull distributions were adopted to model the PFS and OS curves, the life years of both strategies would decrease and approximate the trial’s estimates of median survival (Supplementary Table 5). Thus, durvalumab consolidation therapy was not cost-effective in terms of cost per QALY gained ($130,264 USD).
Our study has several limitations. First, we applied the same utility value to patients with a preprogression status receiving durvalumab consolidation or no consolidation therapy. Nevertheless, treatment with durvalumab following chemoradiotherapy in limited-stage SCLC did not have a clinically meaningful detrimental effect on patient-reported outcomes.34 Thus, the QALY gained from durvalumab consolidation versus no consolidation should not be overestimated. Using the same utility values could even underestimate the ICER. Second, we did not consider postprogression second-line therapy. However, the ADRIATIC trial only reported the probabilities of first-line chemotherapy and immunotherapy after disease progression.4 There was also a lack of second PFS information. Synthesizing the second PFS data from another trial (e.g., the IMpower133 study35) might introduce bias as it relies on multiple assumptions, such as similar patient characteristics. Finally, PFS and OS curves in the ADRIATIC trial were used to model the lifetime survival of patients. Patients encountered in real-world practice were usually older and had worse Eastern Cooperative Oncology Group performance statuses than those enrolled in the trial. Consequently, the ICER would be underestimated. In addition, we did not consider reduced doses or treatment discontinuation. Effectiveness and cost on the basis of real-world data merit future research.
In conclusion, our analysis suggests that durvalumab after chemoradiotherapy in limited-stage SCLC is not a cost-effective strategy from the perspective of the Taiwanese health care sector. Reducing the price of durvalumab enhances the cost-effectiveness of the therapy. Thoracic oncologists and health policymakers should consider the study’s results when treating patients and reimbursing the drug.
CRediT authorship contribution statement
Sheng-Han Tsai: Data curation, Formal analysis, Investigation, Roles/writing—original draft, Writing—review and editing.
Jui-Hung Tsai: Conceptualization, Data curation, Writing—review and editing.
Li-Jun Chen: Investigation, Visualization, Writing—review and editing.
Szu-Chun Yang: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Roles/writing—original draft, Writing—review and editing.
Disclosure
Dr. Yang reports receiving grants from the 10.13039/100020595National Science and Technology Council and 10.13039/501100004844National Cheng Kung University Hospital during this study. The remaining authors declare no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Cancer Society Global Cancer Facts & Figures. 5th ed. Altlanta, GA: American Cancer Societyhttps://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/global-cancer-facts-and-figures/global-cancer-facts-and-figures-2024.pdf 2024
- 2Byers L.A.Rudin C.M.Small cell lung cancer: where do we go from here?Cancer 12120156646722533639810.1002/cncr.29098 PMC 5497465 · doi ↗ · pubmed ↗
- 3Koinis F.Kotsakis A.Georgoulias V.Small cell lung cancer (SCLC): no treatment advances in recent years Transl Lung Cancer Res 5201639502695849210.3978/j.issn.2218-6751.2016.01.03PMC 4758968 · doi ↗ · pubmed ↗
- 4Cheng Y.Spigel D.R.Cho B.C.Durvalumab after chemoradiotherapy in limited-stage small-cell lung cancer N Engl J Med 3912024131313273926885710.1056/NEJ Moa 2404873 · doi ↗ · pubmed ↗
- 5Ganti A.K.P.Loo Jr. B.W.Badiyan S.NCCN clinical practice guidelines in oncology: small cell lung cancer. Version 3https://www.nccn.org/guidelines/guidelines-detail?category=1&id=14622025
- 6U.S. Food & Drug Administration FDA approves durvalumab for limited-stage small cell lung cancerhttps://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-durvalumab-limited-stage-small-cell-lung-cancer
- 7Armeni P.Borsoi L.Fornaro G.Jommi C.Grossi F.Costa F.Cost-effectiveness and net monetary benefit of durvalumab consolidation therapy versus no consolidation therapy after chemoradiotherapy in stage III non-small cell lung cancer in the Italian National Health Service Clin Ther 4220208308473235449510.1016/j.clinthera.2020.03.012 · doi ↗ · pubmed ↗
- 8Chen X.Yang Z.Xiang G.Durvalumab consolidation therapy in patients with stage III non-small cell lung cancer after concurrent chemoradiation: a China-based cost-effectiveness analysis Expert Rev Pharmacoecon Outcomes Res 2220226476543464312910.1080/14737167.2022.1993062 · doi ↗ · pubmed ↗