Applying healthcare failure mode and effect analysis to enhance patient-controlled analgesia in acute post anesthesia pain management
Shaoru Chen, Hongmei Zhang, Hui Zhi, Jie Wang

TL;DR
This study shows that using a healthcare analysis method improves pain management and recovery after surgery.
Contribution
The novel application of HFMEA to optimize patient-controlled analgesia in post-anesthesia pain management.
Findings
HFMEA implementation reduced risk priority numbers and pain scores significantly.
Patients had shorter PACU stays after adopting the HFMEA-optimized process.
The optimized process improved pain control and recovery speed post-anesthesia.
Abstract
This study aimed to evaluate the application of Healthcare Failure Mode and Effect Analysis (HFMEA) to optimize the patient-controlled analgesia management process for patients experiencing acute pain after general anesthesia. In this retrospective study, the experimental group included 475 patients who underwent general anesthesia between July and December 2024, whereas the control group included 503 patients between January and June 2024. The experimental group received an HFMEA-optimized analgesia management process, whereas the control group received the standard nursing protocol. Patients’ pain scores, post-anesthesia care unit (PACU) stay length, and risk priority number (RPN) values were compared before and after HFMEA implementation. Following implementation, RPN values decreased from high to low risk, pain scores dropped significantly, and PACU stay was shortened (p < 0.05).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
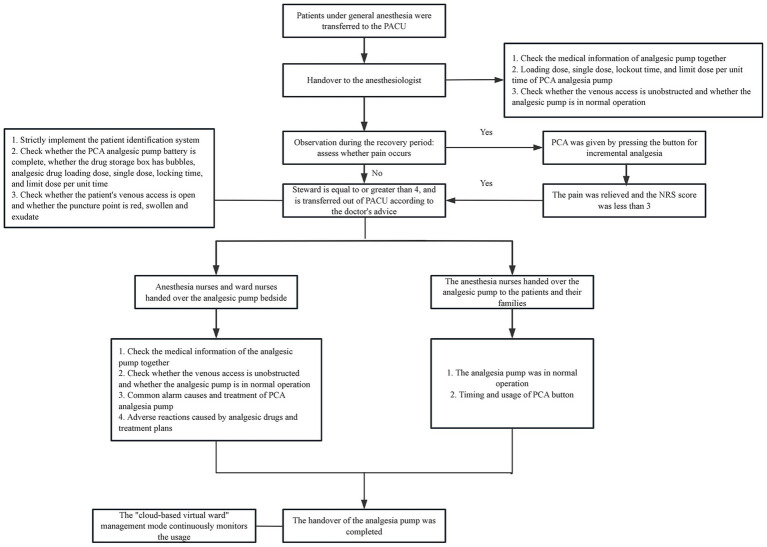 Figure 1
Figure 1| Item | Control group ( | Intervention group ( | t |
| |
|---|---|---|---|---|---|
| Gender | Male | 279 (0.55) | 272 (0.57) | 0.320 | 0.571 |
| Female | 224 (0.45) | 203 (0.43) | |||
| Age (years) | 48.14 ± 18.90 | 46.53 ± 19.52 | 1.313 | 0.189 | |
| ASA | III | 62 (0.12) | 68 (0.14) | 0.839 | 0.360 |
| IV | 441 (0.88) | 407 (0.86) | |||
| Level | NRS score | Score |
|---|---|---|
| Extremely serious | NRS:9 ~ 10 | 4 |
| Severe | NRS:7 ~ 8 | 3 |
| Moderate | NRS:4 ~ 6 | 2 |
| Mild | NRS:1 ~ 3 | 1 |
| Level | Standard of scoring | Score |
|---|---|---|
| Frequent | It often occurs or occurs for a short period of time | 4 |
| Occasional | May occur (several times within 1 to 2 years) | 3 |
| Uncommon | May occur (have occurred within 2 to 5 years) | 2 |
| Remote | Hardly ever (once in 5 to 30 years) | 1 |
| Severity occurrence | Extremely serious (4) | Severe (3) | Moderate (2) | Mild (1) |
|---|---|---|---|---|
| Frequent (4) | 16 | 12 | 8 | 4 |
| Occasional (3) | 12 | 9 | 6 | 3 |
| Uncommon (2) | 8 | 6 | 4 | 2 |
| Remote (1) | 4 | 3 | 2 | 1 |
| Process steps | Failure mode | Potential causes of failure | Hazard score | Decision tree analysis | |||||
|---|---|---|---|---|---|---|---|---|---|
| S | O | RPN | Single point weakness | Existing control measure | Detectable | Proceed | |||
| Patients under general anesthesia were transferred to PACU | Patient-controlled analgesia pump information was not checked before patients left the operating room | The verification process of analgesic pump needs to be standardized | 3 | 3 | 9 | → | N | N | Y |
| Handover with the anesthesiologist | The delivery of analgesia pump was not standardized (such as no label, wrong writing of label information, inconsistent parameter Settings and label information) | Some doctors and nurses were not familiar with the parameter setting and adjustment of analgesic pump | 3 | 3 | 9 | → | N | N | Y |
| The condition was observed during the recovery period | The pain was not treated in time after the patient woke up | Some doctors and nurses used pain assessment tools incorrectly | 4 | 3 | 12 | → | N | N | Y |
| Steward ≥4 was transferred out of PACU following medical advice | The patient-controlled analgesia pump was not checked again by the anesthesia nurse before the patient left the PACU | Some doctors and nurses were not familiar with the verification process of analgesic pump | 3 | 3 | 9 | → | N | N | Y |
| Transfer to ward | Patient-controlled analgesia training and health education were not in place | 1. Ward nurses were not familiar with the alarm handling of patient-controlled analgesia pump | 4 | 2 | 8 | → | N | N | Y |
| 2. Incorrect timing and usage of patient-controlled keys | |||||||||
| Process | Measures for improvement |
|---|---|
| Patients under general anesthesia were transferred to PACU | Patient information, connection and usage parameters of patient-controlled analgesia pump were checked before transport |
| Handover with the anesthesiologist | 1. Medical staff should be trained on the use of analgesic pump through on-site demonstration and lecture. |
| The condition was observed during the recovery period | 1. Training patients on pain scoring, and correctly using the corresponding scoring tools for different groups |
| Steward ≥4 was transferred out of PACU following medical advice | 1. The anesthesia nurse should implement the patient identification system again before the patient leaves the PACU |
| Transfer to ward | 1. Carry out analgesic pump use courses for ward nurses |
| Group | Patient-controlled analgesia pump information was not checked before patients left the operating room | The handover of analgesia pump was not standardized | The pain was not treated in time after the patient woke up | The patient-controlled analgesia pump was not checked again by the anesthesia nurse before the patient left the PACU | Patient-controlled analgesia training and health education were not in place | (x̅ ± |
|---|---|---|---|---|---|---|
| Before HFMEA | 9 | 9 | 12 | 9 | 8 | 9.40 ± 1.52 |
| After HFMEA | 6 | 4 | 6 | 4 | 6 | 5.20 ± 1.10 |
|
| 5.020 | |||||
|
| <0.05 |
| Group |
| NRS | PACU stay time (h) | |
|---|---|---|---|---|
| Before treatment | After treatment | |||
| Before HFMEA | 503 | 7.14 ± 1.71 | 1.04 ± 0.21 | 2.83 ± 0.37 |
| After HFMEA | 475 | 4.36 ± 0.64 | 1.08 ± 2.09 | 2.01 ± 0.21 |
|
| 33.953 | −2.411 | 42.544 | |
|
| <0.05 | 0.016 | <0.05 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNausea and vomiting management · Pain Management and Opioid Use · Anesthesia and Pain Management
Introduction
1
Patient-controlled analgesia (PCA) is a therapeutic method in which clinicians preprogram analgesic doses based on the patient’s physiologic condition and pain intensity, enabling the patient to self-administer medication for pain relief. PCA reduces perioperative pain, thereby suppressing the stress and inflammatory responses induced by surgical trauma (1, 2). PCA is easy to use, provides effective analgesia, and accelerates patient recuperation after surgery. It is a crucial tool in postoperative pain management (3). The Chinese Society of Anesthesiology’s 2024 “Expert consensus on the Clinical Application of Patient-Controlled Analgesia” noted that PCA should adhere to the “on-demand analgesia” principle and be tailored to patient-specific needs across clinical contexts and time points. The efficacy and safety of PCA are compromised by several factors, including insufficient clinical awareness among medical staff, ambiguous role delineation, ineffective doctor-patient communication, and the absence of standardized management and quality assessment protocols (3).
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) formally recognizes healthcare failure mode and effect analysis (HFMEA). This methodology prospectively optimizes and verifies risk procedures in medical processes, thereby reducing adverse events within the medical quality management model (4, 5). The basic process consists of six steps: identifying the theme, assembling the team, developing the process, analyzing the risks, creating an action plan, and assessing the outcome. This procedure involves conducting a prospective quantitative analysis of potential process failures, identifying their underlying causes, and implementing targeted improvements to systematically prevent these failures and reduce the frequency of medical risks (6). It plays a role in pain management (7), emergency nursing (8), post-anesthesia care unit (PACU) quality management (9, 10), and operating room nursing (11). However, reports on the application of the HFMEA model to patient-controlled analgesia for acute pain following general anesthesia remain scarce. As patients often have a limited understanding of PCA, clinicians must provide comprehensive assessments, clear instructions, and diligent supervision to ensure effective postoperative pain relief (3).
In this study, the HFMEA model was used to evaluate the failure modes and influencing factors across each link of the PCA management plan for patients with acute pain after general anesthesia, analyze the key links, formulate an optimized PCA management plan, and accelerate the perioperative surgical recovery of patients.
Materials and methods
2
Inclusion and exclusion criteria
2.1
The experimental group comprised 475 patients who received general anesthesia in the PACU between July and December 2024, whereas the control group included 503 patients who received general anesthesia in the same setting between January and June 2024. This study had a retrospective cohort design. This study adhered to the provisions of the Helsinki Declaration, safeguarded the privacy of the participants.
The inclusion criteria were as follows: (i) intubated patients transferred to the PACU after general anesthesia, (ii) American Society of Anesthesiologists (ASA) grade III-IV, (iii) Numerical Rating Scale (NRS) > 3, and (iv) no adverse events before or during the operation.
The exclusion criteria were as follows: (i) severe cardiopulmonary or cerebral disease not transferred to the PACU, and (ii) preoperative assessment of dementia, cognitive impairment, or inability to communicate effectively. There were no significant differences in age, sex, department, or ASA grade between the two groups (p > 0.05), as shown in Table 1.
Healthcare failure mode and effect analysis (HFMEA)
2.2
The first step was to determine the research theme: “Effect evaluation of optimizing PCA management process for patients with acute pain after general anesthesia based on HFMEA”.
Step 2: set up the HFMEA team
2.2.1
One anesthesiologist, one head nurse, five nursing team leaders in the recovery room, and one pain management nurse were among the physicians and nurses who collaborated to form the HFMEA team. All had a bachelor’s degree or higher, and there were six intermediate titles, one senior title, and one associate senior title. Following the team’s formation, members completed a systematic study of the HFMEA model and the research issues through both online and offline theoretical teaching techniques. After completing the test, they were able to understand the HFMEA research procedures and safety measures before beginning the actual operation process. The team held sporadic quality control meetings, conducted frequent business conversations, and set up an online communication group.
Step 3: draw the flow chart of patient-controlled analgesia management for patients with acute pain after general anesthesia
2.2.2
Through field tracking, brainstorming, literature analysis, and clinical practice experience, the HFMEA team members examined the postoperative PCA process for patients under general anesthesia in the PACU. The sub-process under the main process was improved, and steps requiring optimization were identified based on the timing and workflow. Five steps were identified and included in the flow chart of PCA management for patients experiencing acute pain following general anesthesia: patients were transferred to the PACU, anesthesiologists were consulted, patients’ conditions were monitored during the recovery period, patients with a Steward score ≥ 4 were moved out of the PACU per the doctor’s orders, and the patients were transferred to the ward.
Step 4: identify the potential failure modes, conduct risk analysis, and calculate the risk priority index
2.2.3
From the sub-processes, potential failure modes, failure causes, and potential effects, the HFMEA project team used brainstorming, literature analysis, and expert group meetings to examine the six processes in managing a PCA pump for patients experiencing acute pain following general anesthesia, supplemented by clinical experience. The failure risk priority number (RPN) was determined, which is essential when applying the HFMEA paradigm for continuous quality management. The determinants of RPN are Occurrence (O) and severity (S) (12). Failure severity was graded into four categories using the clinical medical risk severity grading standard: extremely serious, severe, moderate, and mild. These categories received scores of four, three, two, and one points, respectively, with higher scores indicating greater severity (Table 2). Each of the four grades—frequent, occasional, infrequent, and rare— was given 4, 3, 2, and 1 points, respectively, in accordance with the Australian Clinical Medical Risk Likelihood Assessment Grading standard model; higher scores indicated greater failure probability (Table 3). With a total score ranging from 1 to 16, the RPN = S × O. A higher RPN score indicated a higher risk value, indicating a latent hazard of the process (Table 4). To identify key failure modes, decision tree analysis was used to examine the failure modes with high RPN scores (RPN ≥ 8) and failure modes with high damage severity (RPN < 8) (4, 13) (Table 5).
Step 5: develop and implement improvement measures
2.2.4
After multidisciplinary discussions, the HFMEA project team identified six major failure modes through decision tree analysis, examined and categorized the possible causes of failure, and developed improvement strategies. Optimization details are provided in Table 6. To assist the medical staff in the PACU in accurately implementing pertinent measures, a clear and refined verification flowchart for PCA in patients with acute pain following general anesthesia was constructed based on the optimized content as illustrated in Figure 1. To optimize the entire process, the team established task divisions, coordinated the work of physicians and nurses, delivered scheduled training and supervision, promptly communicated and coordinated existing details online, and held group quality control meetings.
Flow chart of patient-controlled analgesia management for patients with acute pain after general anesthesia. (i) Power alarm: this alerts nurses to connect the power or replace the battery when the power is off or the battery display is too low. (ii) The alarm is activated and the obstruction’s cause is addressed when the infusion pipeline or the catheter’s front end becomes blocked or broken. (iii) Air alarm When air bubbles form in the infusion pipeline, they should be released to avoid the bubbles getting into the body and raising concerns. (iv) The analgesic pump is promptly removed and placed in the “analgesic pump recycling box” in the treatment room when the alarm at the conclusion of the infusion is triggered.
Step 6: observation index
2.2.5
(i) Evaluation of the RPN value for PCA pump management before and after HFMEA deployment in patients experiencing acute pain following general anesthesia. (ii) Patient pain rating. (iii) Time spent in the PACU before and after the improvement measures were implemented.
Statistical analysis
2.3
Data entry was performed using excel, and statistical analyses were performed using SPSS version 25.0. The mean ± standard deviation was used to describe measurement data that fit a normal distribution, whereas the frequency and constituent ratios were used to describe count data. Continuous normal variables were tested using the two independent sample t test, whereas categorical variables were tested using the χ^2^ test. Statistical significance was set at p < 0.05.
Results
3
Comparison of RPN values of PCA in patients with acute pain after general anesthesia before and after HFMEA
3.1
The project team reassessed the risk value of the PCA pump management process six months after HFMEA management was introduced into the PCA management process for patients experiencing acute pain following general anesthesia. As indicated in Table 7, the risk value was significantly lower than before the adoption of HFMEA (p < 0.05).
The pain scores and PACU length of stay were compared before and after HFMEA
3.2
The project team reassessed the pain incidence and PACU retention time of the PCA pump management process six months after HFMEA management was introduced into the PCA management process for patients experiencing acute pain following general anesthesia. As indicated in Table 8, the risk value was significantly lower than before the adoption of HFMEA (p < 0.05).
Discussion
4
The application of HFMEA model in risk assessment of PCA management process for patients with acute pain after general anesthesia can optimize the management process and reduce the management risk
4.1
The HFMEA management approach enhances nursing quality and aids in the development of medical management processes. To achieve standardized management and improvement of the evaluation index, HFMEA can prospectively evaluate the project process, effectively highlight weaknesses in the medical care process management, precisely identify failure modes and causes, create action plans, and clearly reflect the evaluation index of the project’s improvement effect (14). The five primary processes of PCA management for patients experiencing acute pain following general anesthesia were identified in this study: transferring patients under general anesthesia to the PACU, handoff to anesthesiologists, monitoring the patients’ condition during the recovery phase, transferring patients with a Steward score ≥ 4 out of the PACU in accordance with the doctor’s orders, and transferring to the ward. The potential risk factors were analyzed and refined to create focused improvement strategies and streamline procedures. The findings demonstrated that the risk values of the failure modes in every stage of the PCA management process for patients experiencing acute pain following general anesthesia significantly decreased following the implementation of HFMEA management, and the differences were statistically significant (p < 0.05). This demonstrates that the HFMEA-based PCA management procedure for patients experiencing acute pain following general anesthesia can lower the risk of multiple factors during the procedure, enhance overall process safety, and show viability and efficacy. To prevent postoperative patient-controlled anesthetic oversedation events, Cronrath et al. (15) used the HFMEA model to manage complex processes. The predetermined HFMEA goal—a 50% decrease in oversedation events—was accomplished after a year. In the study, Sun et al. (11) verified that the use of the HFMEA model in sputum specimen management can enhance specimen quality and the rate of positive detection. Zhao’s research, which utilized HFMEA approach to manage postoperative diabetes insipidus in pediatric neurosurgery, helped optimize the management process, alleviate postoperative symptoms of diabetes insipidus, and improve the prognosis (16).
The application of HFMEA model to optimize the PCA management process of patients with acute pain after general anesthesia can improve the effect of pain management, reduce the incidence of pain, and the length of PACU stay
4.2
The HFMEA is a crucial instrument for diagnosing health systems and a potent tool for enhancing professional health learners’ knowledge and capacity for quality improvement (17). In this study, pain scores and PACU length of stay were significantly lower after the implementation of HFMEA, and the differences were statistically significant (p < 0.05) after the HFMEA model was used to optimize the PCA management process for patients with acute pain following general anesthesia. Healthcare organizations should conduct prospective risk analyses in high-risk processes at least once a year according to JCAHO. The requirements for high-risk processes are as follows: an internal unusual event report suggests that the event is frequent or of high severity; a sentinel event shows that the event poses a risk to patient safety; an external source indicates that the event is frequent or of high severity; or a new system or procedure is required (18). An examination of the literature revealed that acute pain following general anesthesia is common and, if left untreated, can adversely affect patients (19). Thus, the PCA management procedure for patients experiencing acute pain following general anesthesia was optimized, and the frequency of associated adverse events decreased in accordance with the expert consensus on PCA management (2). Sun et al. (4) used the HFMEA model. To improve medication safety management, a multidisciplinary team evaluated the risk of intrathecal morphine pump use and prioritized steps to lower this risk. This allowed nursing managers to shift safety events associated with intrathecal morphine pump administration from negative treatment to positive prevention prior to the event. It guarantees nursing safety and represents an ongoing enhancement of nursing quality.
In conclusion, as a quality management methodology, HFMEA uses prospective analysis to identify emerging issues, enable preventive action before issues arise, and prevent adverse events by addressing root causes. One limitation of this study is its retrospective design relying on historical data, which may affect the accuracy of outcome analyses. Prospective cohort studies will be conducted to optimize future designs. This study examined causes of PCA failure in the anesthesia and perioperative medicine departments and aimed to improve the PCA procedure to greatly enhance patient pain management and reduce the duration of PACU stay. As a result, applying HFMEA to the PCA management process for acute pain following general anesthesia can proactively control failure modes and guarantee patient safety, supporting broader clinical adoption.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hicks CM Dyck MA Martin L Guthrie DM Stewart SL Hirdes JP. Patient-controlled analgesia for managing pain in adults receiving palliative care: a scoping review. Pain Manag Nurs. (2025) 26:361–374. doi: 10.1016/j.pmn.2025.02.01440155305 · doi ↗ · pubmed ↗
- 2She S Yu W Huang Y Yao S Yu B Liao C. Expert consensus on clinical application of patient-controlled analgesia. Chin J Pain. (2024) 20:509–526. doi: 10.3760/cma.j.cn 101658-20240323-00036 · doi ↗
- 3Zhang J Cai Y Zheng K Chen M Liu X Wu Y. A systematic review of guidelines for patient-controlled analgesia management in patients with acute postoperative pain. Chin J Nurs. (2021) 56:1868–1875. doi: 10.3761/j.issn.0254-1769.2021.12.018 · doi ↗
- 4Sun L Fang M Xu T Liu M Fang S Feng W. Application of healthcare failure mode and effect analysis in the Management of Patients with Intrathecal Morphine Pump Implantation. Pain Manag Nurs. (2024) 26:e 207–4. doi: 10.1016/j.pmn.2024.10.019, PMID: 39613668 · doi ↗ · pubmed ↗
- 5Li N Xiong X Cheng Q Tu P Li L. Application progress of healthcare failure mode and effect analysis in standardizing nursing workflow. Nurs J. (2023) 30:36–40. doi: 10.16460/j.issn 1008-9969.2023.11.036 · doi ↗
- 6Chen H Zhang C Wu B Zou K Pei Y. Application of healthcare failure mode and effect analysis in risk management of intraoperative acquired pressure injury. Chin Nurs Manag. (2022) 22:713–717. doi: 10.3969/j.issn.1672-1756.2022.05.015 · doi ↗
- 7Ni Y Feng Y Huang Y Zhang R. Application of intelligent specimen submission combined with HFMEA model in improving satisfaction and management quality indicators in the pathology specimen submission process in the operating room. Minerva Surg. (2024) 79:1–3. doi: 10.23736/S 2724-5691.24.10634-X, PMID: 39535819 · doi ↗ · pubmed ↗
- 8Chia J-S Chang C Lo S-C Yang C-H Yang H-Y. Healthcare failure mode and effect analysis combined service blueprint—mitigating mass casualty triage in emergency units: a qualitative study. Int Emerg Nurs. (2024) 77:1–9. doi: 10.1016/j.ienj.2024.101508, PMID: 39236663 · doi ↗ · pubmed ↗