The health-promoting experiences of storytellers in group-based digital storytelling workshops: a meta-synthesis of qualitative studies
Jonathan Dominguez Hernandez, Bernadette Irene Brieskorn, Vanessa Leutenegger, Astrid Krahl, Rachael Eastham, Mark Limmer

TL;DR
Digital storytelling workshops help people reframe their health experiences, leading to positive changes in their attitudes and behaviors.
Contribution
This study is the first meta-synthesis to explore how digital storytelling impacts health through narrative re-framing and emotional engagement.
Findings
Digital storytelling workshops create a safe space for participants to reframe their health narratives.
The re-storying process increases storytellers' sense of agency and control over their health experiences.
Participants are motivated to use their stories to support others after engaging in digital storytelling.
Abstract
To synthesize qualitative evidence, using the framework analysis method, on how participating in a digital storytelling workshop shapes the storytellers’ health attitudes, values, beliefs, or behaviors. We conducted a meta-synthesis using the framework analysis method to generate analytic themes. We searched Medline, CINHAL, SocIndex, Embase, PsycINFO, SciELO, Academic Search Ultimate, Scopus, the Directory of Open Access Journals, and LIVIVO. We used the GRADE-CERQual approach to assess the confidence in the review findings. We included 25 qualitative studies from six countries representing the experiences of 629 storytellers. Confidence in most review findings was moderate. Storytellers experience digital storytelling workshops as a safe space where they reframe the narratives around their health experiences. This re-storying process extends storytellers’ understanding of their…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
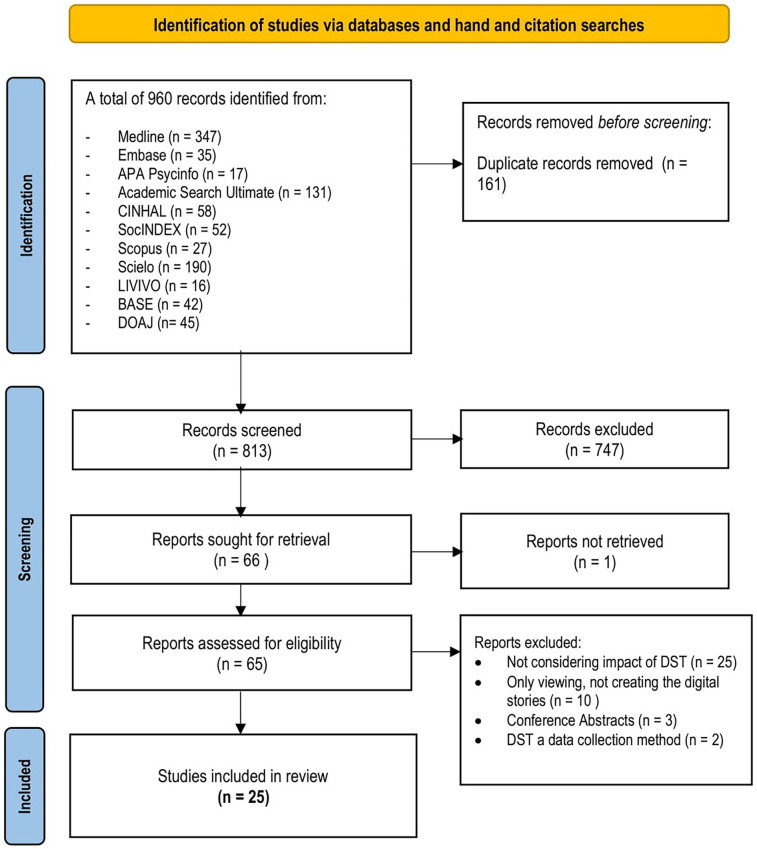 Figure 1
Figure 1| SPIDER | Inclusion criteria | Exclusion criteria | Rationale |
|---|---|---|---|
| Sample | All populations, including pediatric populations | N/A | Digital storytelling is accessible to all populations with the ability to write, read, and use a computer. This can include the majority of the pediatric population. Digital storytelling is a facilitated process that can be adapted to all populations. In addition, digital storytelling experiences are unique for the storytellers. Including a wider population can provide a more general understanding of various health-promoting experiences. |
| Phenomenon of interest | The health-promoting potential of digital storytelling on the storyteller in a health context | Digital storytelling outside the health context | Digital storytelling has been widely used as a pedagogical approach in education and as an instrument for persuasion in marketing. It was essential to differentiate these studies from those addressing health issues. |
| Design | Interviews, focus groups, observations, case studies or action research | Surveys, online surveys | Measuring lived experience with an instrument remains a challenge. Researchers who have employed standard instruments to measure experiences of digital storytelling participation have not found evidence of an effect ( |
| Evaluation | Health attitudes, values, beliefs, behaviors | N/A | Research evidence indicates that digital storytelling can lead to storytellers replacing their health narratives with health-promoting attitudes, values, beliefs or behaviors ( |
| Research type | Qualitative or the qualitative components of mixed-method studies | Observational (Cross-sectional, etc.) experimental and quasi-experimental studies | To ensure a comprehensive representation of the available qualitative evidence. In addition, it provides richer and more in-depth data on the storytellers’ experiences. |
| Language | The search strategy was developed in English, German, and Spanish, but no language restrictions were applied during the search or screening process. | N/A | Based on the principal reviewer's language competence. The titles and abstracts of articles in other languages were translated using artificial intelligence through DeepL (translator function). |
| Type of publication | Primary research, including published peer-reviewed and grey literature (such as dissertations or other type of reports of primary qualitative research) | Non-primary research such as editorials, letters to the editor, reviews, case reports, and case series | Primary qualitative research offers rich and in-depth data, and grey literature (such as dissertations and reports) can contribute to more diverse viewpoints and nuances. |
| Author(s), Year | Country | Population | Sample size | Context/Setting | Aim(s) or research question(s) | Philosophical/Theoretical underpinnings | Study design | Digital storytelling approach | Data collection | Analytic process | Reflexivity |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Beltrán and Begun 2014 ( | New Zealand | Māori community (20–45 years) | University Campus | To facilitate dialogue and use digital storytelling to interrupt contemporary challenges often faced by Indigenous communities | Historical trauma theory | Community-based participatory inquiry | StoryCenter | In-depth qualitative interviews | Thematic analysis | Yes | |
| Boydell et al. 2018 ( | Canada | Young people (16–23 years) with the first episode of psychosis | Early intervention clinic rural community | To produce individual digital stories describing how to manage psychosis in everyday life | The social world “does not consist of separate things. but of relationships.” | Community-based participatory inquiry | StoryCenter | Participant observation informal interviewing and reflexive field notes | Not described | No | |
| Briant et al. 2016 ( | USA | Working-class Hispanics of Mexican origin | Cancer Research Center | To explore if digital storytelling could be a culturally relevant tool for Hispanics/ Latinos of Mexican origin to share their experiences with cancer or other diseases. | Transportation theory | Community-based participatory action research and a narrative framework | Creative Narrations digital storytelling | Semi-structured face-to-face interviews | Thematic analysis | No | |
| De Vecchi et al. 2017 ( | Australia | Mental health consumers and clinicians | Rural psychiatric service | To explore participation in digital storytelling and investigate the potential of digital storytelling as a research method. | Interpretative paradigm | Instrumental Case study and process evaluation | StoryCenter | Semi-structured Interviews | Not described | No | |
| DiFulvio et al. 2016 ( | USA | Puerto Rican Latinas (15–21 years) | New England City | To assess the effectiveness of the digital storytelling process in creating positive changes in participants’ sexual attitudes or values, self-esteem, social support, and empowerment (including self-efficacy, sense of hope for the future, and community activism). | Not reported | Mixed-methods | StoryCenter | Qualitative part: Open Ended questions | Not reported | No | |
| Dixon and Isaac 2023 ( | USA | Black African-American women, cisgender, queer, and middle-class, public health doctoral students | Weekly Zoom meetings | To explore how the intersection of racism, sexism, and socio-cultural expectations shape BFRB experiences. | Critical Narrative Archaeology of Self (AOS) | Autoethnography | StoryCenter | Digital storytelling process and online discussions | Content analysis | Yes | |
| Ferrari et al. 2015 ( | Canada | Persons of African, Caribbean, and European descent | Toronto, Ontario, | To examine how the process of making their digital stories can be “therapeutic” or “cathartic. | Not reported | Not reported | StoryCenter | workshop evaluation and 11 of them a survey | Thematic analysis | No | |
| Fiddian-Green et al. 2017 ( | USA | Puerto Rican Latinas (15–21 years) | New England City | To examine and delineate salient cultural paradigms of sexuality. | Constructivist grounded theory | Case-Study | StoryCenter | Semi structured interviews | Content, discourse analysis | No | |
| Goodman 2019 ( | Canada | Drug users (25–45 years) | Drug recovery clinic | To help transform widespread assumptions and prejudices about long-term heroin users | Not reported | Not described. | StoryCenter | Interviews | Descriptive, digital stories | Yes | |
| Gubrium et al. 2016 ( | USA | Puerto Rican Latinas (15–21 years) | New England City | To know if the digital storytelling process affected a participant's self-esteem, sense of empowerment, social support, or sexual attitudes or behaviors. | Constructivist grounded theory | Mixed-methods | StoryCenter | Story transcripts, Field notes, observation, follow-up semi-structured interviews | Using code matrix and three node structure | Yes | |
| Gubrium et al. 2019 ( | USA | Puerto Rican Latinas (15–21 years) | Offices of a community-based organization | To collaboratively interrogate and address experiences of interpersonal and structural violence and embodied trauma. | Critical Narrative | Digital storytelling as a research method | StoryCenter | Digital storytelling, field notes and follow-up interviews | Intertextual transcription method, content analysis, contextual analysis | Yes | |
| Howard et al. 2023 ( | Canada | People with endometriosis | Online workshops via Zoom. | To assess the feasibility of story co-creation and sharing. | Not reported. | Qualitative methods | StoryCenter | Reflective journals | Qualitative interpretive description | Yes | |
| Jun et al. 2022 ( | USA | Nurses from a not-for-profit public-health organization | Workshops offered within the nursing organization | To evaluate the first-person experiences of attending in-person digital storytelling workshops. | Not reported | Descriptive qualitative method | StoryCenter | Semi-structured phone interviews | Thematic analysis | Yes | |
| Kim et al. 2021 ( | USA | Adults (18 or older) who received a hematopoietic cell transplant | Not known | To explore experiences of participating in a 3-day digital storytelling workshop | Narrative theoretical model/social cognitive theory/constructivist grounded theory | Descriptive qualitative method | StoryCenter | Workshop evaluation questionnaire | Content analysis | No | |
| Kim et al. 2023 ( | USA | Vietnamese or Korean American women (18 or older) | Virtual digital storytelling via Zoom | To assess feasibility, acceptability and in-depth analysis of the mother's cultural experience of HPV | Constructivist grounded theory | Mixed methods | StoryCenter | Questionnaire, field notes, web-bsed workshop activtivities | Thematic analysis | No | |
| Laing et al. 2017 ( | Canada | Children and young adults cancer survivors (5–19 years) | Childreńs hospital | To determine how digital stories might be effective therapeutic tools | Hermeneutics | Not reported | StoryCenter | Semi-structured interviews | Hermeneutic | No | |
| Laing et al. 2019 ( | Canada | Adult (18 or older) patients with cancer | Outpatient cancer treatment center | To discover how the creation of a digital story affects adult patients with cancer | Hermeneutics | Qualitative, interpretive methodology | Two-hour sessions with assistant trained in digital storytelling | Semi structured interviews face to face and telephone | Hermeneutics | No | |
| Lamarre & Rice 2016 ( | Canada | Young Women with Eating Disorder Recovery | Not described | To illustrate the possibilities of a guided practice of digital storytelling for critical arts-informed research processes | Critical feminism/theoretical frame (post-structuralist) | Narrative | StoryCenter | Digital stories | Visual analysis | No | |
| Lenette & Boddy 2013 ( | Australia | Women with refugee backgrounds | Not reported | To explore women's experiences of being a refugee | Feminism | Visual ethnography | Not described. | Photovoice, Photo-eliciting and digital storytelling, in-depth interviews | Visual ethnography | No | |
| Martin et al. 2019 ( | Canada | Young women exposed to dating violence | University campus | To explore the impact of learning digital storytelling skills to promote change and interrupt the cycle of abuse. | Feminist, qualitative, and arts-based research | Digital storytelling as a research method | StoryCenter | Focus group | Not described | No | |
| Njeru et al. 2015 ( | USA | Somali and Spanish-speaking patients with type II diabetes | Healthy Community Partnership centre | To develop a diabetes digital storytelling intervention with and for immigrant and refugee populations. | Social Cognitive Theory, Narrative Theory, and social construction theory | Digital storytelling as a research method | StoryCenter | Digital Stories | Not described | No | |
| Nyirenda et al. 2022 ( | Malawi | Residents from Bangwe and Ndirande | Bangwe and Ndirande, Malawi | To assess if digital storytelling could be used to explore community perspectives on health concerns. | Gaventa's theories of power and participation | Digital storytelling as a research method | Similar to the StoryCenter approach | Digital Stories | Not described | No | |
| Paterno et al. 2018 ( | USA | Peer mentors in recovery from SUD | Community site in a rural county in New England | To assess the feasibility of using digital storytelling with peer mentors. | Not described | Digital storytelling as a research method | StoryCenter | In-depth, semi structured follow-up interviews | Thematic analysis | No | |
| Wexler et al. 2013 ( | USA | Young people from 12 rural villages in Northwest Alaska | Rural sparse populated areas of Alaska | To use digital storytelling as a health promotion strategy within a PYD approach. | Freirian Model | Mixed-methods | StoryCenter | Interviews after workshop | Coding but not further description | No | |
| Willis et al. 2014 ( | Zimbabwe | Young people with HIV (8-22 years) | Africaid's Zvandiri program | To evaluate the digital storytelling process as a therapeutic approach | Social constructionism | Qualitative methods | StoryCenter | Focus groups digital stories, field notes, | Thematic analysis | No |
| Author(s), Year | CASP tool questions | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | |
| Beltrán and Begun 2014 ( | Yes | Yes | Yes | No | Yes | Yes | Can't tell | Can't tell | Yes |
| Boydell et al. 2018 ( | No | Yes | Yes | Can't tell | Yes | No | No | Can't tell | No |
| Briant et al. 2016 ( | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes |
| De Vecchi et al. 2017 ( | Yes | Yes | Yes | No | Yes | Can't tell | Yes | Can't tell | Yes |
| DiFulvio et al. 2016 ( | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes |
| Dixon and Isaac 2023 ( | Yes | Yes | Yes | Can't tell | Can't tell | Yes | Can't tell | Yes | Yes |
| Ferrari et al. 2015 ( | No | Can't tell | Yes | Can't tell | Yes | No | No | Cańt tell | Yes |
| Fiddian-Green et al. 2017 ( | Yes | Yes | Yes | Yes | Yes | Can't tell | Yes | Yes | Yes |
| Goodman 2019 ( | No | Yes | Can't tell | Yes | Yes | Yes | Yes | No | Yes |
| Gubrium et al. 2016 ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Gubrium et al. 2019 ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Howard et al. 2023 ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Jun et al. 2022 ( | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Kim et al. 2021 ( | Yes | Yes | Yes | No | No | Can't tell | Yes | Yes | Yes |
| Kim et al. 2023 ( | Yes | Yes | Yes | Yes | Yes | Can't tell | Yes | Yes | Yes |
| Laing et al. 2017 ( | Yes | Yes | Yes | Yes | Yes | Can't tell | Yes | No | Yes |
| Laing et al. 2019 ( | Yes | Yes | Yes | Yes | Yes | Can't tell | Yes | Can't tell | Yes |
| Lamarre & Rice 2016 ( | Yes | Yes | Can't tell | Can't tell | Yes | Yes | No | Can't tell | Yes |
| Lenette & Boddy 2013 ( | No | Yes | Yes | Yes | Yes | Can't tell | Yes | Can't tell | Yes |
| Martin et al. 2019 ( | Can't tell | Yes | Yes | Can't tell | Yes | Can't tell | Yes | Yes | No |
| Njeru et al. 2015 ( | Yes | Yes | Yes | No | Yes | Can't tell | No | Can't tell | Yes |
| Nyirenda et al. 2022 ( | Yes | Yes | Yes | Yes | Can't tell | Can't tell | Yes | Can't tell | No |
| Paterno et al. 2018 ( | Yes | Yes | Yes | No | Yes | Can't tell | Yes | Can't tell | Yes |
| Wexler et al. 2013 ( | Yes | No | Yes | Yes | Yes | Can't tell | Yes | No | No |
| Willis et al. 2014 ( | Yes | Yes | Yes | No | Yes | Can't tell | Yes | Yes | No |
| Descriptive themes (Review Findings) | Studies contributing to the review finding | GRADE-CERQual Assessment of confidence | Example of Supporting data | Analytical theme |
|---|---|---|---|---|
| 11 Studies | Moderate confidence | “In the beginning, I was really, really anxious about it, but even halfway through the first session, that anxiety definitely decreased just at how welcoming and accepting and just how common it felt our experience was. We had this like connection that was beyond just Endo, having Endo. It was really great” ( | Re-storying lived experience | |
| 14 Studies | Moderate confidence | “It sort of forces you to reflect on things that maybe you don't sit down and do every day, right? It's not like you go, “Today I'm going to think about this.” This is kind of an opportunity that forces you into something like that. It made me think about things that maybe I didn't want to, or hadn't very much, you know?” ( | ||
| 16 Studies | Low confidence | “Life-changing stuff. You can see it. You can hear it in people's narratives. It's about talking through their story. You can hear the growth and the de-cluttering. Yeah, it's almost like watching a flower, like a peony rose… beautiful flowers…and it's just like watching them burst into life” ( | ||
| 7 Studies | Moderate confidence | “It was also nice to get so much support, because I don't know if I would've shared that story had I not had the environment being the way it was, because it was so safe, …it was kind of like a powwow, where we all came together and really understood where each other was coming from” ( | The ripple effect of digital storytelling | |
| 14 Studies | Moderate confidence | “I think it was great when everyone talked and supported each other. Number one, if you heard their story, you understood where they were coming from because you can actually feel it and connect to those who experienced the same thing” ( | ||
| 8 Studies | Moderate confidence | “It reminded me that I wasn't alone. Not only are there others who share my experiences, but [they] share my view of the experiences.” ( | ||
| 10 Studies | High confidence | “I was very moved by [name] story as so much of my own is captured in her words. Again, I felt a sense of connection and of a deep understanding from my fellow participants, which was really beautiful and made me want to think about how to connect further with these women or others who have Endo” ( | ||
| 8 Studies | Moderate confidence | “…I found it challenging because some of the stories were.. emotionally resonating..you felt for what people go through, what's behind that outer shell that you show to the world” ( | Investing and processing emotions | |
| 8 Studies | Moderate confidence | “I was surprised at how much emotional I was when I went over my real story. I never thought of once any of the feelings that I was having. This workshop opens me up to realize the value of talking and sharing emotions. Now I am sharing my emotions with my family” ( | ||
| 11 Studies | Moderate confidence | “I grew. I was liberated and at peace. I'm at peace with myself in a way that I've not been for…I don't know…probably forever…by getting [the story] out, because I harboured it for so long. That's not a healthy way to be. It really makes…well, talking about health and trauma… it is medicine. That's the best way I can say it” ( | ||
| 13 Studies | High confidence | “…I just think that when you look at someone who's like you—looks like you—and they tell a story that is similar to yours, and they've come through it and they are now putting voice to it, and now they're not hurting, it gives you hope. It gives you hope that, ‘Well, what if I put a voice to my story?” ( | Owning the Script | |
| 8 Studies | Moderate confidence | “I definitely want to take my story and show it to my iwi, my family, and I want to see if they would be interested in doing some work of this nature. I feel like I've been given something that will help me help someone in a very simple way…” ( |
- —ZHAW Zurich University of Applied Science
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDigital Storytelling and Education · Empathy and Medical Education · Literacy, Media, and Education
Introduction
A growing body of evidence indicates that digital storytelling as a participatory and community-based approach can provide storytellers with potential health-promoting benefits (1–4). During the digital storytelling process, six to eight individuals who share a common experience work together over three consecutive eight-hour sessions to co-create unique digital stories by sharing and discussing their lived experiences, personal beliefs, and values in response to specific life events (5–7). A trained facilitator guides the storytellers to express and explore their personal experiences in relation to the stories and feedback of fellow participants (5–7). The goal is for storytellers to review their narratives and select and combine music, images, and text with their voiceover to portray compelling stories, engage with the audience, and evoke emotional responses (8). This process results in three to five-minute visual digital narratives eliciting rich, affective, and nuanced insights into the storytellers’ lived experiences (9). The assumption is that as storytellers articulate their lived experiences in a digital story, they gain new insights that could empower them to adopt health-promoting behaviors, values, attitudes, or beliefs (6, 10, 11).
Three phases in the digital storytelling process could explain the mechanisms that drive these potential health-promoting benefits. The story construction phase, which includes writing the script and integrating images, video, and sound, has been found to afford storytellers increased control over their health experiences (12). The collaborative construction approach used during the so-called “story circle” phase, in which the storytellers share their stories with other participants (9), also appears to promote positivity in the group by reducing feelings of social isolation and increasing empathy (2). The final screening phase, where participants screen their stories and discuss their narratives and core elements (9), can also positively affect recipients’ cognition, affect, and health behavior, increase self-efficacy and social support, and positively impact physical and mental health (6, 11, 13). Reports indicate that given these potential benefits, digital storytelling can be used as a learning and capacity-building tool to raise awareness about health issues or to inform and support public health initiatives through advocacy and community empowerment (5, 7, 14). For example, researchers have successfully implemented digital storytelling in youth sexual health promotion (15), to foster dialogue and reduce power imbalances between mental health patients and clinicians (11) or to promote a greater sense of health and well-being in refugee women (16). Digital storytelling has also played a role in youth empowerment in diabetes prevention (17) and has been integrated into participatory efforts for food security and policy development (18). However, it has been argued that any benefits the storytellers may obtain are, at most, anecdotal, coincidental, and a fortunate by-product of the research process because digital storytelling applied in a research setting often has facilitators not trained as therapists, who primarily intend to explore a phenomenon of interest and not how the process influences health attitudes or behaviors (19).
Digital storytelling has previously been subject to review in academic research. However, there is still limited information on the potential health-promoting effects on storytellers because the reviews available did not primarily focus on their experiences (2, 19, 20), narrowed their search to a pediatric (20) or older adult population (21), or did not critically appraise the literature or follow a fully systematic process (3, 22, 23). Therefore, a qualitative evidence synthesis of primary research using an interpretative methodology can add to the current body of knowledge by explaining the potential health-promoting experiences of storytellers. Further, because digital storytelling has been used in diverse contexts, applying a meta-synthesis methodology can enable the integration of contextual nuances that might shape storytellers’ experiences.
Methods
Qualitative synthesis methodology
We used the meta-synthesis methodology coined by Stern and Harris (24) and refined by Wals and Downe (22) as an approach rooted in a hermeneutic paradigm that goes beyond the meta-aggregation of the data (23). This approach facilitated an interpretative or meaning-making analysis in generating descriptive themes through an iterative data synthesis process using a framework developed a priori. We initially identified each component of this framework and organized and integrated these components into analytic themes, capturing the health-promoting experiences of storytellers (25–27). The ENTREQ checklist items (28) guided our reporting of this meta-synthesis. In addition, some items of the PRISMA statement (29) including the study selection chart or the study characteristics table were used to achieve full transparency in reporting. We registered this meta-synthesis at the inception stage, and there were no deviations from the review protocol (PROSPERO; registration number CRD42023478062).
Theoretical framework
Salutogenesis was deemed a fitting theoretical framework because it departs from the premise that even in a situation of “illness,” individuals still possess healthy attributes within a continuum between health breakdown and full health (30, 31). We assumed that the digital storytelling process could reveal these healthy attributes and enhance storytellers' sense of coherence (SOC) through the expression and exploration of their personal experiences, fostering health-promoting attitudes, values, beliefs, or behaviors (5–7). Health promotion is this context was defined as the process of empowering people to, individually and collectively, increase control over their health and improve it (32).
Reflexive note
It was acknowledged from the outset that the reviewers’ experiences, values, and orientations would influence how meaning was derived from the data (33, 34). The principal reviewer had previous experiences participating in digital storytelling workshops and continuously reflected, critiqued, and evaluated his prior beliefs when synthesizing and interpreting the textual data. We consciously and deliberately looked for evidence that challenged these beliefs to avoid overemphasizing data aligned with pre-existing viewpoints. In addition, discussions with the other reviewers questioned how much the principal reviewer could have imposed meaning on the data items. None of the other reviewers had previously participated in a digital storytelling workshop, and as midwives and academics, this was their first contact with digital storytelling. We aimed to minimize the over-influence of the principal reviewer through this member reflection process and ensure the credibility of the findings (35).
Inclusion criteria
We included studies exploring the health-promoting experiences of storytellers participating in a digital storytelling workshop. We defined digital storytelling as a collaborative, participative, and group-based approach to co-create three- to five-minute digital stories portraying participants’ experiences of health. We considered studies for inclusion if they employed qualitative methods and included the qualitative components of mixed-methods studies. The inclusion criteria and their rationale are detailed in Table 1.
Data sources
We searched Medline (Ovid), CINHAL (Ebsco), SocIndex (Ebsco), Embase (Ovid), and PsycINFO (Ebsco) in November 2023. Additionally, a search in the SciELO, Academic Search Ultimate (Ebsco), Scopus, the Directory of Open Access Journals (DOAJ), and LIVIVO databases expanded the search for potential articles, particularly in Spanish, German, and the global south. The global reach of digital storytelling demanded the inclusion of articles in other languages. We also reviewed the lists of references from the included studies and retrieved grey literature using the Bielefeld Academic Search Engine (BASE).
Search strategy
The search strategy included Boolean and proximity operators, subject headings (MeSH), word searching (free text), and the use of spelling (truncation), syntax, line numbers, and publication-type filters to retrieve qualitative and mixed methods articles. We applied free-text terms to cover unavailable subject headings (36). We initially developed the search strategy in Medline (via Ovid) using keywords such as “digital” and “stories,” “storytelling,” “narratives,” “interviews,” or “qualitative” and adapted the search to fit other databases (see Supplementary Appendix A1). Search terms in English were then translated into German and Spanish, although the German terms proved unhelpful in retrieving articles (37).
Study screening
Two reviewers screened the retrieved articles independently. A third independent reviewer resolved disagreements arising during the stages of the screening process (38), including an initial title and abstract review guided by a screening tool, illustrating the inclusion criteria and assisting the reviewers with inclusion decisions. An initial piloting phase of this tool with twenty-five articles assisted reviewers in ascertaining its applicability and ability to maximize inter-rater reliability (39). All retrieved studies were exported after deduplication from Endnote to Covidence (40). We used the same screening process to screen the full-text articles of included studies.
Quality of included studies
We used the critical appraisal skills program (CASP) tool to evaluate the methodological rigor of the included studies (41). The principal reviewer independently assessed the quality of all included studies, and three reviewers performed the second independent assessment, each evaluating one-third of the included studies. Conflicts were resolved through consensus (42). We did not exclude any articles based on quality rating, but as a form of sensitivity analysis, we explored how removing the findings from weaker studies would influence the analytic themes (43).
Data extraction
We extracted data items such as the philosophical position, theoretical assumptions, research methods, contextual nuances, and findings. Using an adapted version of the Joanna Briggs Institute's (JBI) instrument (44), two reviewers piloted the tool with a purposive sample of two articles (45). The goal was to limit interpretation and selection errors (46). The principal reviewer independently extracted all data items from all included studies, and three reviewers independently extracted the data from one-third of the included studies.
Data synthesis
A framework analysis approach was used to synthesize the data. Two index papers of the best quality were selected to develop the initial framework. Two reviewers independently open-coded the findings using NVivo and created a matrix containing the initial codes and descriptive themes. We discussed each coded section to determine its significance and how it could answer the research question. Conflicts were resolved by returning to the index studies to agree on the most suitable theme. We entered the final themes into a spreadsheet to organize and map the data against this framework (see Supplementary Appendix A2). The initial framework was refined iteratively as new themes emerged from other studies. We created or allocated new themes to existing categories using the constant comparative approach. If a new theme emerged, we assigned a name (a metaphor) and compared it with those included in the initial framework (47). The quality of the included studies assisted reviewers in determining the emphasis of new emerging themes in contrast with those within the framework and their closeness to the theoretical framework. For instance, new themes from high-quality studies replaced or modified existing ones (see Supplementary Appendix A2).
After coding and mapping the data, we began interpretation, ensuring the original themes’ meaning was preserved (22). We used the framework to cluster metaphors and reach a consensus on the descriptive themes. Participant quotations for each review finding illustrate the final themes. We assessed the level of confidence in the review findings using the GRADE-CERQual approach, considering methodological limitations, coherence, that is, how well the data supported the review findings, their adequacy or the degree of richness and quantity of the data, and the relevance of the data concerning the specified context of the meta-synthesis (48). The assessments of these four components collectively contributed to a level of confidence ranging from high to very low (49) (see Supplementary Appendix A3). We defined a review finding as an analytical result that describes a phenomenon or an aspect of a phenomenon based on data from primary studies (50).
Results
The review identified 974 records from electronic databases and hand and citation searching. After removing 161 duplicates, the reviewers screened the titles and abstracts of 813 articles. This led to the final inclusion of 25 peer-reviewed qualitative and mixed-methods articles exploring storytellers’ experiences (Figure 1).
PRISMA flow diagram of the study selection process (Switzerland, 2024).
Studies characteristics
The included studies were conducted in the United States, Canada, Australia, New Zealand, Malawi and Zimbabwe. The sample sizes ranged from two participants to a sample of 342, making a total of 629 participants. Most studies used StoryCenter's (51) approach to digital storytelling or the approach of the Creative Narrations organization (52). A detailed description of the characteristics of the included studies can be found in Table 2.
Methodological rigor
There were some concerns with the overall methodological rigor of the included studies, with only three studies being rated as having no methodological weaknesses that would impact the transferability of the results (53–55). In this meta-synthesis, transferability refers to the extent to which study findings can be subjected to de-contextualization and abstraction to generalize the emerging themes to other situations (56). The biggest issue of concern was the lack of reflexivity, with 14 studies either poorly addressing or not reporting any aspects of personal, interpersonal, methodological, or contextual reflexivity. A detailed description of our assessments is presented in Table 3.
Synthesis output
This meta-synthesis generated 12 descriptive themes (review findings), of which nine were graded with moderate confidence, indicating that these review findings are likely a reasonable representation of the storytellers’ health-promoting experiences. Two themes were graded with high confidence and a single theme with low confidence, making them highly likely or possibly a reasonable representation of the storytellers’ experiences, respectively. From these descriptive themes, we derived four analytical themes:—“Re-Storying Lived Experience,” “The Ripple Effect Of Digital Storytelling,” “Investing And Processing Emotions,” And “Owning The Script.” The final framework and its associated CERQual gradings are presented in Table 4.
Re-storying lived experience
Participation in a digital storytelling workshop prompts storytellers to alter, reshape, or even replace their narratives concerning their lived experiences of health with new or more positive ones. We assumed the distinction between stories, the specific tales shared about their experiences, and narratives, the broader contextual or social resources storytellers draw upon to construct their stories (57). Storytellers reconsider their experiences as they listen to and share stories with fellow participants, triggering a deliberate sense-making process that helps storytellers make new connections to other aspects of their lives and gain new narratives. They use these new narratives to create their digital stories, often leading to telling a different story than initially intended. This re-storying becomes an accomplishment and reshapes their understanding of their experiences and broader discourses around their health. Initially, storytellers feel vulnerable sharing sensitive and intimate stories about their health with strangers, worrying about being judged or misunderstood and about how their stories will unfold. However, this apprehension fades as they listen to the stories of others, finding inspiration and reinforcing the belief that their stories must be told.
The ripple effect of digital storytelling
Despite their initial apprehension, storytellers experience digital storytelling as a safe, supportive, health-promoting space. As they listen to the stories, they learn that all share similar experiences, creating an environment of understanding where they feel empowered to share their health experiences openly. The stories resonate with the storytellers and make them feel connected, validated, and comforted by learning that they are not alone. It is a ripple effect, which begins with the storytellers becoming story recipients. Engaging with the stories provokes an empathic response from fellow storytellers, triggering emotional and physical responses such as expressing admiration, feeling inspired or moved, or even embracing the narrator to comfort them. These responses, in turn, foster a sense of community belonging, make participants feel hopeful, and inspire a commitment beyond the workshop. Storytellers realize they are part of something bigger and feel compelled to tell their stories to help others. This shift from empathy to compassion involves a deep connection with the storytellers’ experiences of health, which requires a personal knowing of those experiences, evoking caring actions that bring comfort (58). Compassion here is a deliberate process in which storytellers treat others as they wish to be treated themselves.
Investing and processing emotions
The storytellers share more than similar stories and experiences. They vividly recognize the emotions described and portrayed in the stories shared as some of their own. Learning about and experiencing the emotions of others heightens the storytellers’ awareness of their own emotional state. Storytellers harness this intensified emotional awareness and use it to work and process their emotional burdens into their digital stories. Their emotional responses drive storytellers to open up to sharing things they would not express elsewhere and co-construct compelling stories that portray the authenticity and rawness of their experiences. Some storytellers refer to this process as therapeutic and cathartic because they experience some relief from their emotional burdens by sharing their stories with empathetic listeners who understand what they are going through.
Owning the script
The digital storytelling process affords storytellers the confidence to steer the narratives around their experiences. They acquire a sense of control over their personal narratives by articulating them into a digital story. Some storytellers view the process as an opportunity to challenge existing narratives and discourses about living with a particular condition or trauma. They deliberately seek to convey a message, a counternarrative, a first-hand and accurate account of their experiences. They aim to share their truths with others, even if it means evoking uncomfortable responses from recipients. Upon completing their digital stories, storytellers often recognize the potential impact of their narratives on others. Through this process, storytellers gain agency and are motivated to transform their digital stories into powerful tools to support others.
Discussion
This meta-synthesis used the framework analysis method to synthesize the health-promoting experiences of storytellers participating in a group-based digital storytelling workshop. Our GRADE-CERQual assessment of the findings provided evidence of moderate confidence that co-constructing digital stories about health experiences can shape the storytellers’ attitudes, values, beliefs, or behaviors. This is evidenced by four analytic themes containing health-promoting attributes likely to reasonably represent the storytellers’ experiences.
To gain an insight into how these four analytic themes contain health-promoting attributes, we employed the salutogenic lens underpinning this meta-synthesis. The first analytic theme — Re-storying Lived Experience — illustrates a narrative shift that can strengthen the storytellers’ sense of coherence (SOC). The SOC expresses an individual’s ability to successfully respond to a stressful situation when it is deemed worth dealing with. It is essential for developing and maintaining health, as a stronger SOC generally correlates with better-perceived health (59–61). The SOC can be strengthened by reflecting on stressful situations and identifying appropriate resources (62). We explained that the narrative shift results from a reflection process triggered by the storytellers’ deep engagement with the shared narratives. Although the included studies do not always detail the narratives` characteristics shared between the storytellers, it is plausible that storytellers are exposed to various narrative structures and contents that can have health-promoting attributes during the storytelling process. For instance, research evidence has identified key often shared mental health recovery narrative forms, including narratives of escape, such as resisting stigma, or narratives of enlightenment, where the storyteller views the illness or trauma as ultimately positive (63). There is strong evidence suggesting that narratives of this kind can be health-promoting by reducing stigma, helping individuals better understand mental illness and how to recover, or validating their experiences (13). Exposure to the narratives of individuals who have faced or overcome real-life health challenges has also been found to help storytellers (64). Thus, the various narratives forming the basis of the shared digital stories can be considered resources storytellers draw upon to re-examine or revise their own narratives, steering them towards health-promoting forms, content, or structures. From a salutogenic perspective, the more resources (generalized or specific) storytellers possess to appraise or reflect on their experiences, the more likely they are to shift their narratives and perceive them as more manageable and meaningful, strengthening their SOC (65, 66). The conceptual model on the effects of digital storytelling confirms that storytellers undergo an internal self-reflection exercise and engage in a retrospective sense-making process moderated by the dominant narratives. This process helps storytellers identify their stories’ turning points and transitions, derive meaning from them, and formulate new, more meaningful, and positive narratives (12).
The second analytical theme — The Ripple Effect Of Digital Storytelling — describes storytellers’ collective or social experiences. In the digital storytelling environment, the storytellers find comfort and a safe space to connect and empower each other. The salutogenic model explains that the SOC can be collectively strengthened in a group setting if the group perceives itself as a cohesive unit (67). This is linked to the group´s duration together, size, consensus in their perceptions, and its members’ interwoven self- and social identity (67, 68). Most studies in this meta-synthesis conducted workshops with groups of 6–8 individuals suffering from similar health conditions during three 8-hour long workshops, a level of engagement and group size that makes it plausible for the storytellers to see themselves as a cohesive group. In addition, they appear to achieve a high degree of consensus about their health experiences. Reports confirm that during the group phases, storytellers develop a sense of connection, unity, and community belonging (12, 54). This justifies the assumption that the shared stories and their underlying narratives can also become group resources that storytellers can collectively mobilize and activate to relieve the tension caused by their shared experiences. Thus, it is likely that the digital storytelling process is capable of strengthening the storytellers’ SOC by creating a group setting where each member is empowered to draw on these collective resources (67, 68).
The third analytic theme — Investing And Processing Emotions — denotes that regardless of the narrative characteristics the storytellers are exposed to, creating a digital story evokes a series of affective and emotional responses that can further contribute to a sense of individual and group well-being. Some of these emotional responses reported by recipients of stories can include positive emotions, such as feelings of gratitude or comfort, admiration or being inspired, and negative emotions, such as sadness, distress, or heartbreak (13). Storytellers embrace the opportunity to portray their emotions in a digital story and harness and process them to develop new perspectives of their experiences and move forward (69). Reports indicate that crafting a narrative about health enables individuals to gain a new perspective on their emotional experiences (70) and express and process them through reflection, reframing, or replacement (71). Working on these emotions in this form has been found to have significant health-promoting effects (72), for instance, in people who have cancer by reducing fatigue and improving their general mood (73) or in women with body image and appearance concerns affecting their sleep and eating behaviors by increasing their resilience and reducing physical symptoms (74). It appears that the mechanism behind these benefits involves emotional acceptance, where the storytellers do not seek to suppress or avoid their emotions but accept them, both negative and positive, reducing their emotional distress and enhancing emotional well-being (12). This way, storytellers establish strong emotional bonds with fellow storytellers, fostering unity, cohesion, and belonging. The salutogenic model explains that this type of emotional closeness to a social group contributes to the individual's appraisal that it is worth investing energy and resources to address a particular stressor (30, 31, 75). This appraisal is one of the most critical components of the SOC, meaningfulness, as it refers to the motivational and emotional entity that determines whether an individual is willing to deal with a particular situation (76). Meaningfulness can be maintained or enhanced by investing in four crucial areas of life, including main activity, inner emotions, social connections, and existential concerns (76). The three-phase digital storytelling process acknowledges that people “understand and give meaning to their lives through the stories they tell” (77) and addresses these four crucial areas of life. Thus, whilst it deals with comprehensibility and manageability, it focuses strongly on meaningfulness through reflection.
The fourth analytical theme — Owning The Script — explains that the narrative shift is a deliberate act by the storytellers driven by a newly gained sense of control. The collaborative approach to story construction instills the belief in storytellers that they can steer the narrative in the direction of their choosing. It has been reported that this is a turning point that allows storytellers to re-story their experiences and support their efforts to confront and deal with illness or traumatic events and move on with their lives (78). The salutogenic model can explain this theme by digital storytelling fostering empowerment and reflection that facilitates the identification of the stories and their narratives as resistance resources that influence behavior (62). This is often referred to as gaining personal agency in storytelling, where storytellers actively resist being defined by a dominant discourse and become the active change agents of their own narratives (63, 79). The conceptual model on the effects of digital storytelling cites Bandurás construct of self-efficacy to explain this phenomenon (12). Bandura postulated that self-efficacy primarily emerges through past experiences, vicarious experiences, verbal appraisals from trusted individuals, and emotional arousal (80), all aspects addressed during the storytelling process. According to Fiddian-Green and others, Storytellers work on shared and individual emotional challenges, fostering self-renewal and empowerment while highlighting various experiences that can be acted upon (12). This sense of control also stems from participants’ acquisition of technical and emotional skills that culminate in a digital story (12).
Limitations
We employed a comprehensive and systematic search strategy but included studies with limited methodological quality. While the reviewers considered these limitations in interpreting the data, recent reports have questioned the rigor of the CASP tool to identify potential methodological strengths and limitations of qualitative evidence (81). Thus, it is uncertain whether using a more comprehensive tool such as the recently published CAMELOT would decrease confidence in the findings. In addition, some of the included studies did not seek to primarily address the experiences of the storytellers, limiting the richness of the data for synthesis. We could not uncover the extent to which each phase of the digital storytelling process provides storytellers with the highest health-promoting value. The data from the included studies treated the entire process as a compound intervention.
Conclusion
This meta-synthesis addressed exclusively the health-promoting experiences of the storytellers participating in a facilitated, collaborative, and participative group-based digital storytelling workshop. The data provided evidence of moderate confidence that any health-promoting benefits of digital storytelling stem primarily from the storyteller's ability to revise and re-examine their existing stories and the narratives underpinning their lived experiences of health. This process results in a narrative shift likely to contain health-promoting attributes that can shape the storytellers’ health attitudes, values, beliefs, or behaviors. It is clear from the evidence that there is a before and after the workshop. However, considering that both negative and positive narratives could contain health-promoting attributes, there is a need to explore further the types of narratives shared or that emerge in such workshops and provide the strongest health-promoting benefit. Thus, professionals and researchers considering digital storytelling as a strategy in health promotion should carefully monitor the types of narratives shared and the directions that these take. The salutogenic model can explain how the process can be health-promoting for the individual storytellers and them as a cohesive group. Finally, we acknowledge that the analytical themes are not isolated constructs but emerge in response to one another. While we present them sequentially, they do not necessarily represent a linear progression of the storytellers’ experiences. Instead, they interact dynamically, each theme enriching and amplifying the others. This interconnectedness underscores the complexity of the storytellers’ health-promoting experiences and provides a more holistic and nuanced understanding.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Evans BC Crogan NL Bendel R. Storytelling intervention for patients with cancer: part 1–development and implementation. Oncol Nurs Forum. (2008) 35(2):257–64. 10.1188/08.ONF.257-26418321838 · doi ↗ · pubmed ↗
- 2Mc Call B Shallcross L Wilson M Fuller C Hayward A. Storytelling as a research tool used to explore insights and as an intervention in public health: a systematic narrative review. Int J Public Health. (2021) 66:10–2. 10.3389/ijph.2021.1604262 PMC 859284434795554 · doi ↗ · pubmed ↗
- 3West CH Rieger KL Kenny A Chooniedass R Mitchell KM Winther Klippenstein A Digital storytelling as a method in health research: a systematic review. Int J Qual Methods. (2022) 21:16094069221111118. 10.1177/16094069221111118 · doi ↗
- 4Kim SS Lee SA Mejia J Cooley ME Demarco RF. Pilot randomized controlled trial of a digital storytelling intervention for smoking cessation in women living with HIV. Ann Behav Med. (2019) 54(6):447–54. 10.1093/abm/kaz 062PMC 739121631863582 · doi ↗ · pubmed ↗
- 5Beltrán R Begun S. ‘It is medicine’:narratives of healing from the aotearoa digital storytelling as indigenous media project (ADSIMP). Psychol Dev Soc J. (2014) 26(2):155–79. 10.1177/0971333614549137 · doi ↗
- 6De Vecchi N Kenny A Dickson-Swift V Kidd S. How digital storytelling is used in mental health: a scoping review. Int J Ment Health Nurs. (2016) 25(3):183–93. 10.1111/inm.1220626900000 · doi ↗ · pubmed ↗
- 7Ferrari M Rice C Mc Kenzie K. ACE pathways project: therapeutic catharsis in digital storytelling. Psychiatr Serv. (2015) 66(5):556. 10.1176/appi.ps.66050525930226 · doi ↗ · pubmed ↗
- 8Davey NG Benjaminsen G. Telling tales: digital storytelling as a tool for qualitative data interpretation and communication. Int J Qual Methods. (2021) 20:16094069211022529. 10.1177/16094069211022529 · doi ↗