An unusual cause of fatal pulmonary embolism: A case report
Nino Cmor, Eva Dora, Martina Zitko, Tomaz Kocjan, Mitja Lainscak

TL;DR
A rare case of a fatal pulmonary embolism caused by an adrenal tumor invading the inferior vena cava is reported.
Contribution
This case highlights a rare and fatal complication of adrenal tumors extending into the IVC.
Findings
Adrenal tumors invading the IVC can lead to life-threatening pulmonary embolism.
Prompt imaging is crucial for diagnosing and managing such cases.
The patient had a secondary adrenal tumor from pulmonary adenocarcinoma that caused a fatal tumor thrombus.
Abstract
Adrenal tumours invading the inferior vena cava (IVC) are rare but can cause life-threatening complications such as pulmonary embolism. Early recognition, rapid diagnosis, and prompt imaging—including point-of-care ultrasonography (POCUS), echocardiography, and advanced modalities like CT and PET-CT—are essential for optimal management. We present a patient with pulmonary adenocarcinoma and secondary adrenal tumour that extended into IVC and caused fatal tumour thrombus pulmonary embolism.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
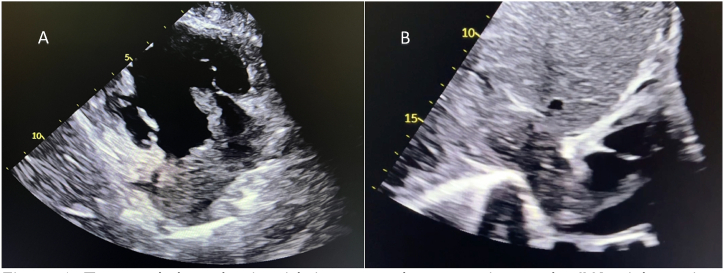 Figure 1
Figure 1 Figure 2
Figure 2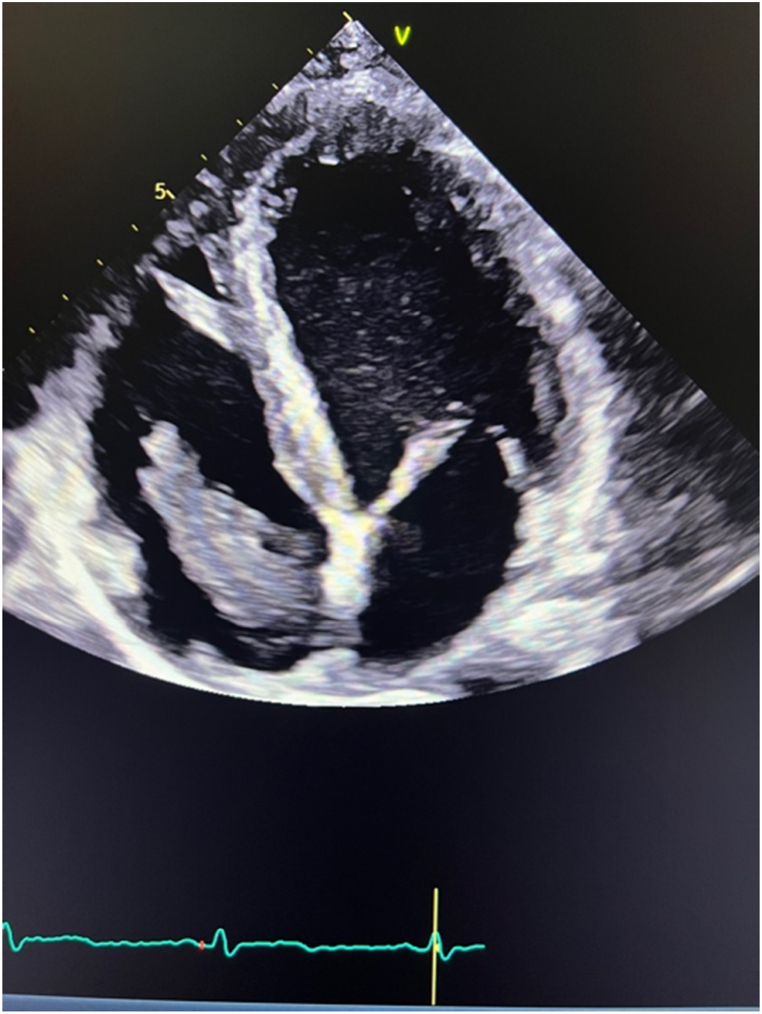 Figure 3
Figure 3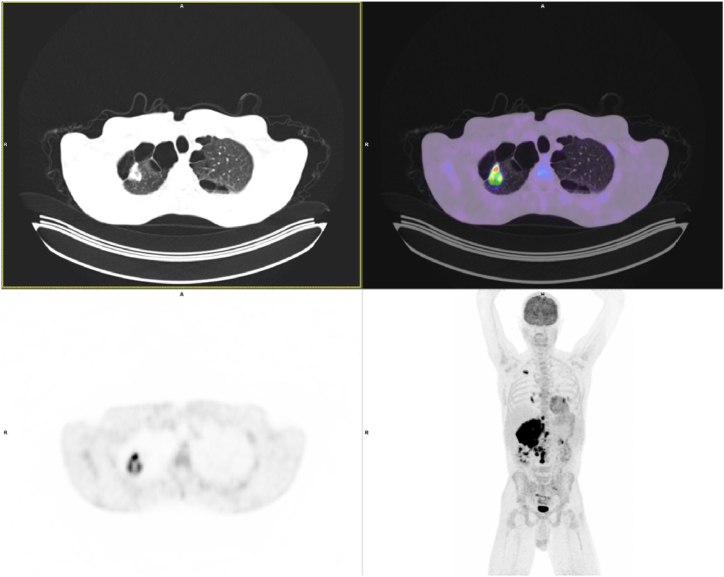 Figure 4
Figure 4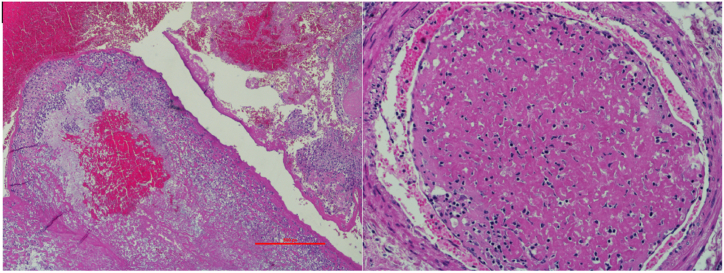 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal and Paraganglionic Tumors · Cardiac tumors and thrombi · Vascular anomalies and interventions
Introduction
1
Adrenal tumours extending into inferior vena cava (IVC) present considerable clinical challenges due to their rarity and potential for severe complications [[1], [2], [3], [4]]. This rare condition involves tumour thrombus infiltration from the adrenal gland into the IVC, sometimes reaching cardiac chambers, and can lead to pulmonary embolism (PE) [5]. Symptoms like dyspnoea and chest pain prompt for diagnosis, with emergency room imaging (e.g. point of care ultrasonography - POCUS, echocardiography) having a central role in visualizing thrombus, its extension and potential cardiac involvement [[6], [7], [8], [9]]. We describe a case of a secondary adrenal tumour extending into IVC diagnosed by echocardiography.
Case report
2
A 45-year-old man, without relevant medical history, presented to the emergency department with pain under the right rib cage. The pain had persisted for three weeks and worsened with movement, leading him to initially suspect a muscle strain. Three days prior, he noticed swelling in both legs and began experiencing dyspnoea during exercise. He also reported an unintentional weight loss of 8 kg over the last three months.
Clinical examination revealed tenderness on palpation under the right rib cage and bilateral leg oedema. A 12-lead ECG showed no abnormalities, and the chest X-ray was within normal limits. Laboratory findings were significant for elevated levels of alkaline phosphatase (ALP = 18.82 μkat/L; reference value 0,67-2,15 μkat/L) and gamma-glutamyl transferase (GGT = 5.54 μkat/L; reference value < 0,92 μkat/L), with normal bilirubin levels and hypoalbuminemia (albumin = 25 g/L).
POCUS showed a right atrial mass with extension into the right ventricle and an obliterated IVC (Fig. 1A–B/VIDEO 1). A contrast-enhanced computed tomography (CT) scan of the abdomen and thorax revealed a 107 × 84 mm large tumorous formation of the right adrenal gland, presumably an adrenocortical carcinoma, with thrombus extending into the IVC and further into both common iliac veins, the right renal vein, the middle hepatic vein, and into the right atrium. Additionally, a lesion was found in the upper right pulmonary lobe, with enlarged right hilar lymph nodes (Fig. 2). CT angiography of the pulmonary arteries revealed a segmental PE.Fig. 1. Tumoural thrombosis with intravascular extension to the IVC, right atrium and ventricle on bedside echocardiography. A – parasternal long axis/right ventricular inflow view B- subxiphoid view.Fig. 1. Fig. 2A contrast-enhanced computed tomography scan of the abdomen and thorax: A large tumorous formation of the right adrenal gland, with thrombus extending into the IVC and right atrium.Fig. 2
The following are the Supplementary data related to this article:
Supplementary data related to this article can be found online at https://doi.org/10.1016/j.rmcr.2025.102303.Multimedia Component 1Multimedia Component 1
Subcutaneous nadroparin was initiated, and the patient was transferred to a tertiary care hospital for diagnostic assessment. Expanded hormonal testing to exclude a functional adrenal mass (1 mg dexamethasone suppression test, aldosterone, plasma renin activity, 17-OH progesterone, dehydroepiandrosterone sulphate, androstenedione, estradiol, plasma metanephrines and normetanephrines) was normal.
A comprehensive echocardiography showed a hypoechogenic mass extending from the IVC into the right atrium, prolapsing into the right ventricle, without tricuspid valve dysfunction (Fig. 3/VIDEO 2–4). After excluding a pheochromocytoma, a biopsy of the tumour was performed. Histopathology report diagnosed a poorly differentiated pulmonary adenocarcinoma.Fig. 3. Tumoral thrombosis in right atrium and ventricle with a normal left and right ventricular function on echocardiography.Fig. 3
The following are the Supplementary data related to this article:
A whole-body 18F-fluorodeoxyglucose positron emission tomography-computed tomography (PET/CT) scan revealed a hypermetabolic tumour in the right upper lung lobe, with signs of metastatic spread to ipsilateral hilar lymph nodes, ipsilateral and contralateral mediastinal lymph nodes, abdominal lymph nodes, and the right adrenal gland with intravascular extension into the IVC (Fig. 4).Fig. 4. Whole-body 18F-fluorodeoxyglucose positron emission tomography-computed tomography: a hypermetabolic tumour in the right upper lung lobe, with signs of metastatic spread to ipsilateral hilar lymph nodes, ipsilateral and contralateral mediastinal lymph nodes, abdominal lymph nodes, and the right adrenal gland with intravascular extension into the IVC.Fig. 4
Based on comprehensive diagnostic workup, the patient was diagnosed with pulmonary adenocarcinoma with metastatic spread to the right adrenal gland and intravascular extension to the IVC and right atrium. A multidisciplinary team recommended immunotherapy for the primary tumour and palliative radiotherapy of secondary tumour. Due to advanced tumour stage surgical treatment was not seen as a primary option. Patient was discharged after 44 days on subcutaneous nadroparin and analgesics with an outpatient management plan.
Pembrolizumab was initiated and patient had regular radiotherapy of secondary tumour, as planned. During follow-up, liver enzymes normalized, and he was switched to oral anticoagulation with edoxaban. A CT scan six months later demonstrated a reduction of both primary and secondary tumour, along with reduction of tumour thrombus in the IVC while right atrial thrombus was larger. No PE was seen and he was switched back to subcutaneous nadroparin. During regular follow up visit 8 months post discharge patient felt better, had no specific complaints and he gained weight; nadroparin was discontinued because of new-onset thrombocytopenia.
Two days after last follow-up visit, he collapsed at home; his partner started resuscitation and called the emergency team. On arrival, he was in asystolic cardiac arrest; despite prolonged and complete resuscitation the patient died. Post-mortem examination confirmed the primary and secondary tumour, and massive PE in proximal left and right pulmonary artery. Emboli were histologically characterised as tumour thrombi (Fig. 5).Fig. 5. The histologic specimen of the patient's massive pulmonary embolism, which was histologically characterised as tumour thrombi.Fig. 5
Discussion
3
Primary and secondary adrenal tumours extending into IVC present significant diagnostic and therapeutic challenges due to their rarity and potential for severe complications [[1], [2], [3], [4]]. These tumours encompass various neoplasms, including adrenocortical carcinomas (ACCs), pheochromocytomas, and metastatic tumours [1]. According to Chesson et al., from 1952 to 2000, there were 105 reported cases of histologically confirmed adrenal tumours involving the IVC, consisting of 78 ACCs, 16 pheochromocytomas, 3 neuroblastomas, and others [2]. Secondary tumours involving the IVC are extremely rare and to the best of authors knowledge, this is the first report of pulmonary adenocarcinoma with secondary adrenal gland involvement that extended into the IVC and right heart.
Patients often present with symptoms consistent with inferior vena cava syndrome, such as abdominal pain, weight loss, dyspnoea, chest pain, and leg swelling [[1], [2], [3], [4]]. In our case, the patient presented with significant leg swelling and dyspnoea, raising suspicion of heart failure. POCUS was performed in the emergency room and was the key for further evaluation [9]. The findings confirmed the thrombus in the IVC, right atrium and a PE. Major left and right ventricular dysfunction were excluded. Nadroparin was initiated as it was not possible to differentiate the thrombus aetiology only by emergency imaging.
The management of adrenal gland tumours with IVC extension requires a multidisciplinary approach [1]. Anticoagulation therapy is a routine early in the patient management due to increased risk of venous thromboembolism [1,5], and should be maintained once the final diagnosis is made. Our patient had a secondary adrenal gland tumour, which according to the guidelines is a contraindication for surgery [1]. Therefore, radiotherapy and immunotherapy in an outpatient setting, along with a close follow-up, pain management and palliative service was organized.
During follow-up, the patient's performance improved, and the malignant disease was in regression. Due to new-onset thrombocytopenia, anticoagulation therapy was discontinued as per guidelines [10]. Two days later, he experienced fatal PE. In the context of this patient, the key question was the embolism origin, with two main potential sources: tumour thrombus or venous thrombus. Post-mortem resolved this dilemma and confirmed massive pulmonary embolism due to tumour thrombi. The cause of death in this young male patient with advanced malignant disease may have been preventable but specific treatment, surgical removal of secondary tumour, is not in line with the current guidelines [1]. Because the guidelines provide general advice that must be tailored to each patient, one could argue that repeated multidisciplinary consultations may be necessary to reassess the patient's condition and weigh the benefits and risks of specific treatment procedures. It is also possible that the oncologic therapy itself mobilized the tumor thrombus, contributing to the development of PE. Therefore, regular, individualized follow-up assessments and reevaluation of the management plan should be implemented for patients with a young biological age and good overall performance status to prevent premature and potentially fatal complications, as illustrated in this case.
Conclusion
4
This case promotes crucial role of multimodal imaging and multidisciplinary teamwork to optimize management of adrenal tumours with IVC extension. Additionally, we highlight patient-oriented evaluation of potentially preventable premature death due to tumour pulmonary embolism. Although surgical removal of metastatic adrenal tumours is not guideline-recommended, this could be challenged in patients who respond well to specific therapy, have good performance status and longer than average expected survival. Authors are proponents of regular multidisciplinary consultations to reassess treatment options which may prevent fatal intravascular complications.
CRediT authorship contribution statement
Nino Cmor: Writing – review & editing, Writing – original draft, Conceptualization. Eva Dora: Writing – review & editing. Martina Zitko: Writing – review & editing. Tomaz Kocjan: Writing – review & editing. Mitja Lainscak: Writing – review & editing, Conceptualization.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fassnacht M.Dekkers O.M.Else T.Baudin E.Berruti A.De Krijger R.R.European society of endocrinology Clinical practice guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the european network for the study of adrenal tumors Eur. J. Endocrinol.17942018 Oct G 1G 463029988410.1530/EJE-18-0608 · doi ↗ · pubmed ↗
- 2Chesson J.P.Theodorescu D.Adrenal tumor with caval extension: case report and review of the literature Scand. J. Urol. Nephrol.3612002 Jan 171731200236210.1080/003655902317259409 · doi ↗ · pubmed ↗
- 3Patil S.Singh V.Kumar A.Sankhwar S.N.Adrenocortical carcinoma with tumour thrombus extension to right atrium: a rare finding in uncommon tumour BMJ Case Rep.2013 Oct 14bcr 2013200804
- 4Verma Y.Mohith A.Shimjee S.Batra R.B.Reddy Aleti S.Verma B.S.Adrenal tumor with inferior Vena Cava tumor thrombus: a case report and review of literature J. Endourol Case Rep.642020 Dec 14934963345771110.1089/cren.2020.0172 PMC 7803237 · doi ↗ · pubmed ↗
- 5Lee H.J.Kwak J.Y.Kim Y.J.Kim T.H.Lee J.D.Lee H.W.A case of an adrenocortical carcinoma with pulmonary embolism as the initial manifestation Endocrinol Metab 271201293
- 6Rosen B.Rozenman Y.Harpaz D.Extension of adrenocortical carcinoma into the right atrium – echocardiographic diagnosis: a case report Cardiovasc. Ultrasound 112003 Dec 51277718010.1186/1476-7120-1-5PMC 156660 · doi ↗ · pubmed ↗
- 7Kim K.H.Park J.C.Lim S.Y.Sohn I.S.Yun K.H.Cho S.H.A case of non-functioning huge adrenocortical carcinoma extending into inferior vena cava and right atrium J. Kor. Med. Sci.2132006572
- 8Abdelnabi M.Almaghraby A.Saleh Y.Abd El Samad S.Right atrial and ventricular invasion by adrenal carcinoma: a case report J. Cardiol. Cases 2022019 Aug 42443144030910.1016/j.jccase.2019.03.010PMC 6698249 · doi ↗ · pubmed ↗