Immune reconstitution syndrome-mediated acute fulminant tuberculous myopericarditis in young postpartum patient: a case report
Mochamad Rizky Hendiperdana, Astrid Putri, Dyan Tony Cahya, Nugroho Sigit Hartanto

TL;DR
A young postpartum woman developed severe heart inflammation due to tuberculosis, likely caused by immune reconstitution syndrome, and recovered with timely treatment.
Contribution
Highlights IRS as a potential mechanism for acute tuberculous myopericarditis in postpartum patients.
Findings
The patient showed complete left ventricular recovery after treatment.
Anti-tuberculosis therapy led to significant clinical improvement.
IRS may mediate acute fulminant tuberculosis myopericarditis postpartum.
Abstract
Postpartum symptom deterioration of tuberculosis is associated with the condition that is termed immune reconstitution syndrome (IRS). In the postpartum period, restitution of cellular immunity mediates the hypersensitivity reaction to Mycobacterium tuberculosis (MTB) antigen that hypothetically results in acute fulminant tuberculosis myopericarditis. A 29-year-old woman develop acute respiratory distress 5 days following caesarean section. On admission vital sign indicating haemodynamic instability. Chest X-ray showed extensive pulmonary consolidation which signified for pulmonary tuberculosis. Echocardiography finding revealed left ventricular (LV) dysfunction with minimal pericardial effusion. Cardiac magnetic resonance imaging showed non-ischaemic late gadolinium enhancement (LGE) distribution. Upon to this finding, acute fulminant tuberculosis myopericarditis diagnosis was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
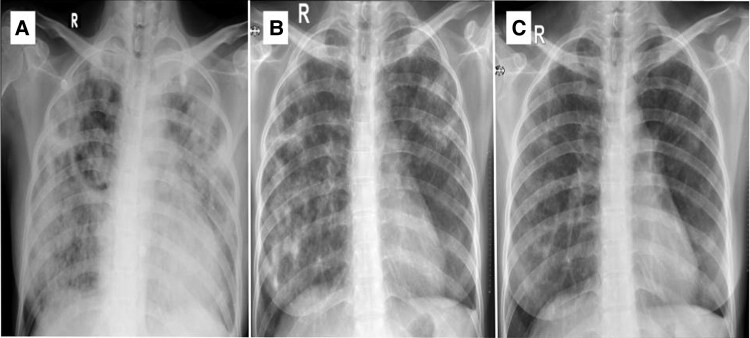 Figure 1
Figure 1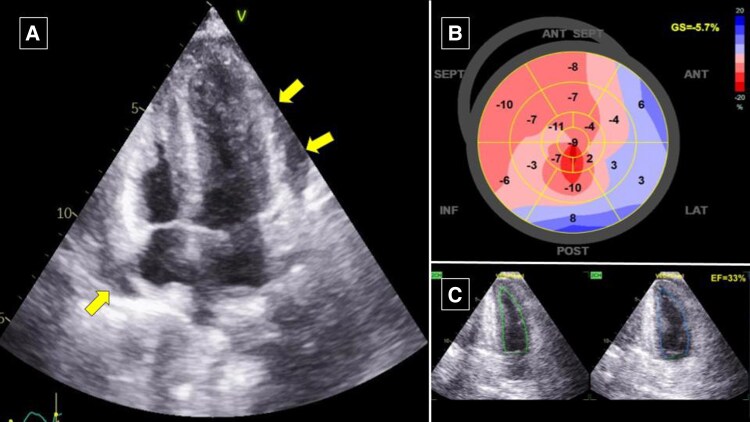 Figure 2
Figure 2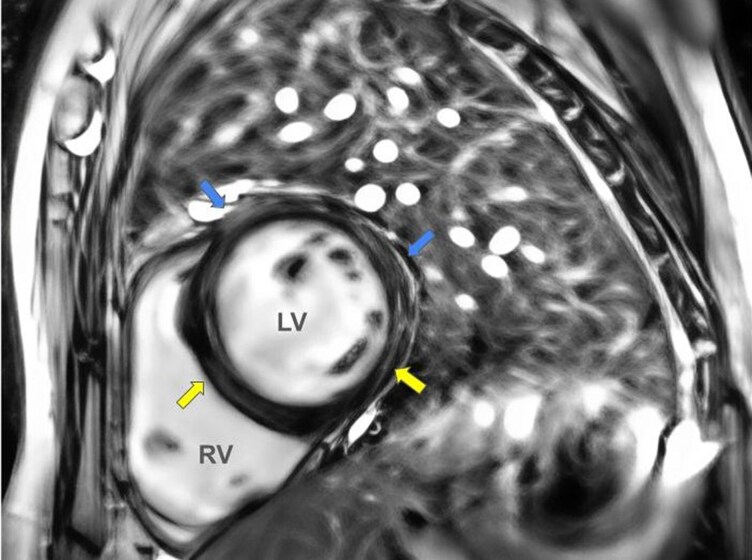 Figure 3
Figure 3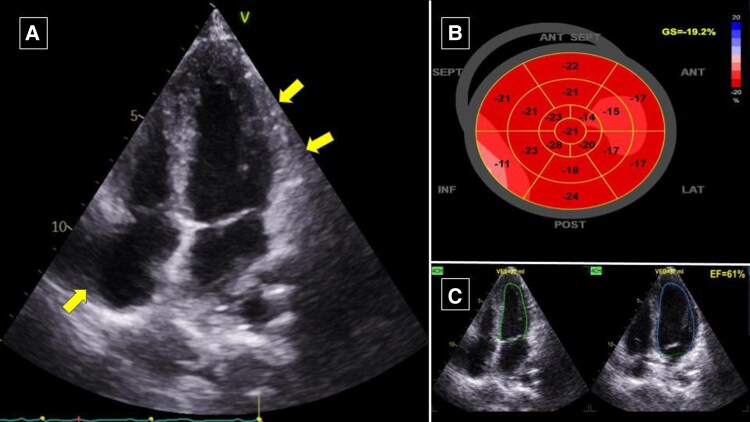 Figure 4
Figure 4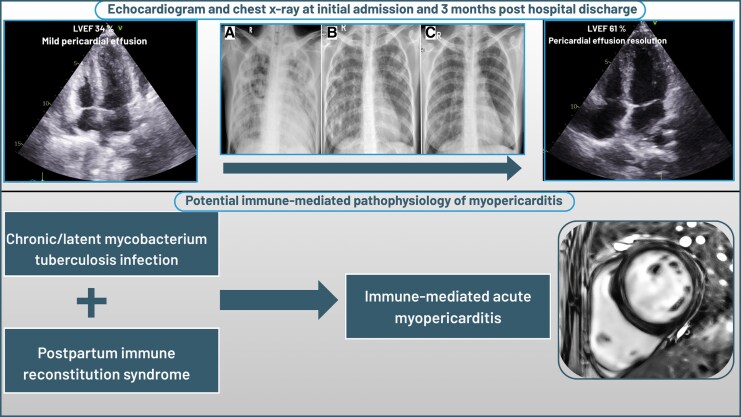 Figure 5
Figure 5| Timeline | Events |
|---|---|
| 10 days prior to admission | Caesarean section procedure for the third pregnancy |
| 5 days prior to admission | Severe breathlessness commenced with progressive worsening |
| Admission (Day 0) | Presented at emergency ward with unstable haemodynamic: diaphoretic and distressed with a heart rate 153 beats/minute and marked hypotension with blood pressure (BP) 65/31 (45) mmHg, peripheral oxygen saturation 95%, and respiratory rate 22 breaths/minute. |
| Day 1 | Admitted to the intensive care unit for further management and haemodynamic stabilization. |
| Day 2 | GDMT for heart failure start to be administered: |
| Day 3 | Bisoprolol 2.5 mg o.d. was added. |
| Day 5 | CMR imaging showed LGE with midwall distribution at inferoseptal and inferolateral, subepicardial LGE at anteroseptal and anterolateral LV territory which signifies for non-ischaemic LGE distribution. |
| Day 8 | Discharged uneventfully with serum lactate 1.5 mmol/l. Discharged medication: |
| One-month follow-up | Symptom improved with echocardiographic signs of LV function recovery with LVEF of 65%. |
| Three-month follow-up | Complete LV recovery with LVEF 61%. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Infectious Diseases and Tuberculosis · Takotsubo Cardiomyopathy and Associated Phenomena
Introduction
Tuberculosis is a global health burden particularly in the low-middle income countries that caused up to 1.4 million annual deaths worldwide.^1–5^ Postpartum symptom deterioration of tuberculosis is associated with the condition that is termed immune reconstitution syndrome (IRS).^6,7^ In the postpartum period, restitution of cellular immunity mediates the hypersensitivity reaction to Mycobacterium tuberculosis (MTB) antigen that hypothetically results in acute fulminant tuberculous myopericarditis.^7^ Herein, we reported a case of IRS-mediated postpartum fulminant tuberculous myopericarditis with left ventricular (LV) dysfunction which was successfully treated with anti-tuberculosis treatment (ATT), cortisteroid, and heart failure medication.
Summary figure
**: **
LVEF, left ventricular ejection fraction; GDMT, guideline-directed medical therapy; ATT, anti-tuberculosis treatment; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement.
Case summary
A 29-year-old woman presented to the emergency department with severe breathlessness in 5 days after the caesarean section procedure for her third delivery. Dyspnoea worsened progressively until the patient presented at our centre. On admission vital signs: the patient looks diaphoretic and distressed with a heart rate 153 beats/minute and marked hypotension with blood pressure (BP) 65/31 (45) mmHg, peripheral oxygen saturation 95%, and respiratory rate 22 breaths/minute. The significant physical examination finding was bilateral lung crackles on chest auscultation. There was no history of pulmonary infection or any cardiac disease during recent and previous pregnancy. The patient noticed significant body weight reduction that was accompanied by non-productive cough 4 months prior to delivery.
Electrocardiography revealed marked sinus tachycardia with poor R wave progression. Chest X-ray showed cardiomegaly with diffuse pulmonary consolidation which signified for pulmonary tuberculosis (Figure 1A). Laboratory results were euthyroid, increased in serum creatinine (2.8 mg/dl and eGFR 21.23 ml/min), lymphopenia 570 (n.v. 800–4000/µl), increased erythrocyte sedimentation rate to 54 mm/h, significant increase D-dimer >10 000 ng/ml and lactatemia (4.4 mmol/l). Other laboratory results were unremarkable.
Serial chest roentgenography at (A) baseline initial admission; (B) 1-month post-hospital discharge; (C) 3 months after hospital discharge. The baseline X-ray showed diffuse consolidation over both lung lobes that followed gradual improvement of pulmonary consolidation at 1 month and 3 months after hospital discharge.
Transthoracic echocardiography revealed global hypokinetic LV with ejection fraction (LVEF) of 34%, LV GLS (−5.7%), minimal pericardial effusion was also observed, and other findings were insignificant (Figure 2) (see Supplementary material online, Video S1). Upon to these findings, the patient was diagnosed with acute heart failure and cardiogenic shock that suspiciously caused by two most possible aetiology. Firstly, it was highly suspected that the aetiology is peripartum cardiomyopathy (PPCM) and lastly, the tuberculous myopericarditis process.
Baseline transthoracic echocardiography revealed (A) minimal pericardial effusion around the heart from apical 4-chamber view (arrow); (B) LV GLS (−5.7%); (C) global hypokinetic with LVEF of 34%. LV, left ventricular; GLS, global longitudinal strain; LVEF, left ventricular ejection fraction.
The patient was admitted to the intensive cardiac care unit for further management and haemodynamic stabilization. The patient was administered dobutamine along with intravenous furosemide for decongestion purpose. Guideline-directed medical therapy (GDMT) for heart failure was administered with regimen ramipril 2.5 mg o.d., spironolactone 25 mg o.d., and warfarin 2 mg o.d. After several days of haemodynamic stabilization, bisoprolol 2.5 mg o.d. was added. Due to diagnosis establishment for a tuberculous process, the ATT with RHZE regimen (rifampicin 300 mg, isoniazid 150 mg, pyrazinamide 800 mg, and ethambutol 550 mg) and intravenous hydrocortisone 100 mg/8 h were administered.
At the 5th admission day, patient symptoms were resolved and haemodynamic was improved (HR 110 b.p.m., BP 100/50 mmHg). Serum lactate and creatinine were also improved (2.7 mmol/l and 1.2 mg/dl, respectively). Patient was then transferred to the medical ward with continuous GDMT uptitration. Cardiac magnetic resonance (CMR) imaging showed late gadolinium enhancement (LGE) with midwall distribution at inferoseptal and inferolateral, subepicardial LGE at anteroseptal and anterolateral LV territory which signifies for non-ischaemic LGE distribution (Figure 3). Patient then diagnosed as tuberculous myopericarditis.
CMR imaging showed LGE with midwall distribution at inferoseptal and inferolateral, subepicardial LGE at anteroseptal and anterolateral LV territory which signifies for non-ischaemic LGE distribution. CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement; LV, left ventricular.
At the 8th admission day, the patient was discharged uneventfully with stable haemodynamic and serum lactate 1.5 mmol/l with lactate clearance at the end of admission was 65.9%. The patient was discharged with medication furosemide 40 mg o.d., ramipril 10 mg o.d., spironolactone 50 mg o.d., bisoprolol 5 mg o.d., hydrocortisone 20 mg o.d., and ATT.
On an outpatient visit 1 month after discharge, the symptom resolved with echocardiographic signs of LV function recovery with LVEF of 65% with LV GLS (−15.3%). While symptom improvement was observed, we found significant change in chest X-ray infiltrate which depicted diffuse pulmonary tuberculosis (Figure 1B). Three months post-discharge visit, the patient showed complete LV recovery with LVEF 61% and LV GLS (−19.2%) (Figure 4). Chest X-ray also showed resolution of pulmonary consolidation (Figure 1C). The GDMT and ATT regimens were continued.
Three-month follow-up transthoracic echocardiography showed (A) resolution of pericardial effusion from apical four-chamber view (arrow); (B) significant improvement of LV GLS to (−19.2%); (C) significant improvement in LVEF of 61%. LV, left ventricular; GLS, global longitudinal strain; LVEF, left ventricular ejection fraction.
Discussion
Myocardial involvement in tuberculosis is a rare case in published reports. The prevalence is 0.14%–2% from various series.^3,8,9^ The clinical presentation consists of ventricular arrhythmia, acute heart failure due to LV systolic dysfunction, and sudden cardiac death.^9^ This case was mimicking PPCM due to history of recent postpartum episodes. The presence of pericardial effusion in our case depicts pericardial involvement process. Hence, the aetiology of tuberculosis is more likely because of the myocardial involvement in tuberculosis is commonly in the form of myopericarditis.^8^
It is hypothesized that the immunological system adaptation that developed immediately in the postpartum period mediates the tuberculous myopericarditis by hypersensitivity reaction. Therefore, IRS phenomena possibly induced worsened tuberculosis in our patient which manifested as myopericarditis and acute heart failure.^6^ The possible explanation concerning the pathogenesis in this case was the involvement of immune-mediated hypersensitivity from IRS to the myocardium and pericardium. The clinicians had to put a high suspicion index of IRS in postpartum patients with unstable haemodynamic.
It is also important to consider the acute fulminant tuberculous myopericarditis in unexplained causes of heart failure that developed immediately in the postpartum period. The chronic and latent nature of tuberculous made recent infection is less likely. Therefore, the IRS-induced tuberculous myopericarditis is reasonable to be considered as an underlying mechanism (Figure 5).^6^ Unfortunately, endomyocardial biopsy for diagnosis establishment was not performed in our case due to resource limitation. Therefore, in our case, the administration of ATT was relied on TB suspicion from the chest X-ray that demonstrated diffuse pulmonary consolidation and CMR which showed non-ischaemic LGE distribution.
Visual summary of patient’s clinical course and proposed pathophysiological process of disease.
Raffali et al. reported a young woman with heart failure and disseminated TB who was successfully treated with ATT regimen and GDMT.^9^ On the other hand, Agarwal et al. and Cowley et al. reported a fatal case of acute fulminant tuberculous myocarditis that was later confirmed by post-mortem biopsy.^4,10^ Based on collected reports from Michira et al., 81% of tuberculous myocarditis is predominant in young patients (below 45 years).^2^ While Shaikh et al. reported a similar case in an older man patient, which showed age distribution variability.^3^ Myocardial involvement of tuberculosis in the paediatric population has also been reported.^11,12^
Eighty per cent of tuberculous myocarditis fatal cases occurred in female patients with LV dysfunction whom also observed in our case.^2^ Fortunately, our case showed significant clinical response to ATT and GDMT with significant LV systolic function improvement several weeks after therapy. Most of the reported cases of tuberculous myopericarditis also showed significant improvement after ATT initiation.^5,9^ Unfortunately, due to the low incidence rate, subtle and slowly progressing nature of this condition made the antemortem diagnosis rarely.^2,10^ Therefore, clinician vigilance and awareness for early diagnosis and timely management of ATT and GDMT as effective therapy for tuberculous myopericarditis are of the utmost importance in the management of this reversible aetiology of heart failure,^1,2,4^ as demonstrated in our case that clinical improvement and myocardial reverse remodelling were observed. Since the immune-mediated hypersensitivity mechanism is prominent in this case, the role of systemic steroids to suppress immune response is also important to be considered as a myocarditis management although controversial.^7^
Lead author biography
M. Rizky Hendiperdana MD, FIHA, currently a provider cardiology service at Pandan Arang General Public Hospital, Boyolali, Indonesia. He completed his training in cardiovascular medicine field at the Department of Cardiology and Vascular Medicine, Faculty of Medicine University of Indonesia/National Cardiovascular Centre Harapan Kita, Jakarta, Indonesia.
Supplementary Material
ytaf542_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1López-López JP, Posada-Martínez EL, Saldarriaga C, Wyss F, Negretti CP, Alexander B, et al Tuberculosis and the heart. J Am Heart Assoc 2021;10:e 019435.33733808 10.1161/JAHA.120.019435 PMC 8174360 · doi ↗ · pubmed ↗
- 2Michira BN, Alkizim FO, Matheka DM. Patterns and clinical manifestations of tuberculous myocarditis: a systematic review of cases. Pan Afr Med J 2015;21:118.26327955 10.11604/pamj.2015.21.118.4282 PMC 4546727 · doi ↗ · pubmed ↗
- 3Shaikh GA, Yaqoob S, Batool F, Waseem R, Shah HH, Abbasi AA, et al A rare case of tuberculous myocarditis: a diagnostic challenge in a tuberculosis-endemic country. Clin Case Rep 2023;11:e 8224.38028083 10.1002/ccr 3.8224 PMC 10654465 · doi ↗ · pubmed ↗
- 4Agarwal R, Malhotra P, Awasthi A, Kakkar N, Gupta D. Tuberculous dilated cardiomyopathy: an under-recognized entity? BMC Infect Dis 2005;5:29.15857515 10.1186/1471-2334-5-29PMC 1090580 · doi ↗ · pubmed ↗
- 5Al-Jahdali F, Al-Harbi A, Baharoon S, Al Gamdi M, Al-Jahdali H. Tuberculous myocarditis is not always fatal: report of three confirmed cases with uneventful outcome. Int J Mycobacteriol 2017;6:111–115.28317817 10.4103/ijmy.ijmy_9_17 · doi ↗ · pubmed ↗
- 6Cheng VC, Woo PC, Lau SK, Cheung CH, Yung RW, Yam LY, et al Peripartum tuberculosis as a form of immunorestitution disease. Eur J Clin Microbiol Infect Dis 2003;22:313–317.12743831 10.1007/s 10096-003-0927-1 · doi ↗ · pubmed ↗
- 7Shinohara T, Kagawa K, Okano Y, Sawada T, Kobayashi T, Takikawa M, et al Disseminated tuberculosis after pregnancy progressed to paradoxical response to the treatment: report of two cases. BMC Infect Dis 2016;16:284.27297079 10.1186/s 12879-016-1624-x PMC 4906776 · doi ↗ · pubmed ↗
- 8Marcu DTM, Adam CA, Mitu F, Cumpat C, Onofrei VA, Zabara ML, et al Cardiovascular involvement in tuberculosis: from pathophysiology to diagnosis and complications—a narrative review. Diagnostics (Basel) 2023;13:432.36766543 10.3390/diagnostics 13030432 PMC 9914020 · doi ↗ · pubmed ↗