P-wave oversensing during atrial tachycardia in patients with an extravascular ICD
Alexander Breitenstein

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
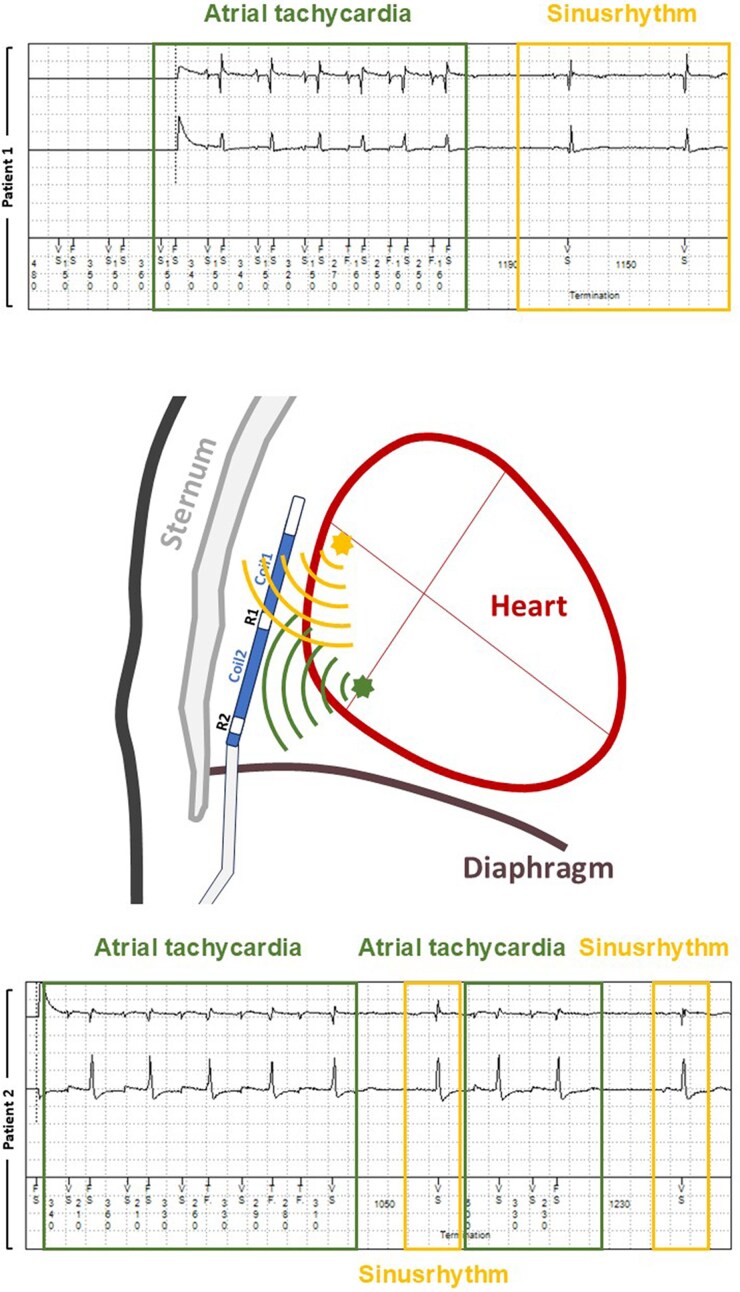 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes · Cardiac pacing and defibrillation studies
Case description
The first patient, a 54-year-old woman with hypertrophic cardiomyopathy, received an EV-ICD for primary prevention. The second patient (48-year-old man) experienced an out-of-hospital cardiac arrest due to ventricular fibrillation without an identifiable reversible cause. In both cases, implantation was uneventful, and initial sensing parameters showed good ventricular signal amplitude with no significant P-wave oversensing during sinus rhythm. In both patients, the sensing vector was Ring1-Ring2 (near-field sensing between the sensing poles), with a ventricular sensitivity of 0.15 mV (standard recommendation). The oversensing prevention was set to level 4 (on a scale from 1 to 6, where 1 is the most sensitive and 6 the least sensitive).
However, during follow-up, remote transmissions revealed P-wave oversensing during brief episodes of atrial tachycardia in both patients (Figure 1). These episodes were associated with altered atrial electrical activation resulting in increased P-wave amplitude and changed morphology which is a known phenomenon for atrial tachycardias,^1^ leading to oversensing by the device. Although the episodes were self-limiting and did not trigger inappropriate therapy, they highlight a potential risk for signal oversensing. If such arrhythmias are longer-lasting, it may be useful to investigate for potential atrial oversensing during episodes of tachycardia. Due to the short and self-limiting character of these episodes in both patients, no change in device settings were necessary. However, adjusting the sensing vector or sensitivity settings may mitigate this issue. Similar to transvenous defibrillators, the sensitivity in the substernal ICD is dynamic and increases with time after the last ventricular event. For the first period, after a blanking phase, the oversensing prevention feature regulates the sensitivity of the device for a certain time period (on a scale from 1 to 6, where 1 is the most sensitive and 6 the least sensitive) followed by the baseline sensitivity (which is nominally set to 0.15 mV). Additionally, advanced device algorithms such as the ‘Smart Sense’ enhances the discrimination between true ventricular arrhythmias and P-wave oversensing (The ‘Smart Sense’ algorithm is a Medtronic specific feature which detects alternating low (P-wave) and high (R-wave) amplitude signals together with a QRS farfield morphology which is similar to normal sinus rhythm).^2^
Arrhythmia recording of patient 1 (upper panel) and patient 2 (lower panel) during brief episodes of atrial tachycardia with subsequent P-wave oversensing, which is not present during sinus rhythm.
Consent: Both patients have given written informed consent (compliant with COPE guidelines).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee JM, Fynn SP. P wave morphology in guiding the ablation strategy of focal atrial tachycardias and atrial flutter. Curr Cardiol Rev 2015;11:103–110.25308814 10.2174/1573403 X 10666141013121252 PMC 4356716 · doi ↗ · pubmed ↗
- 2Swerdlow CD, Zhang X, Sawchuk R, Greenhut S, Grinberg Y, Liu Y, et al Design and preliminary results of sensing and detection for an extravascular implantable cardioverter-defibrillator. JACC Clin Electrophysiol 2021;7:1387–1399.33933410 10.1016/j.jacep.2021.03.004 · doi ↗ · pubmed ↗