Survival probability and under-five mortality predictors in Western Kenya between 2015 and 2020
Harun Odhiambo Owuor, Asito Stephen Amolo, George Aol, Fredrick Onduru, Richard Omore, Beth Tippett Barr, Victor Akelo, Stephen Munga, Dickens Samwel Omondi Aduda

TL;DR
This study identifies key factors affecting under-five mortality in Siaya County, Kenya, to guide targeted interventions for reducing child deaths.
Contribution
The study provides region-specific predictors of under-five mortality in Siaya County using longitudinal surveillance data.
Findings
Under-five mortality in Siaya was 63/1000 live births, higher than the national average.
Key predictors include maternal education, ANC visits, delivery location, maternal age, and sanitation.
Male gender and younger maternal age were associated with increased mortality risk.
Abstract
Despite gains in reducing under-five mortality in Kenya from 52 to 41.6 deaths per 1000 live births between 2015 and 2022, the rate remains notably higher than the Sustainable Development Goal (SDG) 3 target of 25 deaths per 1000 by 2030. The impact of interventions on risk factors and socio-structural inequities have varied across regions, indicating potential effects of unaddressed issues. There is a need to further understand the key drivers of under-5 mortality in given contexts to help improve intervention effectiveness. To estimate the survival probability and determine predictors of under-five mortality in Siaya County. The study utilized secondary data from the Siaya Health Demographic Surveillance System from 2015 to 2020; semi-annual population-based longitudinal surveillance, and data analyzed in cohort design. We performed both descriptive and multivariable analyses. We…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
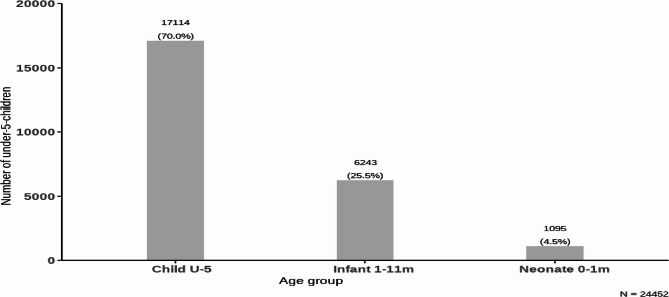 Figure 1
Figure 1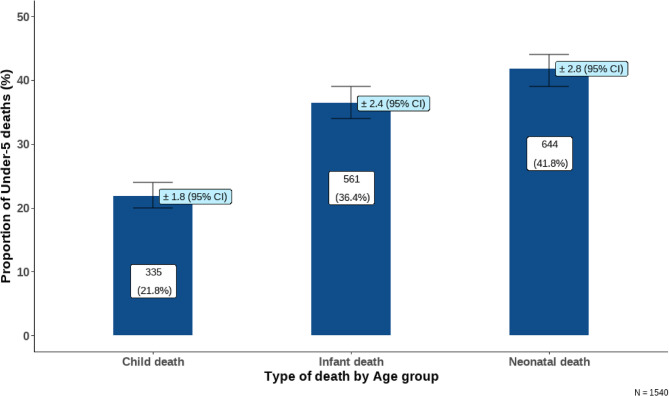 Figure 2
Figure 2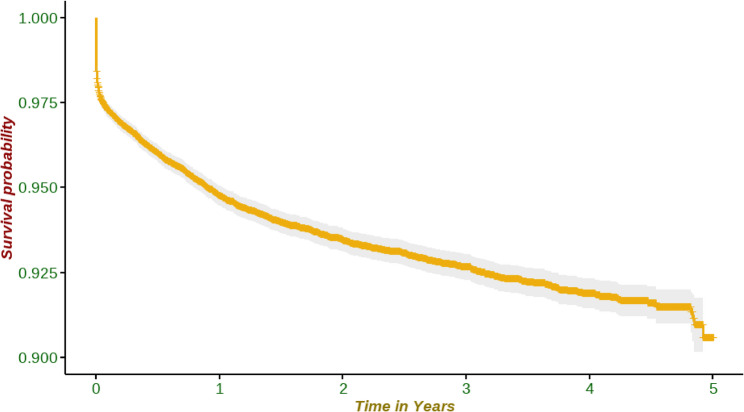 Figure 3
Figure 3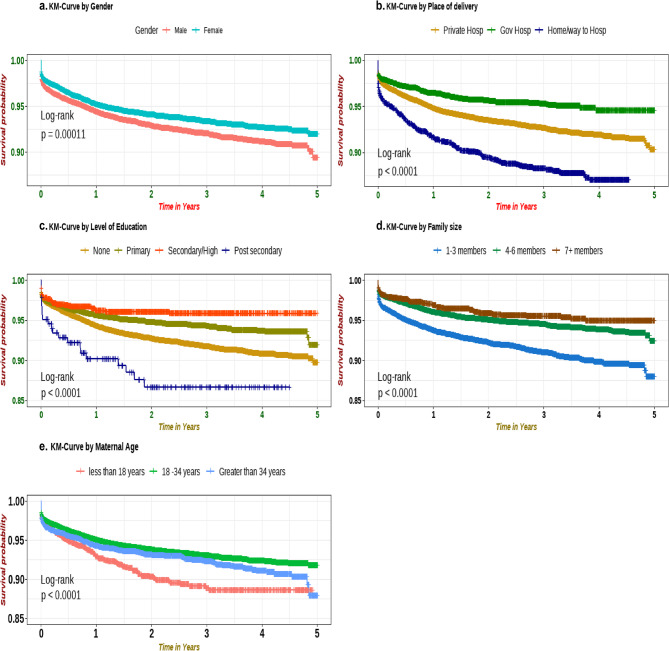 Figure 4
Figure 4- —https://doi.org/10.13039/100000865Bill and Melinda Gates Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Child Nutrition and Water Access · Health and Conflict Studies
Introduction
Under-five mortality remains a prominent issue of public health concern with most of the early childhood mortality being due to conditions that could be prevented or treated with access to simple and affordable interventions [1]. Globally, approximately 4.9 million deaths were reported among under-five children in 2022. Sub-Saharan Africa accounted for 56% of these, an increase from 50.2% in 2015 [2]. In Kenya, under-five mortality has significantly declined from 101.5 deaths per 1000 live births in 1990 to 41.6 deaths per 1000 live births in 2020, driven by improved health services, immunization, bed net use, and free maternal and child healthcare [3]. The country still falls short of the SDG targets, with persistent regional and income disparities impacting maternal and child mortality indicators in the 47 countries [4].
Several studies have revealed mixed findings on various predictors of child mortality [5–7]. High maternal and/or community-level illiteracy, multiple births, low birth weight, short birth interval, low socio-economic status of households, and healthcare facility access challenges have been known to increase mortality. This demonstrates a complex interplay of diverse multi-level factors in under-five mortality across Africa [8–10]. Most of these studies are cross-sectional designs, such as national surveys and mega-data analyses collected after 5 to 10 years or more [11–13]. Data from longitudinal studies have not been frequently employed although they may provide a better association between the exposure and the outcome, enabling a better understanding of causality and dynamic of risk factors over time. It also minimizes recall bias and allows for evaluating life course influence on child survival [14].
Studies have shown the survival rate among under-five to be more than 70%, with high mortality experienced during the early neonatal period [15, 16]. A study conducted in selected countries in Sub-Saharan using Health Demographic Survey data in 2018 demonstrated that the cumulative survival rate was 88.9% among children below the age of five [17]. However, there is a paucity of data on the survival probability among those under the age of five years in Siaya County. The study aimed to estimate the survival probability and predictors of under-five mortality in Siaya County, Western Kenya.
Methods
Study design
Siaya HDSS is a system of continuous longitudinal monitoring of demographic events in a geographically defined population, with timely production of data on all births, deaths, and migrations. HDSS rounds gather information on births, deaths, pregnancies, migrations, morbidity, parent survival status, immunization, educational status, religion, marital status, and ethnicity semiannually. HDSS collects verbal autopsy data to determine causes of death among the HDSS population. They use the collected data to regularly track and measure demographic and health dynamics, including birth rates, mortality rates, causes of death, sickness, migration, and socioeconomic indicators. It also serves as a platform to monitor infectious and non-infectious disease indicators and compute disease rates by providing accurate denominators [18]. This study used a retrospective longitudinal cohort study design. In order to answer the objective of this study, we retrospectively extracted data (between 2015 and 2020) from the existing DSS database with our event of interest being under-five mortality recorded within the scope of five years.
Study area
Siaya Health Demographic Surveillance System (HDSS) is located in Rarieda, Siaya, and Gem sub-counties in Siaya County, Western Kenya. The county is a malaria-endemic zone with a high HIV prevalence of 21% and an under-five mortality rate of 67.4 deaths per 1000 live births [19] which is more than the national average.
Data source
The study utilized secondary data from the HDSS dataset downloaded from the KEMRI server and maintained in the Microsoft SQL database at the KEMRI Center for Global Health Research in Kisumu. The KEMRI/CDC HDSS follows a population of approximately 256,000 individuals, 42% of whom are children. These residents live in 393 villages spread over 700 km2, in 64,317 households and 44,461 compounds. The HDSS population was visited twice annually during the study period and data on basic demographic and health information were collected by community health interviewers.
Study population
The study population for the analysis included all children under five years of age born within the study period and whose data was recorded in the Siaya HDSS database between 2015 and 2020. The child may be alive or dead at the time of the interview.
Inclusion and exclusion criteria
We included all children between 0 and 59 months who were recorded in the HDSS database between 2015 and 2020. We excluded children whose data were incomplete from the analysis.
Data management and analysis
The selection of covariates analyzed in this study was based on the associated literature review and the data missingness in the dataset. Exploratory data analysis was performed to evaluate the extent of missing values, identify potential outliers, and check for multicollinearity. Since children are the basic unit of analysis, data was transformed such that each child constituted a unit of observation. Follow-up time was censored to 59 months of age, death, or out-migration. Descriptive statistics were used to describe maternal and child characteristics. Cox bivariate proportional hazard model was fitted for outcomes against the predictors independently to identify the confounding and adjusted variables for the final model. A p-value of < 20% was used to identify the covariates to adjust for in the full model. Variables violating proportional hazard assumptions were excluded unless biologically plausible or supported by the literature. Covariates with > 10% missingness were excluded (Supplementary 1), while those with < 10% were imputed using the multivariate imputation by chain equation (MICE). The final Cox proportional hazards model included variables with p-values < 0.05 and biologically plausible factors, reporting hazard ratios (HRs) at p < 0.05. We conducted the analysis using R version 4.2.1.
Results
Descriptive statistics of the study population
A total of 24,452 children were observed during the study period, we excluded 7 children whose data was incomplete due to incomplete interviews. Most of the population was aged between 1 year to < 5 years (Fig. 1). At the end of the follow-up, 1540 (6.3%) deaths were recorded, or 63 deaths per 1000 live births. The age distribution of participants is shown in Fig. 1 and deaths in Fig. 2, respectively. Different age clusters classified under-five child mortality as neonatal deaths (0–28 days), infant deaths (28 days to < 1 year), and child deaths - deaths between 1 year to < 5 years of age (Fig. 2).Fig. 1. Distribution of under-five children by age group in HDSS, Siaya County, Kenya from 2015 to 2020Fig. 2Deaths among children by age group in HDSS, Siaya County, Kenya from 2015 to 2020
The male to female ratio was 1:1. Among children born to mothers under 18 years of age, 43.8% out-migrated, while 8.1% experienced under-five mortality. Under-five mortality was observed in 10.2% of children whose mothers received no antenatal care (ANC) and 8.1% of those whose mothers attended only one ANC visit. Additionally, 10% of children born at home or on the way to the hospital experienced under-five mortality. 12% of children born to mothers with no formal education experienced under-five mortality (Table 1).Table 1. Under-five mortality by basic epidemiological and healthcare-related factors among participants in Siaya County, Kenya using HDSS data from 2015–2020CharacteristicOverall,n (%)Alive, n(%)Outmigration,n(%)Under-five Mortality,n(%)Total24,452 (100)16,914 (69.2)5,998 (24.5)1540 (6.3)Gender Male12,341 (100)8,556 (69.3)2,933 (23.8)852 (6.9) Female12,111 (100)8,358 (69.0)3,065 (25.3)688 (5.7)Maternal age Less than 18 years1,809 (100)869 (48.0)793 (43.8)147 (8.1) 18–34 years19,075 (100)12,984 (68.1)4,951 (26.0)1,140 (6.0) Greater than 34 years3,568 (100)3,061 (85.8)254 (7.1)253 (7.1)Family size 1–3 members7,365 (100)4,539 (61.6)2,272 (30.8)554 (7.5) 4–6 members11,755 (100)10,421 (88.7)750 (6.4)584 (5.0) 7 + members1,964 (100)1,792 (91.2)93 (4.7)79 (4.0)Wealth Index 1 st quantile3,710 (100)2,360 (63.6)1,092 (29.4)258 (7.0) 2nd quantile4,200 (100)2,936 (69.9)994 (23.7)270 (6.4) 3rd quantile4,164 (100)2,903 (69.7)1,016 (24.4)245 (5.9) 4th quantile3,889 (100)2,747 (70.6)901 (23.2)241 (6.2) 5th quantile3,753 (100)2,537 (67.6)1,006 (26.8)210 (5.6)Place of birth Home/way to hospital2,131 (100)1,355 (63.6)543 (25.5)233 (10.9) Private hospital4,087 (100)3,095 (75.7)821 (20.1)171 (4.2) Government hospital18,189 (100)12,438 (68.4)4,619 (25.4)1,132 (6.2)Place of ANC Visit Gov. Dispensary2,813 (100)2,218 (78.8)473 (16.8)122 (4.3) Gov. Health center3,916 (100)3,042 (77.7)718 (18.3)156 (4.0) Gov. Hospital15,539 (100)10,171 (65.5)4,229 (27.2)1,139 (7.3) Home13 (100)9 (69.2)2 (15.4)2 (15.4) Private/mission1,239 (100)978 (78.9)215 (17.4)46 (3.7) Others8 (100)7 (87.5)1 (12.5)0 (0.0)ANC Times None108 (100)63 (58.3)34 (31.5)11 (10.2) One689 (100)450 (65.3)183 (26.6)56 (8.1) Two1,893 (100)1,263 (66.7)466 (24.6)164 (8.7) Three5,351 (100)3,740 (69.9)1,288 (24.1)323 (6.0) Above 414,731 (100)10,468 (71.1)3,407 (23.1)856 (5.8)Maternal Education level None184 (100)129 (70.1)33 (17.9)22 (12.0) Primary15,168 (100)10,690 (70.5)3,393 (22.4)1,085 (7.2) Secondary/high7,629 (100)5,077 (66.5)2,178 (28.5)374 (4.9) Post-secondary1,334 (100)918 (68.8)366 (27.4)50 (3.7)Religion Protestants4,246 (100)2,886 (68.0)1,122 (26.4)238 (5.6) Catholic5,584 (100)3,815 (68.3)1,441 (25.8)328 (5.9) Roho/legio maria5,120 (100)3,587 (70.1)1,174 (22.9)359 (7.0) Others9,181 (100)6,379 (69.5)2,210 (24.1)592 (6.4)Source of Water Protected water7,465 (100)5,077 (68.0)1,937 (25.9)451 (6.0) Unprotected water16,884 (100)11,767 (69.7)4,036 (23.9)1,081 (6.4)Water for Drinking Tap water4,306 (100)2,935 (68.2)1,122 (26.1)249 (5.8) Lake/river6,094 (100)4,250 (69.7)1,396 (22.9)448 (7.4) Rainfall,3,986 (100)2,833 (71.1)952 (23.9)201 (5.0) Unprotected spring/borehole/well6,117 (100)4,209 (68.8)1,510 (24.7)398 (6.5) Protected spring3,159 (100)2,142 (67.8)815 (25.8)202 (6.4)Distance to Water Source In compound4,985 (100)3,514 (70.5)1,231 (24.7)240 (4.8) < 500 m13,976 (100)9,721 (69.6)3,342 (23.9)913 (6.5) 500 m-2 km4,783 (100)3,189 (66.7)1,251 (26.2)343 (7.2) 2–5 km186 (100)131 (70.4)42 (22.6)13 (7.0) > 5 km10 (100)5 (50.0)5 (50.0)0 (0.0) Dk291 (100)204 (70.1)71 (24.4)16 (5.5)Cooking methods Charcoal/firewood23,915 (100)16,559 (69.2)5,837 (24.4)1,519 (6.4) Gas/paraffin/stove537 (100)355 (66.1)161 (30.0)21 (3.9)Toilet type Neighbor/no facility/bush2,375 (100)1,590 (66.9)584 (24.6)201 (8.5) Modern latrine1,936 (100)1,302 (67.3)548 (28.3)86 (4.4) Traditional pit19,921 (100)13,873 (69.6)4,810 (24.1)1,238 (6.2) Birth assistance Nurse/midwife/doctor/chw22,870 (100)15,926 (69.6)5,584 (24.4)1,360 (5.9) Traditional birth attendant1,548 (100)970 (62.7)401 (25.9)177 (11.4)HDSS Health Demographic Surveillence System ^1^ n, Mean (SD) ^2^ n (%)
Survival probability of children under five years in Siaya County
The cumulative survival probability within the first five years was approximately 90% among the children born in the study area (Fig. 3).Fig. 3. Survival probability of children under five in Siaya County using 2015–2020 HDSS data
Kaplan-Meier curve estimate
We estimated the survival probability of children under the age of five years using the Kaplan-Meier curve estimate **(**Fig. 4a **– **e). The analysis of the Kaplan-Meier curves demonstrated that under-five children who are male, not delivered to hospitals, families with 1–3 members, advanced and young maternal age, and no maternal education have lower survival rates than the comparison group.Fig. 4. Kaplan Meier estimates showing child survival by selected epidemiological and health-related factors of participants in Siaya County, Kenya, using HDSS data from 2015 to 2020
Results of the multivariable analysis
Children who were female were 18% more likely to die compared to males (aHR 0.82; 95% CI 0.74–0.82) (Table 2). Children born to mothers with no education and primary education had a higher risk of death (aHR 1.29; 95% CI 1.14, 1.47) and (aHR 1.93; 95% CI 1.19,3.10), respectively. In addition, children born to mothers aged below < 18 years had a higher risk for mortality (aHR = 01.34; 95% CI 1.11, 1.62). Place of birth (aHR 1.5; 95% CI 1.29,1.77), ANC visits (aHR 2.1; 95% CI 1.14, 3.87), and type of latrine (aHR 1.22; 95% CI 1.04, 1.43) were also associated with childhood mortality.Table 2. Cox proportional hazard model to identify factors associated with childhood mortality in Siaya County, Kenya using HDSS data 2015–2020Risk factorsCrude Hazard Ratio**Adjusted Hazard RatioHR^1^95% CI^1^HR^1^95% CI^1^Maternal Level of Education Primary1—1— Secondary/High0.730.65, 0.820.770.68, 0.88 Post Secondary0.550.41, 0.730.590.43, 0.82* None1.731.14, 2.641.490.93, 2.37Maternal Age 18–34 years1—1— less than 18 years1.491.26, 1.771.341.11, 1.62 Greater than 34 years1.161.01, 1.331.040.90, 1.21Number of ANC visits Above 41—1— None2.161.19, 3.932.11.14, 3.87 One1.31.0, 1.701.110.84, 1.47 Two1.41.18, 1.651.261.06, 1.49 Three0.990.87, 1.120.940.83, 1.07Place of birth Government Hospital1—1— Private hospital0.660.56, 0.780.70.60, 0.83 Home/way to Hospital1.631.41, 1.871.511.29, 1.77 Method of cooking Charcoal/Firewood1—1— Gas/Paraffin/Stove0.650.42, 1.010.820.50, 1.32Toilet type Traditional pit1—1— Modern latrine0.720.57, 0.890.840.67, 1.06 Neighbor -No facility/Bush/field1.341.15, 1.551.221.04, 1.43Child Gender Male1—1— Female0.820.74, 0.910.820.74, 0.91n* = 22,441; N events = 1,390; statistic.log = 158; p.value.log = 0.000; statistic.sc = 165; p.value.sc = 0.000; statistic.wald = 172; p.value.wald = 0.000; statistic.robust = 153; p.value.robust = 0.000; R² = 0.007; r.squared.max = 0.702; c-index = 0.592; c-index SE = 0.008; Log-likelihood = −13,494; AIC = 27,019; BIC = 27,098; No. Obs. = 22,441^1^ *HR *Hazard Ratio, *CI *Confidence Interval
Discussion
We observed that one in sixteen children died before the age of five in Western Kenya, a rate higher than the national average of one in twenty-four children. Maternal age, maternal education, number of ANC visits, toilet type, place of delivery, and gender were associated with childhood mortality. The overall cumulative survival probability of children was approximately above 90%, with the highest risk of death during the first month of life.
The high risk of death in the first month of life is consistent with findings from studies in Ethiopia and Nigeria [15, 20]. This may be attributed to factors such as low immunity and adverse fetal outcomes, including prematurity, birth asphyxia, and low birth weight, which play a crucial role in the susceptibility of neonates to preventable diseases [21]. Male infants were found to have a higher risk of dying before the age of 5 years compared to females, consistent with findings from other studies in LMICs [8, 22, 23]. This disparity could be due to the biological and genetic differences that make them more susceptible to many diseases that cause death [24]. Male children also exhibit lower disease resistance and greater vulnerability to complications of prematurity, contributing to a higher hazard risk of death [25].
Our findings revealed a significant association between maternal age and child survival, consistent with findings in previous studies [26]. Mothers with an age below 18 were at higher risk of child mortality, potentially due to their incomplete physical development, which can increase complications during pregnancy and childbirth [27]. Young mothers are also more likely to experience stigma, lower socioeconomic status, and lower educational attainment, all of which may negatively impact their health-seeking behavior and access to health services [28]. Furthermore, observed high outmigration among young mothers may have influenced the observed outcomes, as these mothers often relocate in search of better opportunities or due to social pressures, potentially disrupting continuity of care and access to critical maternal and child health services.
The observed lower under-five mortality rate among children born to mothers with higher education highlights the positive impact of maternal education on child survival outcomes, a finding consistent with previous studies [29, 30]. Studies suggest that educated mothers often have greater health literacy, enabling them to access health services earlier and make informed decisions about their child’s health [31, 32]. They are also more likely to be knowledgeable about various modern contraceptives, timely vaccination, proper hygiene, and proper nutrition, all of which contribute to improved child survival rates [12]. Educated mothers are often employed, providing them greater financial flexibility and independence to afford quality health care and seek treatment at well-equipped health facilities or with specialized doctors [33].
In this study, delivery in a health facility was significantly associated with lower child mortality, consistent with findings from other studies [34, 35]. Lower mortality among children born in health facilities may be attributed to comprehensive healthcare services provided to women and their children during labor and the postpartum period, as well as higher utilization of maternity services [36]. The WHO recommends a minimum of four visits during pregnancy, with the first visit in the first trimester [37]. In this study, children of mothers who attended fewer ANC visits faced a greater risk of death, aligning with results from a study in Ethiopia [16]. This positive impact of ANC services may be due to skilled healthcare workers educating mothers on pregnancy danger signs during routine checkups and administering routine vaccinations [38].
Household access to latrines was also associated with improved child survival, consistent with findings from other studies [39, 40]. This improvement in survival may be attributed to the health benefits of reduced exposure to human excreta, as shared or inadequately managed toilets can contribute to the spread of diseases and increased child mortality [41, 42]. In contrast, we found no significant association between the source of cooking fuel and under-five mortality, which diverges from most previous findings [43, 44]. The differences in the outcome may be attributed to the study setting, sample size, and geographical factors.
Our analysis has several strengths and limitations. The huge dataset provided valuable information for understanding under-five mortality and its predictors in Siaya County between 2015 and 2020. While the study did not utilize the national-level data, the study has highlighted a higher number of under-five deaths and is representative of population-level data. Limitations of this study include the potential biases or inaccuracies inherent in secondary data sources and Karemo HDSS’s use of a consecutive sampling approach, which excludes non-resident households, leading to selection bias. Additionally, some key variables were not included in the final analysis due to missing data, which may have affected the robustness of our findings and the generalizability of the results. The DIP in the final year of the survival curve coincides with the COVID-19 outbreak and could be attributed to multiple factors. The pandemic disrupted routine data collection, leading to underreporting or delays in recording cases. Additionally, health system disruptions, changes in healthcare-seeking behavior, and shifts in disease patterns due to COVID-19 mitigation measures might have influenced the numbers. Lastly, the extended follow-up period led to out-migration, which may have biased the estimates of mortality risk factors in this longitudinal study.
Conclusion
Under-five mortality in Siaya County was markedly high at 63 deaths per 1,000 live births, significantly exceeding the national rate of 41.6 deaths per 1,000 live births. The risk of death was highest among the early neonates and declined with increasing age. Child death was more common among children of young mothers, mothers with no or low level of education, low Antenatal care (ANC) coverage, home deliveries, and households without access to latrines.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arora A, UNICEF DATA. 2024 [cited 2024 Oct 9]. Levels and trends in child mortality. Available from: https://data.unicef.org/resources/levels-and-trends-in-child-mortality-2024/
- 2Ettarh R, Kimani J. Determinants of under-five mortality in rural and urban Kenya. RRH [Internet]. 2012 Mar 13 [cited 2023 Aug 2]; Available from: https://www.rrh.org.au/journal/article/181222417123 · pubmed ↗
- 3Chapter 7. Longitudinal studies [Internet]. [cited 2024 Dec 9]. Available from: https://www.bmj.com/about-bmj/resources-readers/publications/epidemiology-uninitiated/7-longitudinal-studies
- 4Bado AR, Sathiya Susuman A. Women’s Education and Health Inequalities in Under-Five Mortality in Selected Sub-Saharan African Countries, 1990–2015. Carpenter DO, editor. P Lo S ONE. 2016;11(7):e 0159186.10.1371/journal.pone.0159186 PMC 495610927442118 · doi ↗ · pubmed ↗
- 5WHO. 2018. Definition of skilled health personnel providing care during childbirth: the 2018 joint statement by WHO, UNFPA, UNICEF, ICM, ICN, FIGO and IPA [Internet]. 2018. Available from: www.unfpa.org/sowmy
- 6Gage AD, Fink G, Ataguba JE, Kruk ME. Hospital delivery and neonatal mortality in 37 countries in sub-Saharan Africa and South Asia: An ecological study. Myers JE, editor. P Lo S Med. 2021;18(12):e 1003843.10.1371/journal.pmed.1003843 PMC 863539834851947 · doi ↗ · pubmed ↗
- 7WHO-RHR-18. 02-eng.pdf [Internet]. [cited 2024 Sep 30]. Available from: https://iris.who.int/bitstream/handle/10665/259947/WHO-RHR-18.02-eng.pdf
- 8Motsima T, Zuma K, Rapoo E. Levels and trends of Under-Five mortality in South Africa from 1998 to 2012. International Journal of Medical and Health Sciences. 2020;14(5). https://www.researchgate.net/publication/358348859_Levels_and_Trends_of_Under-Five_Mortality_In_South_Africa_from_1998_to_2012.